OB week 4
1/370
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
371 Terms
Characteristics of contractions include?
coordinated, involuntary, intermittent
Contractions throughout pregnancy feel like?
uncoordinated and low intensity
Contractions at the end of pregnancy feel like?
organized and gradually assume a regular pattern of increasing frequency
Frequency
period from the beginning of one uterine contraction to the beginning of the next
Duration
period from the beginning of a uterine contraction to the end of the same contraction
Intensity
strength of a contraction during labor
Where do coordinated uterine contractions begin?
start in the uterine fundus and spread downward toward the cervix to propel the fetus through the pelvis
The contraction cycle consists of?
-increment
-peak
-decrement
Increment
period of increasing strength
Peak
period when the contraction is the most intense
Decrement
period of decreasing intensity as the uterus relaxes
Interval
"relaxation time" period between the end of one contraction and the beginning of the next
Resting tone
the degree of uterine tension between contractions and is described as either soft/relaxed or firm
How does the uterine muscle function during labor/contractions?
-upper 2/3 of uterus contracts actively to push the fetus down
-lower 3rd of uterus remains less active, promoting downward passage of the fetus
Cervical changes during labor
effacement and dilation
Effacement
thinning and shortening of the cervix
Dilation
opening of the cervix from 0-10 cm
Presenting part
the part of the fetal body that enters the pelvis first
Cardiovascular changes during labor
-muscle fibers in the uterus around spiral arteries constrict and shunts 300-500 mL of blood back into systemic circulation
-causes increase in blood volume
-slight increase in bp, slight decrease in pulse
-vitals signs best taken between contractions
-hypotension can occur if supine
Respiratory system changes during labor
-depth/rate of respirations increase
-can cause respiratory alkalosis
-can result in numbness/tingling/dizziness if hyperventilating
GI system changes during labor
-gastric motility is reduced
-N/V
-solid food is contraindicated
-ice chips, popsicles, juices, broth in moderate amounts
Urinary system changes during labor
-reduced sensation of a full bladder
-full bladder can inhibit fetal descent of presenting part due to occupying space in the pelvis
-distended bladder increases risk of bladder hypotonia/infection
Hematopoietic system changes during labor
-500 to 1000mL of blood loss is normal
-leukocyte count is 20,000-30,000
-fibrinogen is elevated
Fetal protective mechanisms during contractions
-fetal Hgb more readily takes on oxygen and releases CO2
-high Hgb and Hct levels carry more O2 than adult
-higher cardiac output
Function of catecholamines in the newborn
-primarily epi/norepi
-produced by fetal adrenal glands in response to stress of labor
-stimulate cardiac contraction/breathing, quicken the clearance of remaining lung fluid, aid in temperature regulation
What are the 4 P's?
-powers
-passage
-passenger
-psyche
Power during the 1st stage of labor
uterine contractions are the primary force moving the fetus through the pelvis
Second stage of labor consists of?
-full cervical dilation to birth of the baby
-client feels an urge to push and bears down
Passage
-birth passage consists of the pelvis and soft tissues
-softening of the cartilage linking the pelvic bones occurs near term because of increased levels of relaxin
What is the passenger?
