Intraoral Image Technique and Projection Geometry
1/25
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
26 Terms
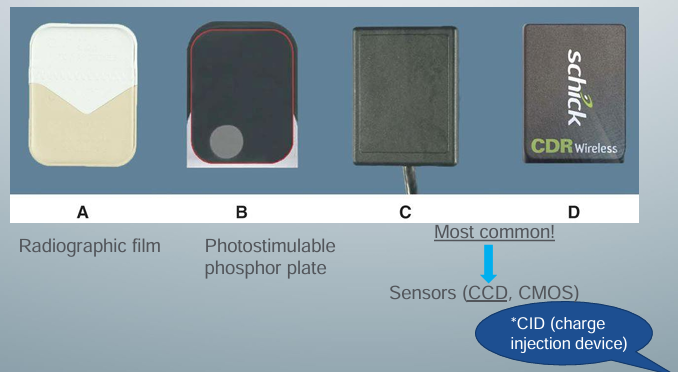
control panel and image receptors
-all units have a control panel (chooses pt’s size, tooth, or teeth location)
-choose a sensor
intraoral unit
-consists of x-ray tube housing and position-indicating device (aiming cylinder)
-unit has a control panel usually outside the room
-on control panel, can chance radiographic exposure settings such as voltage, current, and exposure time by choosing the proper size of the patient and teeth location
-if correct setting not chosen, image will be too faint or dark
-images should have optimal density and contrast for interpretation
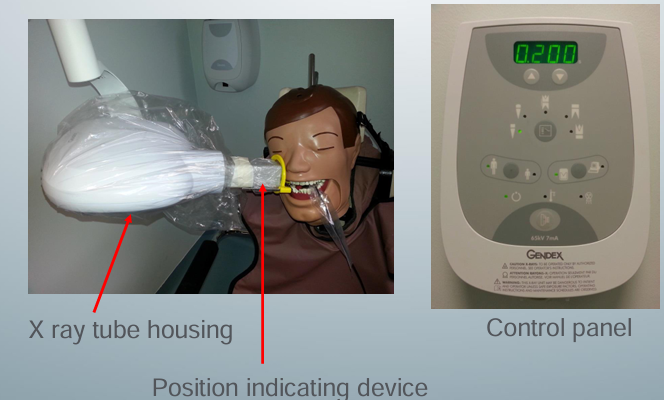
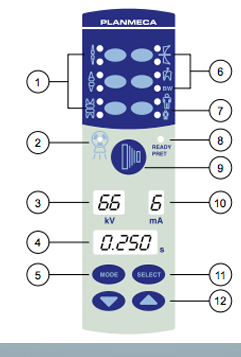
control panel
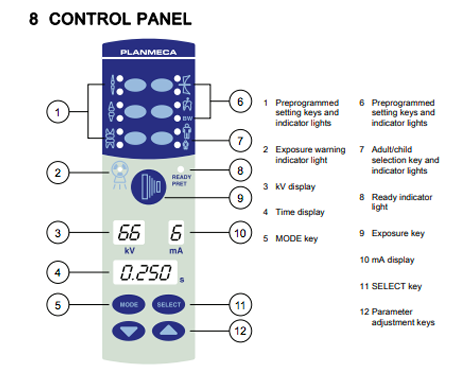
image receptors
-4 sizes for intraoral views
-mainly use size 2 for PA and BW
-sizes 0 and 1 for kids
-no occlusal sensors because they are too expensive
-choose size that will capture the site of interest in its entirety
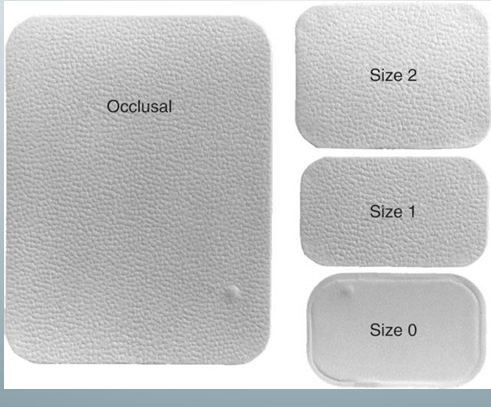
image receptors
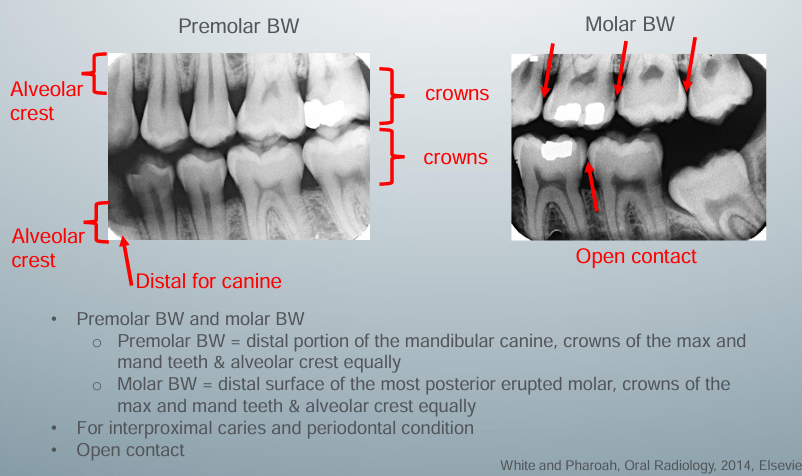
intraoral imaging- FMS
-3 anteriors, 4 posteriors for each jaw, 2 pairs of BWs
-intraoral images are the highest spatial resolution of all imaging modalities available, including CBCT
-can investigate detailed periodontium such as: extent of dental caries, presence and extent of PA inflammation, consequences of traumatic injuries, periodontal bone loss, unerupted and impacted teeth evaluation, external and internal root resorption, assess pulp morphology, determine length of endodontic instrumentation during treatment
