Body Composition
1/23
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
24 Terms
what is excess BF associated with?
-Excess body fat is associated with many chronic conditions.
*remember that BMI is an ACSM risk factor (high BMI=higer risk)
what % of Americans or OW or Obese? % of Children?
-Approximately 70.2% of American adults are classified as either overweight or obese, and more than a third (37.7%) are classified as obese.
-Nearly one-third (31.8%) of American children and adolescents are overweight or obese.
*carry into adulthood; genetic factors
Health-related changes in body composition that accompany aging:
-Increasing body fat
-Decreasing bone mineral density
-Sarcopenia (muscle wastes away)
*Heart Failure ex: normal BMI, but high BF and low LBM
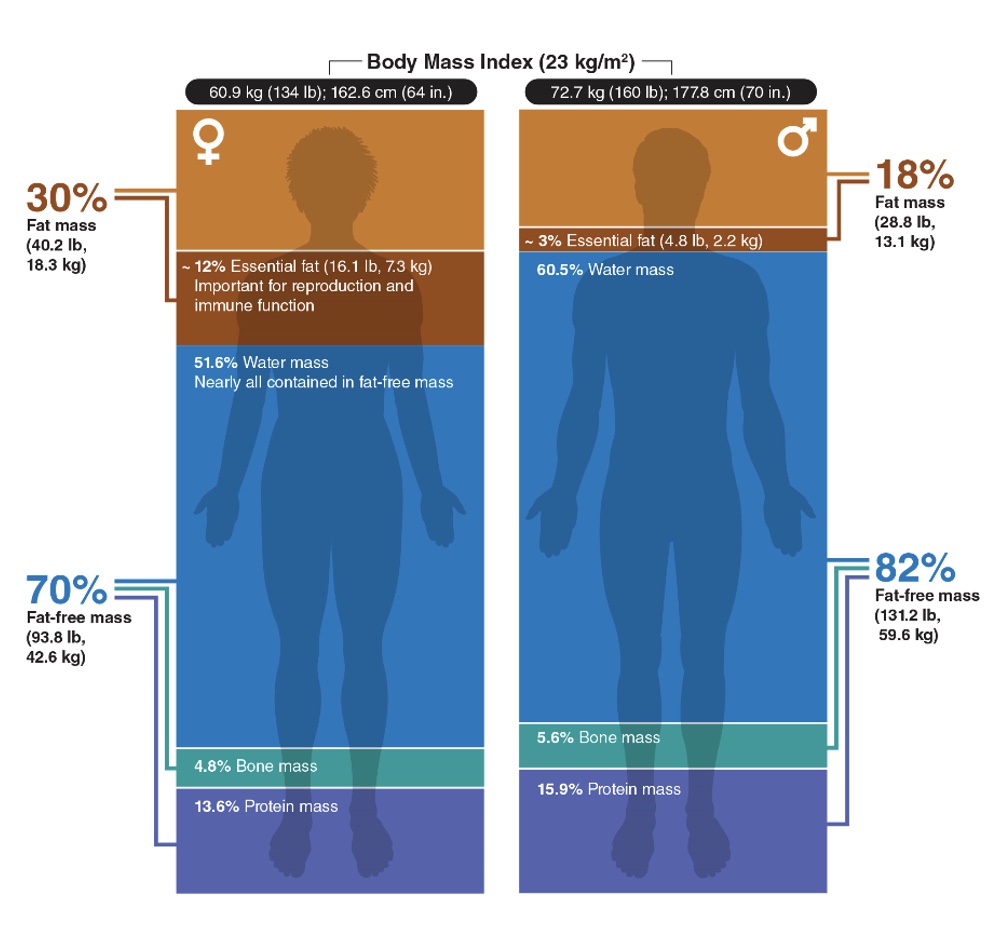
Two-component model
-Expressed as the relative percentage of mass that is fat (FM) and fat-free (FFM) using a two-component model
-Estimated with methods that vary in terms of complexity, cost, and accuracy
-general considerations when weighing someone
-units for BMI
-what does BMI fail to distinguish?