consists of the fetus, membranes, and placenta
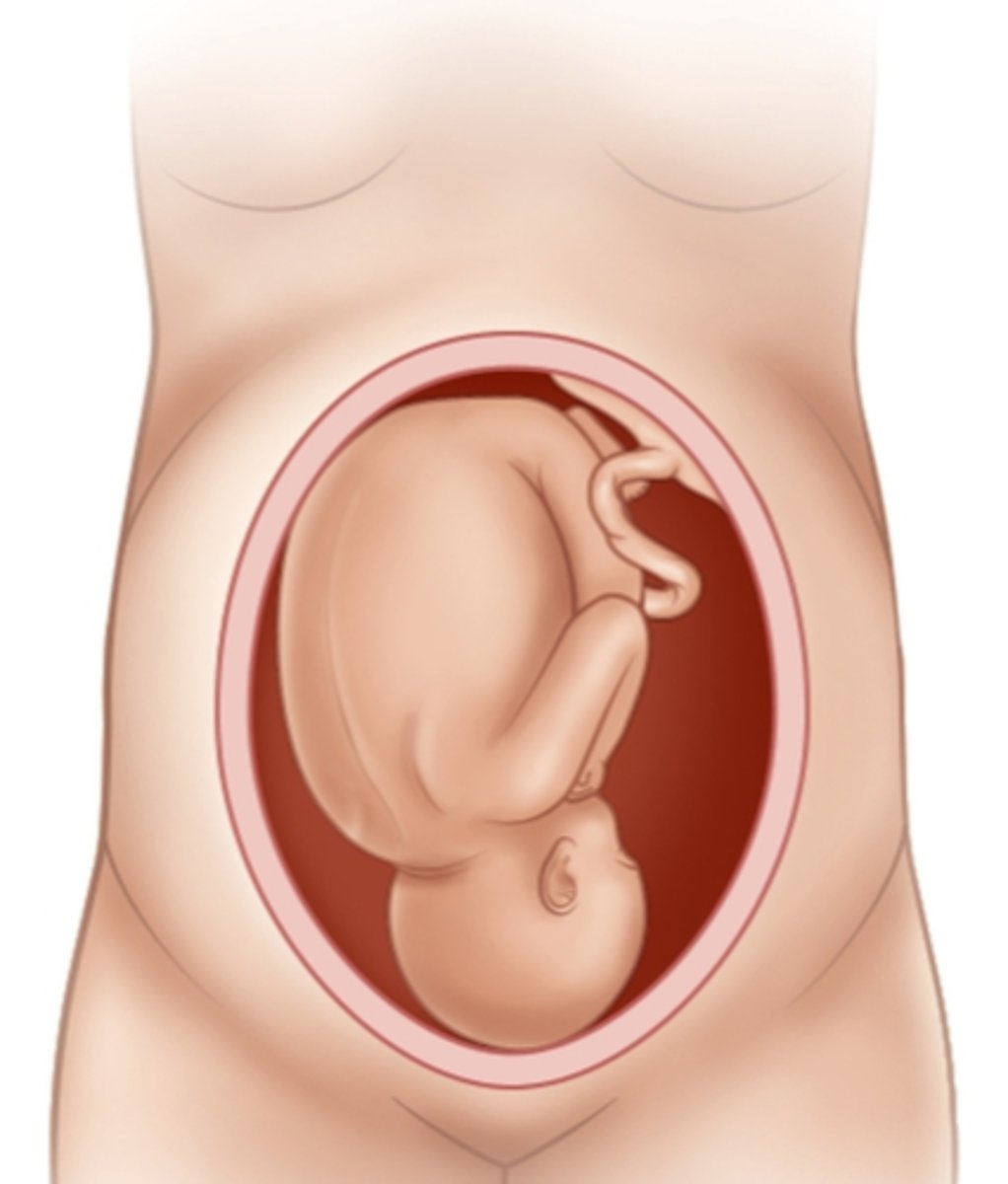
Cephalic presentation
birth position where the head enters the birth canal first
Adaptations of the fetal head for birth
the sutures/fontanels allows the bones to move slightly, changing the shape of the fetal head so it can adapt to the size of the pelvis by molding
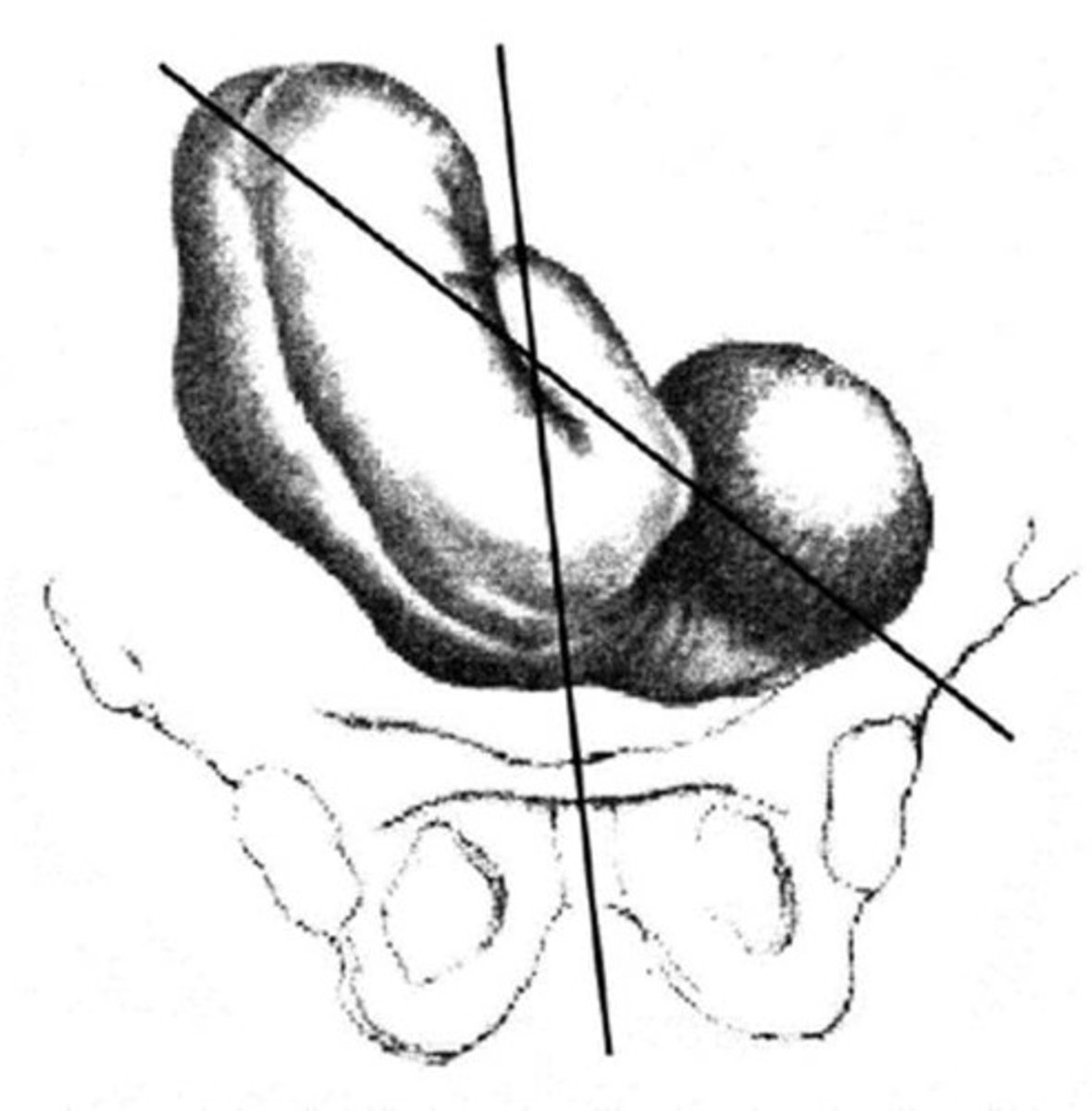
Fetal lie
the orientation of the long axis (spine) of the fetus to the long axis (spine) of the mom
Longitudinal fetal lie
-most common
-either the head or buttocks of the fetus enter the pelvis first
-lie is longitudinal and parallel to the mom
Transverse fetal lie
the long axis of the fetus is at a right angle to the clients long axis

Attitude
the relation of fetal body parts to one another
Normal attitude
-flexion
-head flexed toward the chest and the arms/legs flexed over the thorax
-back is curved in a convex C-shape