position and distance rule
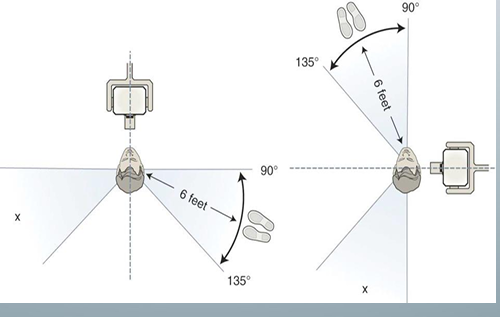
-ideal way to protect self from x-ray exposure: leave the room and hide behind a wall when taking radiographs
-operator may be exposed to leakage radiation from the x-ray tube head, scattered radiation from the patient, and primary photons passing through the patient
-if there is no wall between the patient exposure area, stand at least 6 ft from the pt at an angle of 90-135 degrees to x-ray beam
-never hold image receptors in the pt’s mouth and never hold the x-ray unit during exposure
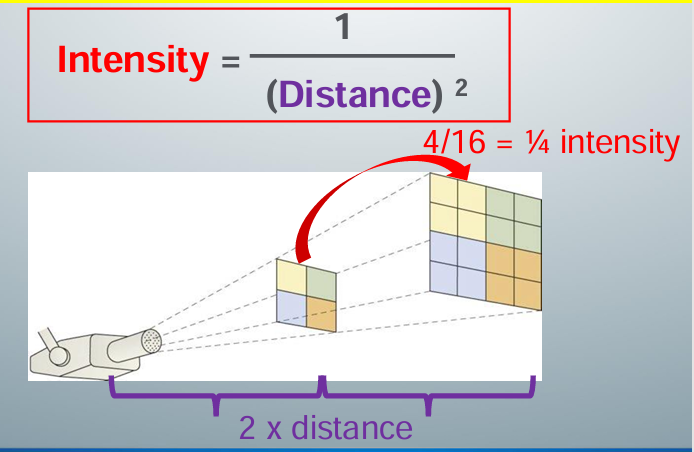
inverse square law
-intensity of an x-ray beam is inversely proportional to the square of the distance between the source and the point of measure
how to acquire a diagnostic image
-correct radiation technique using correct projection geometry
-correct exposure settings
-correct processing of the exposed radiographic film/sensors
-any error in any element of this chain (technique, exposure, processing) will give us an image of non-diagnostic quality (not adequate for diagnosis)
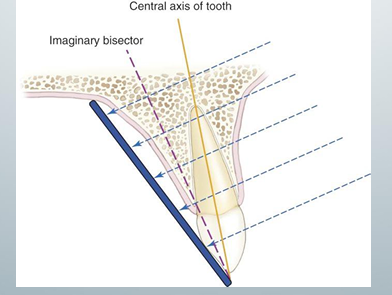
bisecting angle technique
-central ray is directed at a right angle to the imaginary plane that bisects the angle formed by the image receptor and the central axis of the object
-does not use principles of projection geometry, so there is a lot of image distortion
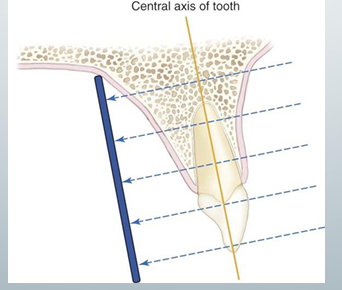
parallel technique
-ensures minimal image distortion