-Calibrated scale with individual wearing minimal clothing, empty pockets, and no shoes
-BMI (kg/m2): body weight (kilograms) / height (meters squared)
-Fails to distinguish between body fat, muscle mass, and bone
*just gives overall distribution
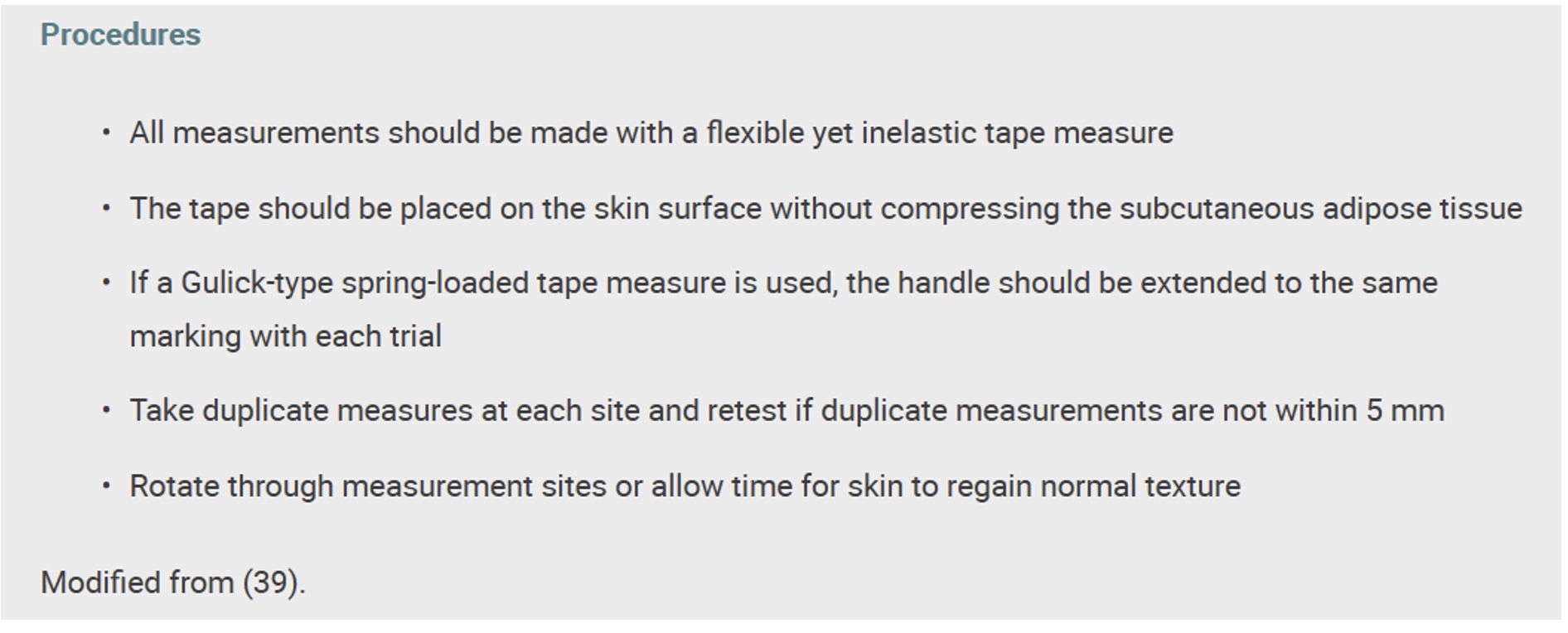
circumferences
-Quantify body fat distribution, especially of the waist and hip
-Equations to predict body fat percentage from circumference measures (standard error of estimate [SEE]=2.5%-4.0%)
*BMI + circumference: most of what need to know risk factor
android obesity vs gynoid obesity
-Android obesity (more abdominal fat) increases risk of chronic diseases compared to gynoid obesity (more fat in hip and thigh)