Extension attitude
-abnormal
-head is extended away from the fetal chest

Oblique fetal lie
an angle between the longitudinal lie and transverse lie
Types of fetal presentation
-cephalic
-breech
-shoulder
Cephalic presentation: vertex
-fetal head is fully flexed
-most favorable
Cephalic presentation: military
head is in neutral position, neither flexed nor extended
Cephalic presentation: Brow
fetal head is partly extended
Cephalic presentation: Face
head is extended, and the fetal occiput is near the fetal spine
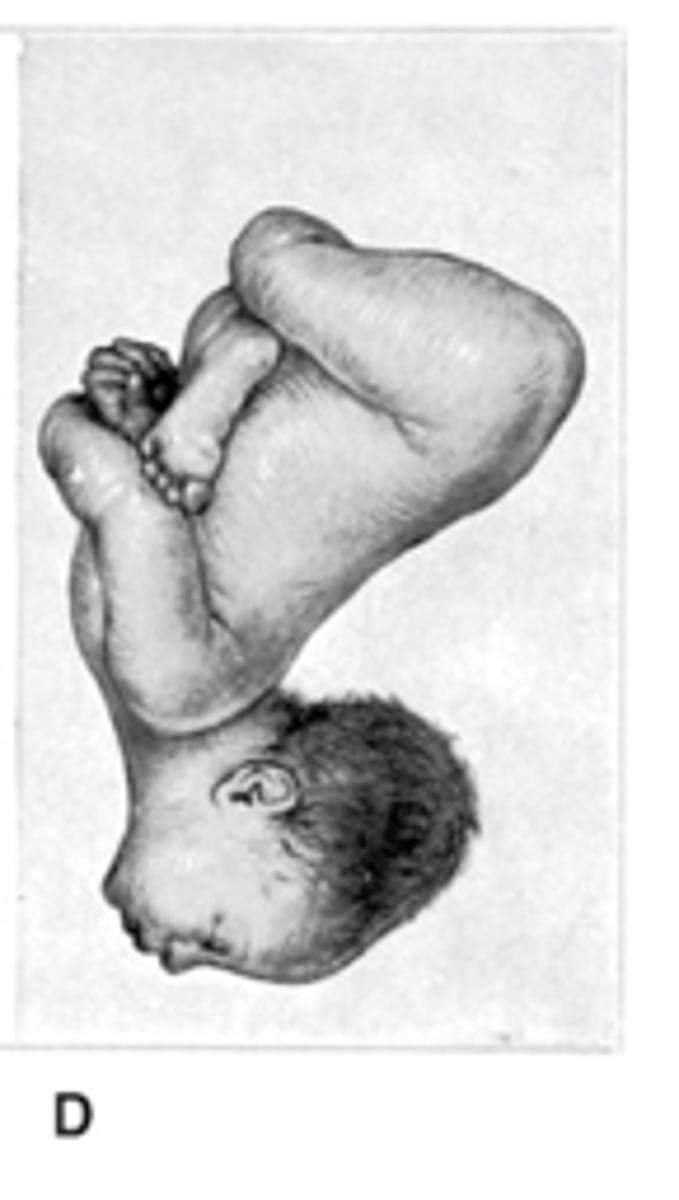
What is breech position?
fetal buttocks or legs enter the pelvis first
What conditions cause breech to occur more often?
-preterm births
-hydrocephaly
-multiple gestations
-abnormalities of the uterus/pelvis
-prior breech delivery
-placenta previa
Frank breech
fetal legs are extended across the abdomen toward the shoulders
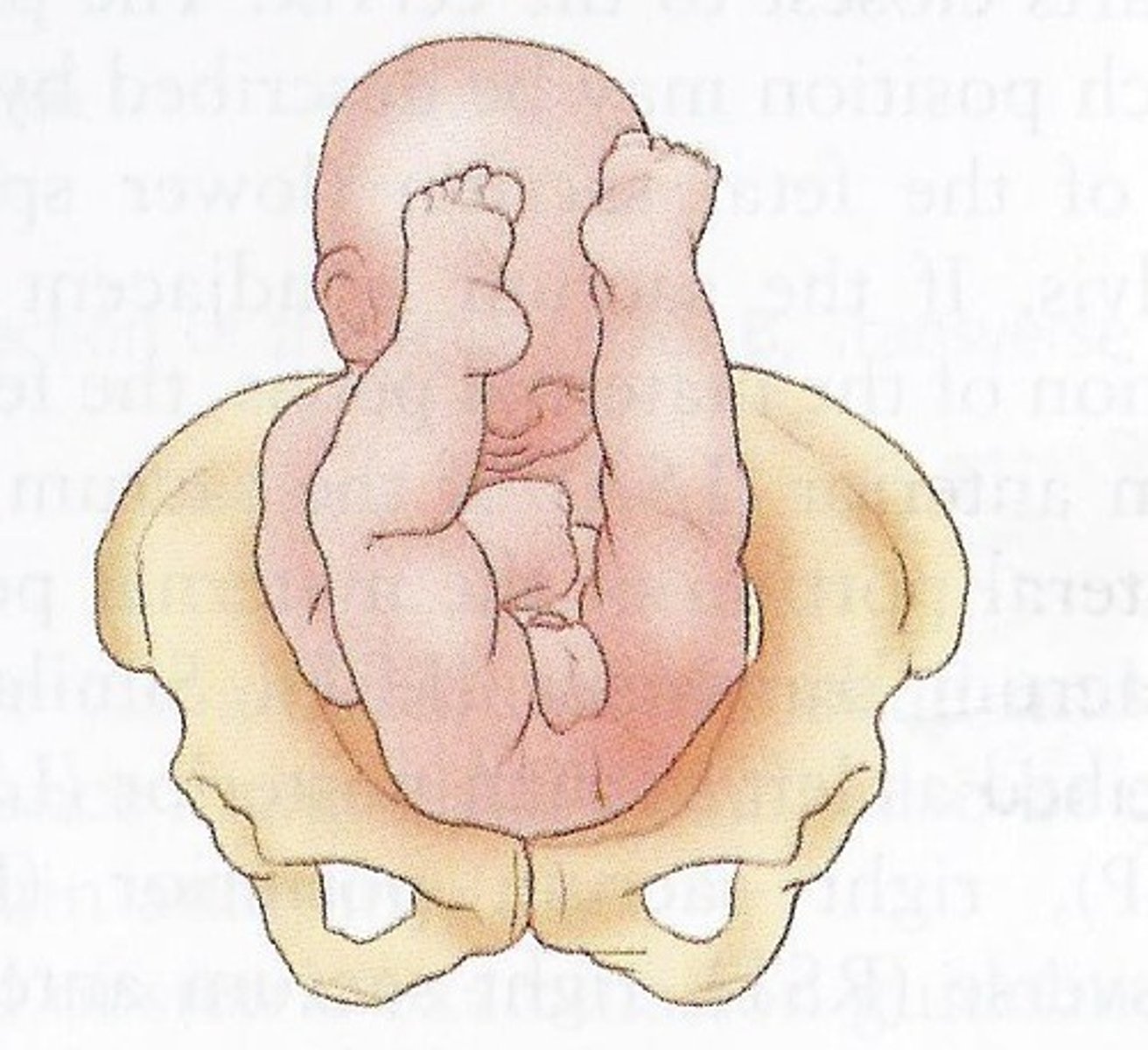