-used by most dentists
-central x-ray beam directed at a right angle to the central axes of the object and the image receptor: 1) put XCP so the image receptor is parallel to teh tooth, 2) align the aiming cylinder parallel to the metal bar of the XCP
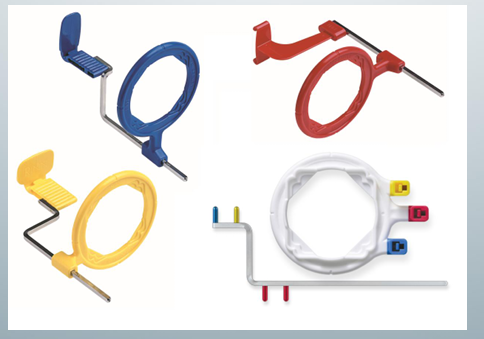
XCP
-extension cone paralleling
-blue for anterior
-yellow for posterior
-red for BW
projection geometry
-describe the effect of the x-ray source and the relative position of the object and image receptor on image clarity, magnification, and distortion
-used to maximize image clarity, minimize distortion, and localize objects in the image field
-involves the distance between 3 items: x-ray source, the object (teeth), and the image receptor
-key concept: x-rays travel in straight lines and have divergent paths
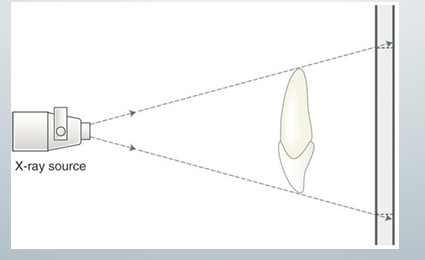
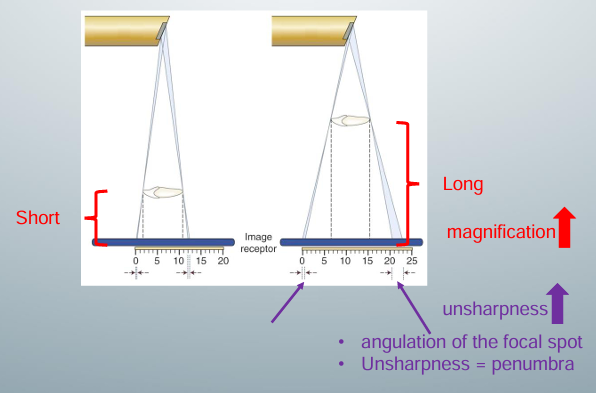
distance between the object and image receptor
-minimize
-long distance: the projected image on the receptor will be magnified because x-rays diverge
-short distance: projected image on receptor will not be as magnified
-width of blue x ray beam at end of object in long distance: width greater because more x-ray photons are hitting this end of the object due to the angulation of the focal spot (where x-rays are produced)’ gives us more projections at this end of the object on the receptor
-^sum of these projections captured on the receptor as an area of unsharpness (penumbra)
-by decreasing the distance between the object and the image receptor, we can decrease the magnification of the object and increase its sharpness