-Visceral vs. subcutaneous fat
waist to hip measurement procedure
Anatomic Origins and Methodology for Body Circumference Measures
*wasit to hip
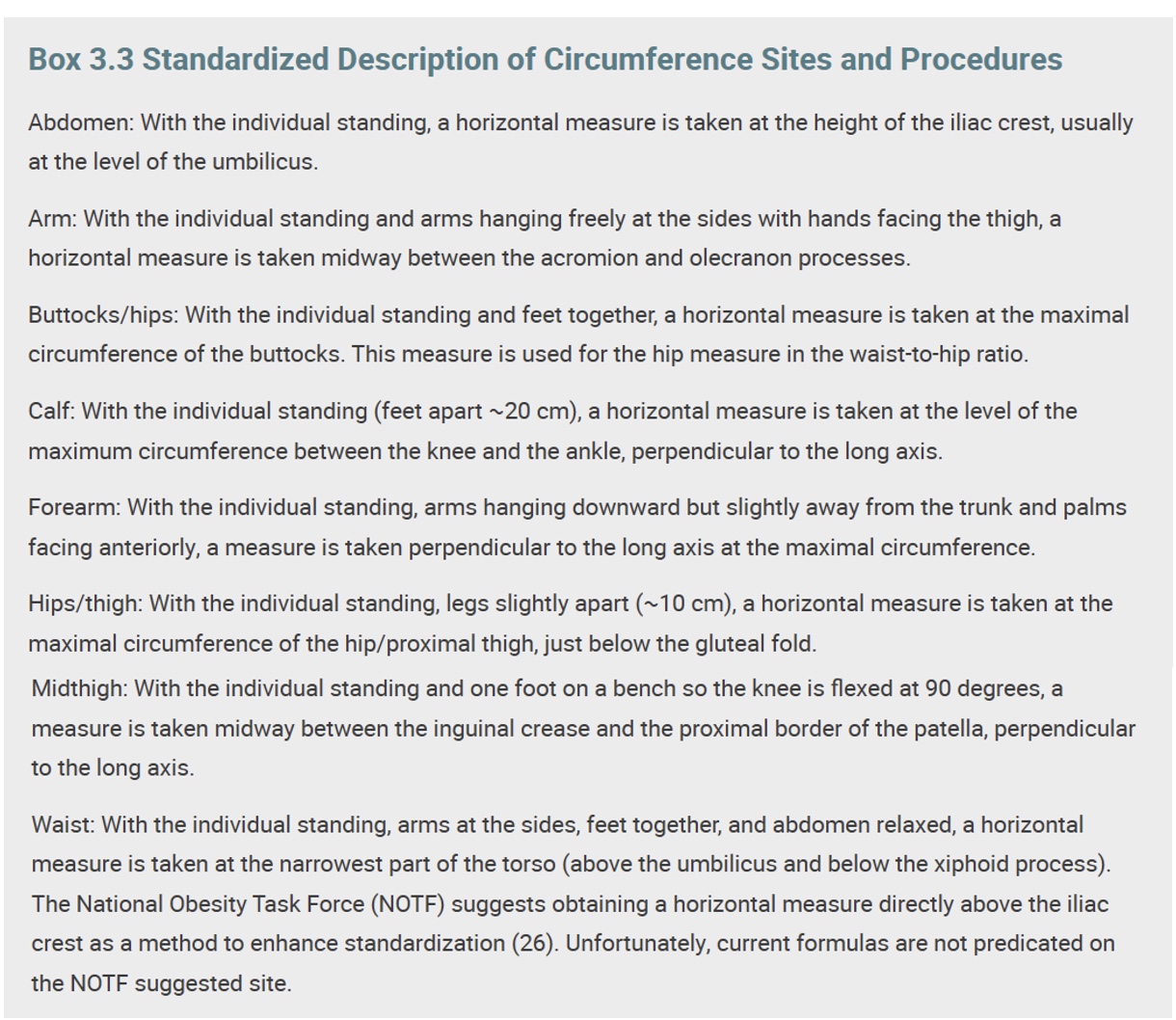
Waist-hip ratio: how measure + risk associated with certain #/s
-Waist-to-hip ratio (WHR): circumference of waist (above the iliac crest) divided by the circumference of the hips (buttocks/hips)
-Health risk increases as WHR increases, and the standards for risk vary with age and sex.
•Younger than 60 years: very high health risk for men with WHR >0.95 and women with WHR >0.86
•60-69 years: very high health risk for men with WHR >1.03 and women with WHR >0.90 (*slightly higher)