Complete breech
-reversal of cephalic presentation
-head, knees, hips are flexed

Footling breech
occurs when one or both feet are presenting

A shoulder presentation most often occurs with?
preterm gestation, high parity, hydramnios, placenta previa, abnormal uterine anatomy
Hormonal changes that cause the onset of labor
-estrogen increases and progesterone decreases
-protaglandins/oxytocin increase uterine sensitivity maintaining contractions
Braxton Hicks contractions
irregular, mild uterine contractions that occur throughout pregnancy and become stronger in the last trimester
Effects of lightening
-this occurs 2-3 wks before the natural onset of labor
-fetus descends to pelvic inlet and breathing becomes easier
-increased pressure on bladder causing more frequent urination
-increased pressure on pelvis causes leg cramps/edema
Vaginal secretions before/during labor
increase in clear/non-irritating secretions occur as fetal pressure causes congestion. of the vaginal mucosa
Ripening
cervix softens due to the release of relaxin allowing it to yield more easily to the forces of labor contractions
How to determine between false and true labor
-the absence of cervical changes including dilation and effacement
False labor characteristics
-contractions are inconsistent in frequency, duration, intensity
-contractions do not change or may decrease w/ activity
-felt in the abdomen or groin
-can be more annoying than painful
-cervix does not change effacement/dilation
True labor characteristics
-contractions are consistent or regular pattern of increasing frequency, duration, intensity
-contractions increase with activity
-felt in lower back and gradually sweeps around to lower abdomen
-can persist as back pain
-can resemble menstrual cramps during early labor
-progressive effacement/dilation
What occurs during the 1st stage of labor?