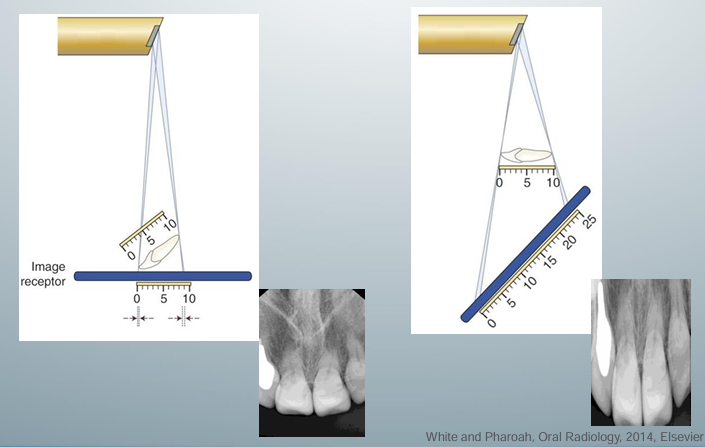
foreshortening and elongation
-occurs when the object and receptor are not parallel to each other
-foreshortening: happens when the central x-ray beam is perpendicular to the image receptor, but the object is not parallel with the image receptor
-elongation: happens when the central x-ray beam is perpendicular to the object but not to the image receptor
distance between the source and the object
-maximize
-short distance: projected image on the receptor will be magnified because x rays diverge
-long: x-rays diverge less, so projected image on receptor will not be as magnified
-due to angulation of focal spot, width of x ray beam is greater here because you have more x ray photons hitting this end of the object in the short distance set up- gives more projections on the receptor, which appear as penumbra (area of unsharpness)
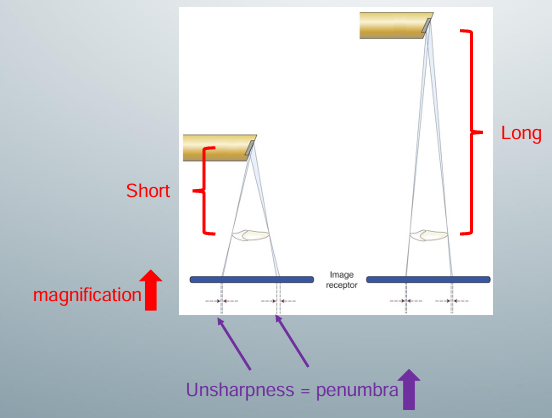
source-object distance clinically
-defined by the length of the aiming cylinder
-market has 8”, 12”, and 16” cones
-choose the one with the longer cone in order to maximize s-o distance to minimize image magnification and image penumbra
size and angulation of focal spot
-focal spot: target where a beam of fast-moving electrons hits to produce x rays from the x-ray unit, has a specific size and angulation in relation to the electron beam to ensure efficient x-ray production and correct projection geometry, sits in copper stem to help dissipate heat
-need a small focal spot at a specific angle
-small focal spot increases the sharpness of the image and decreases the penumbra