*generally, >1= lot of mass in abodmen
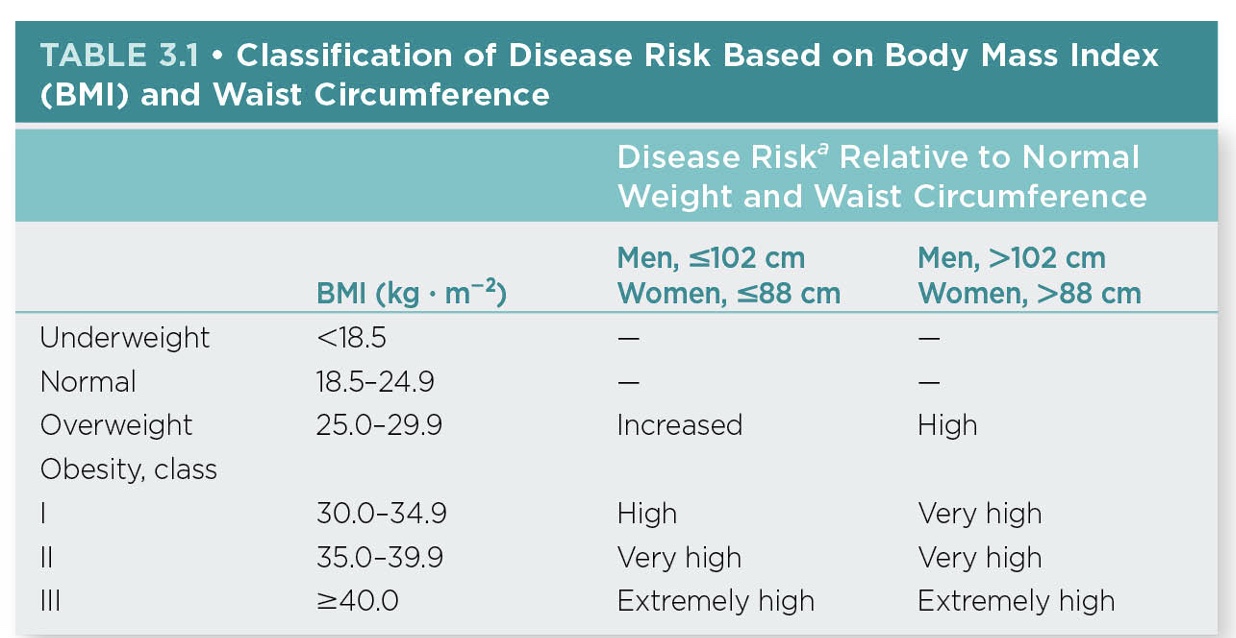
-Waist circumference: indicator of obesity-related health risk because of central obesity as the primary health issue (*central obesity= higher risk CAD)
-Similar limitations as BMI
BMI classifications
*>30=ACSM RF/obese
*>25= OW
*<18.5= higher risk as well (bc can’t fight disease as well; contraversal for people with cystic fibrosis, cancer, etc.)
true or false: BMI and waist circumference are simple antroprometric measures for body comp?
true! (height and weight → calc BMI)
*skin folds are NOT
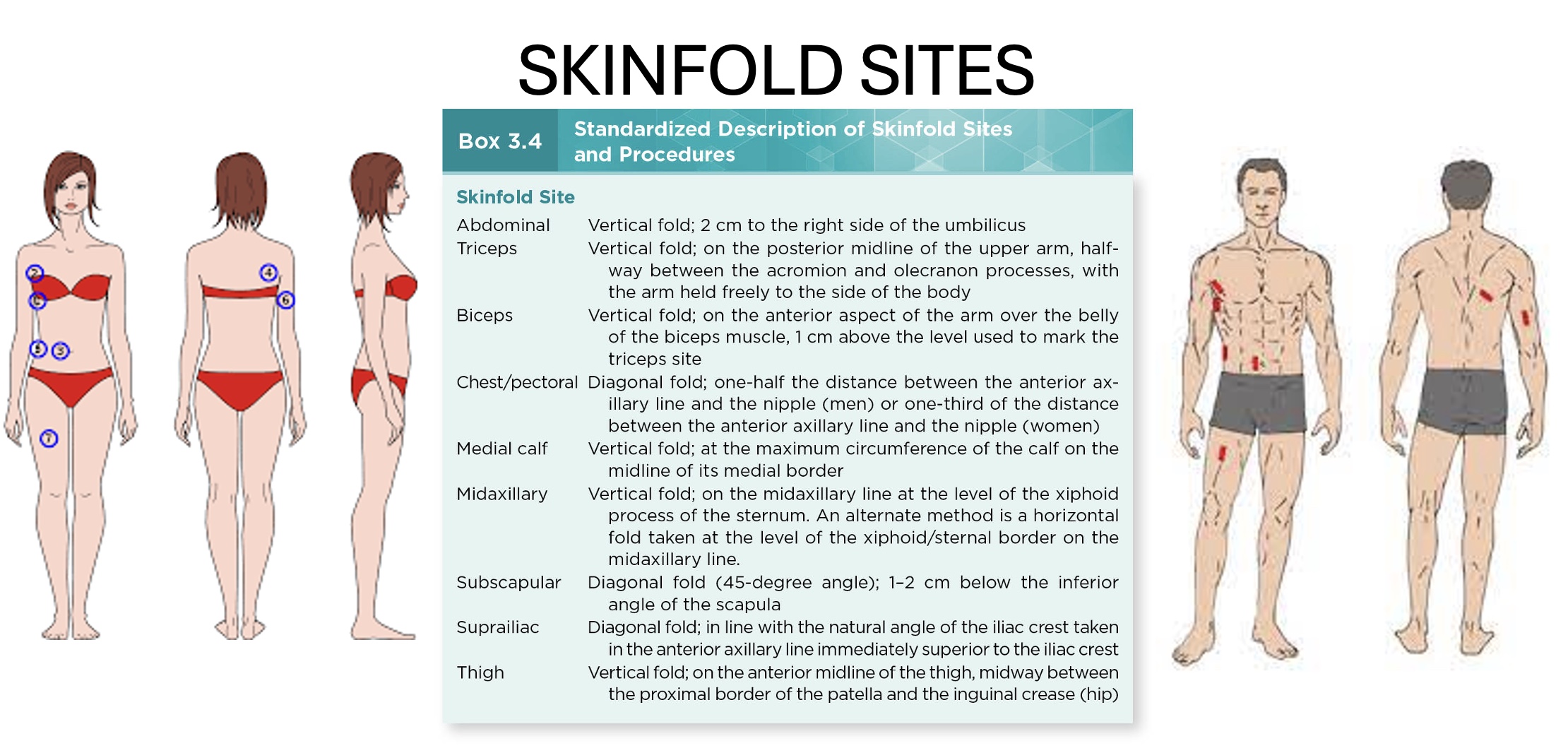
what are skin fold measurements used for? based on what prinicple? sites?