cervical effacement and dilation
Latent phase dilation
0-5cm
Active phase dilation
6-10cm
Forces during 1st stage of labor
uterine contractions
Uterine contraction characteristics in the 1st stage of labor
-initially mild/infrequent
-gradually progresses to strong intensity
-3 to 5 contractions in a 10 min period
Discomforts in 1st stage of labor
-low backache
-sensations similar to menstrual cramps
-back discomfort gradually sweeps to lower abdomen in a girdle-like fashion
-discomfort intensifies as labor progresses
Client behaviors in 1st stage of labor
-sociable, excited, can be anxious
-focus increases as labor intensifies
Work accomplished in 2nd stage of labor
expulsion of fetus
Forces during 2nd stage of labor
uterine contractions and voluntary bearing-down efforts
Cervical dilation in 2nd stage of labor
10 cm (complete)
Uterine contraction characteristics in 2nd stage of labor
-strong, 5-6 contractions in 10 min period
-may be slightly less intense than during late first stage
-can pause briefly before stage begins
Discomforts in 2nd stage of labor
-urge to push or bear down w/ contractions
-distention of vagina/vulva may cause stretching or splitting sensation
Client behaviors in 2nd stage of labor
-intense concentration on pushing with contractions
-often oblivious to surroundings and appears to doze between contractions
Work accomplished in 3rd stage of labor
separation of placenta
Force in 3rd stage of labor
uterine contractions
Uterine contractions in 3rd stage of labor
firmly contracted
Discomforts in 3rd stage of labor
-little discomfort
-sometimes slight cramp is felt as placenta is passed
Client behaviors in 3rd stage of labor
-excited/relieved after baby's birth
-usually tired/cries
Work accomplished in 4th stage of labor
physical recovery and bonding w/ newborn
Force in 4th stage of labor
uterine contraction to control bleeding from the placental site
Uterine contractions in 4th stage of labor
firmly contracted
Discomforts in 4th stage of labor
-discomfort can vary
-can have afterpains if they are multigavida or have had a large baby
-perineal discomfort
Client behaviors in 4th stage of labor
tired by may find it difficult to rest because of excitement, eager to become acquainted w/ the newborn
Sources of pain during labor
-tissue ischemia
-cervical dilation
-pressure/pulling on pelvic structures
-distention of the vagina/perineum
How does tissue ischemia pain occur during labor?
blood supply to uterus decreases during contractions, leading to tissue hypoxia and anaerobic metabolism
How does cervical dilation pain occur during labor?
dilation and stretching of the lower uterus are major sources of pain that travel through SC levels T10, T11, T12, L1
How does pressure/pulling on pelvic structure pain occur during labor?
visceral pain that is in the pelvic structures, ligaments, fallopian tubes, ovaries, bladder, perineum and can be referred to back and legs
How does distention of the vagina/perineum pain occur during labor?
-occurs during fetal descent
-feels like burning, tearing, splitting
Factors influencing perception or tolerance of pain
-labor intensity (precipitous labor has more severe/faster onset of pain)
-cervical readiness
-fetal position (occiput posterior causes back labor)
-pelvic anatomy
-fatigue
When is the ideal time to prepare for non pharmacologic pain control?
before labor, during the last trimester
What does relaxation promote during labor?
-promotes uterine blood flow, improve fetal oxygenation
-promotes efficient uterine contractions
-reduces tension, which decreases pain perception and increases pain tolerance
-reduces tension, can facilitate fetal descent
Progressive relaxation
the client contracts and then releases specific muscle groups until all muscles are released
Neuromuscular dissociation
helps the client learn to release all muscles except those that are working
Relaxation against pain
the partner deliberately causes mild pain and the client learns to release and relax despite the pain
Massage benefits during labor
increases the release of endorphins, promotes circulation, reduces muscle tension
Effleurage
clients may rub their abdomen or legs during labor to counteract discomfort
Thermal stimulation for pain during labor
-warmth increases oxytocin release and local blood flow, relaxes muscles, raises the pain threshold
-cool, damp washcloth placed on forehead, throat, lower abdomen can provide comforting coolness if client feels hot
Double-hip squeeze
support person provides counter pressure, which counteracts the painful perception of labor
Hydrotherapy for pain
-shower, tub bath, whirlpool bath is relaxing and provides thermal stimulation
-buoyancy afforded by immersion supports and equalizes pressure on the body/aids muscle relaxation
-causes fluid to shift from extravascular space to the intravascular space, reducing edema as the excess fluid is excreted by the kidneys
What do breathing techniques do during pain?
PNS releases anti stress hormones like acetylcholine, prolactin, oxytocin, and vasopressin, helping a client to stay calm and relaxed
What is a cleansing breath?
-each contraction begins and ends w/ a deep inspiration and expiration
-provided O2 to help reduce myometrial hypoxia
-helps clients clear their mind to focus on relaxing and signals their labor partner the contraction is beginning or ending
What is slow-paced breathing?
-increases relaxation
-lowers HR/BP
-redirects blood flow away from the locomotive muscles and toward the digestive/reproductive organs
-increases the release of endorphins, activating the immune system/creating sleepiness "dream-like" state
-used as long as possible because it promotes relaxation/oxygenation