-if focal spot too small, though, the heat can destroy the focal spot and the life of the x-ray tube will be shortened
-actual focal spot is a bit bigger than the effective, projected focal spot that is used
-actual focal spot placed at an angle to project a smaller focal spot so actual will have a large enough area to dissipate the heat and produce sharp images
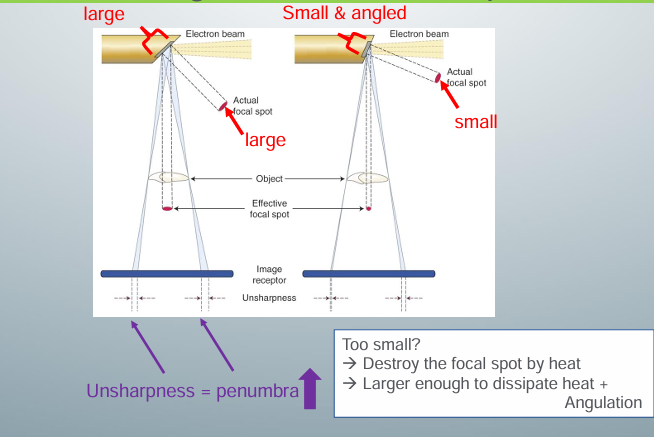
angulation and size of focal spot
-around 20 degrees to the x-ray beam
-most have 0.4mm size
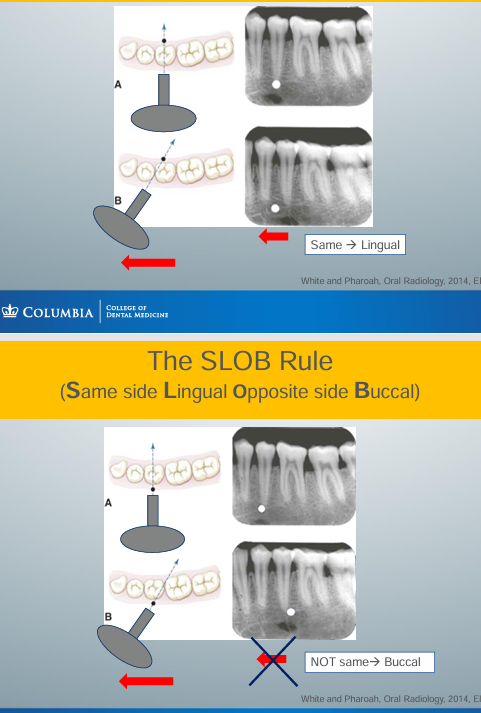
the SLOB rule
-SLOB: Same side Lingual Opposite side Buccal
-if the object shifts in the same position as how you have shifted the aiming cylinder, then the object is lingual to a reference point
-if the object shifts in the opposite position as you have shifted the aiming cylinder, then the object is buccal to a reference point
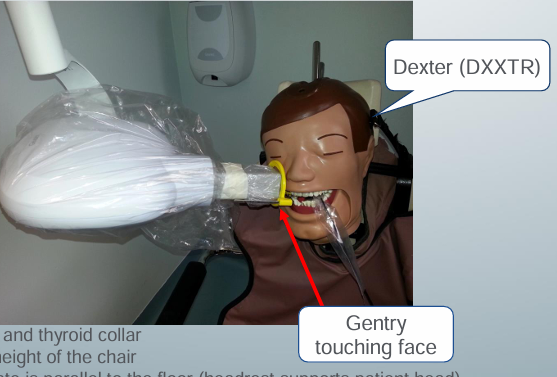
good radiographic technique
-lead apron and thyroid collar
-adjust the height of the chair- maxillary images position chair lower
-occlusal plate parallel to the floor (headrest supports patient head)
-swing x-ray unit closer
-put the image receptor in XCP
-align the aiming cylinder of the x-ray unit
diagnostic BW view

bad BW view
-wrong horizontal angulation → contacts overlap
-cannot evaluate the interproximal caries
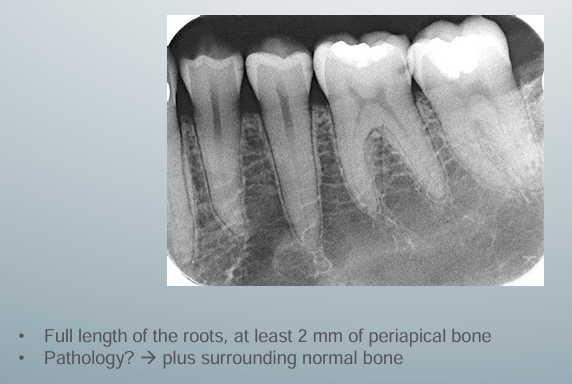
diagnostic PA view
-ensure nothing is distorted
patient should not be ______
-holding the image receptor (sensor, PSP plate) with his/her finger anytime during exposure!!
take home message