-Estimates body fat percentage by determining thickness of several folds of skin across body
*NOT a simpe antro measure!
-Principle: amount of subcutaneous fat is proportional to total amount of body fat
•~1/3 of total fat in body is located subcutaneously
•Exact proportion varies with sex, age, and race
what are the pros and cons of skin folds?
-Pro: Correlates well (r = 0.70–0.90) with hydrodensitometry, air displacement plethysmography, and dual-energy X-ray absorptiometry (DXA) values
-Con: ~±3.5% accuracy, but need skill to be accurate; generally has higher amount of body comp error
skinfold measurement procedures
-All measurements should be made on the right side of the body with the individual standing upright.
-Caliper should be placed directly on the skin surface, 1 cm away from the thumb and finger, perpendicular to the skinfold, and halfway between the crest and the base of the fold.
-Pinch should be maintained while reading the caliper.
-Wait 1–2 seconds before reading caliper.
-Take duplicate, but not consecutive, measures at each site, and retest if duplicate measurements are not within 1–2 mm.
Factors that may contribute to measurement error within skinfold assessment
-Poor anatomical landmark identification
-Poor measurement technique
-An inexperienced evaluator
-An extremely obese or extremely lean individual (doesn’t work for one extreme or the other; same for all body comp measures)
-An improperly calibrated caliper (so calibrate beforehand with known mm block)
Densitometry
-Estimate of total body fat percentage derived from a measurement of whole-body density using the ratio of body mass to body volume
-Used as a reference or criterion standard for assessing body composition for many years
-Limiting factor: accuracy of the body volume measurement because body mass is measured simply as body weight
Hydrodensitometry
-Hydrodensitometry (underwater) weighing is based on Archimedes principle: When a body is immersed in water, it is buoyed by a counterforce equal to the weight of the water displaced.
•Bone and muscle tissue are denser than water, whereas fat tissue is less dense (more non-fat=sink)
•Loss of weight in water allows for calculation of body volume
*scale in tub, blow out all air in lungs; not used much anymore
-When two individuals have the same total body mass, the individual with more fat-free mass (FFM) weighs more in water and has a higher body density and lower percentage of body fat compared to the individual with less FFM.
*labor intensive, but good if patient compliment; not good for people w/ lung disease, lean people
Plethysmography
-Air displacement in a closed chamber
-Uses a dual-chamber plethysmograph that measures body volume by changes in pressure in a closed chamber
*”Bod Pod”
Conversion of Body Density to Body Composition
*determine body density → plug into equation → get body comp
-Percent body fat can be estimated once body density has been determined.
-Prediction equation to estimate percent body fat from body density using the two-component model of body composition:
•ex: [(4.95 / Db) – 4.50] X 100
-Age, gender, race, training status, and certain disease states may affect the density of FFM (much of this variance related to the bone mineral density component)
DXA
-Dual-energy X-ray absorptiometry (DXA)
-gold standard
-measured bone mineral density and body comp; measures water content as well
BIA
-Bioelectrical impedance analysis (BIA)
•Similar accuracy as skinfolds
•Stringent protocol adherence
*current enters 1 electrode and exits other, faster if more muscle (slower if more fat)
*measures water content as well; readily available and less expensive than DXA
*2 site or full body/4 site
*don’t do if have pacemaker, should be okay if pregnant, messed up by menstral cycle?
ultrasound + smartphone applications
-ultrasound: superficial layer to get body comp
-phone prob not best
Body comp norms
-No universally accepted norms for body composition
-Satisfactory for health:
•12%–23% for men
•17%–26% for women
-Age and race also impact what may be construed as a healthy percent body fat.