Exam 2 PMI Review
1/56
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
57 Terms
Timetable for Speech & Resonance Assessment: Birth to 3
working on quantity (# of words, length of utterance) over quality
Timetable for Speech & Resonance Assessment: Ages 3-4
perform speech/resonance VP comprehensive assessment, stimulibility testing, instrumental evaluation if needed
should have longer sentences and better receptive language
Timetable for Speech and Resonance Assessment: Annually
looking at puberty and how it affects speech (e.g., adenoid shrinkage)
Timetable for Speech & Resonance Assessment: After puberty to 18
screening evaluation every 2 years to make sure treatment is working and they are on the right tract
Why shouldn’t we wait too long to evaluate and treat VPI?
longer someone lives with compensatory errors, it is harder to unlearn
social and emotional aspects of living with VPI
Three steps of the Speech & Resonance Assessment
diagnostic interview, perceptual assessment goals, instrumental assessment
What are the goals of a perceptual assessment?
to determine diagnosis and cause
obtain info to make reccommendation or develop a treatment plan
What information is obtained during the diagnostic interview?
parents’ concerns and observations
medical history, diagnoses, and previous surgeries
developmental history (speech, motor)
feeding and oral-motor skills
evidence of upper airway obstruction and obstructive sleep apnea
treatment history, including previous therapy
What are we looking for during the language screening?
risk of langauage delay
formal vs. informal screening
if a language disorder is identified → intervention ASAP
Why is a single word articulation test not advised?
we don’t talk in single words
limited demand on overall speech system
target phoneme may be affected through co-articulation
test is time consuming
What perceptual assessment is the most reliable start?
single sounds
How to test for hypernasality in single sounds
prolongation of a vowel (low v. high vowels)
How to test for nasal emission in single sounds
prolongation of /s/ for both audible and inaudible emission
How to test for hyponasality, cul-de-sac resonance, or airway obstruction in single sounds
prolongation of /m/, if structure is affected or narrowed
How to test for hypernasality in syllables
repeat syllables with low v. high vowels
How to test for nasal emission in syllables
syllables with voiceless sounds combined with low and high vowels
How to test for hyponasality, cul-de-sac resonance, or airway obstruction in syllables
produce /m/ combined with high and low vowels
How to test for hypernasality and nasal emission while counting
60-70 or 66
How to test for hyponasality while counting
90-99 or 99
How to test for speech sound production and resonance and to screen for language?
Load sentences with phonemes that are produced with the same placement
What is the most challenging method of perceptual assessment?
conversation speech, key is finding the client’s interests
What all is being evaluated?
speech sound production
nasal emission
resonance
phonation
Speech sound production: determine the presence of the following
placement errors - are they within norms?
phonological errors - developmental range errors?
developmental errors
Speech sound production with structural anomalies: determine the presence of the following
obligatory distortions - nasalization, nasal emission
compensatory errors - glottal stop, pharyngeal fricative, etc.
Inaudible nasal emission
VPI opening quite large
Audible nasal emission
small VPI opening, lots of friction
Characteristics of nasal emission
weak or omitted consonants
short utterance length: counting from 60 to 70 in one breath
nasal grimace
Nasal emission abnormal structure features (small VP gap)
occurs inconsistently on all pressure-senstive sounds
occurs on plosives
occurence increases in connected speech
treatment: surgery
Nasal emission abnormal function features (posterior nasal fricative)
occurs consistently on phonemes particularly /s/ and other sibilants
never occurs on plosives
occurs the same in single words and connected speech
treatment: speech therapy
What aspect is the most important to determine?
resonance
Common resonance rating scales
seven-point scale
six-point scale: normal, mild, mild-moderate, moderate, moderate-severe, severe
four-point scale: normal, mild, moderate, severe
two-point: normal, abnormal
Why are resonance rating scales unreliable?
subjective
inter-rater reliability is low
severity of resonance can be dependent on content of speech
Does rating resonance severity matter?
not really, treatment is the same
What is more important to determine in terms of resonance?
the type of resonance

What is this?
dental mirror
used for visual detection
not very reliable
can show false positive results
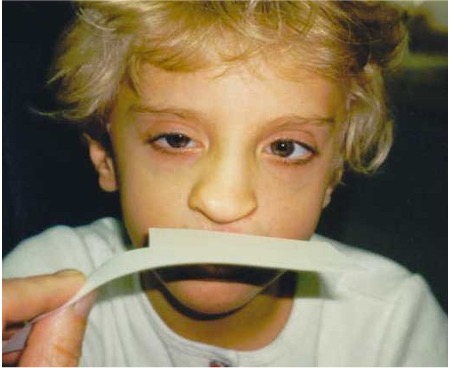
What is this?
air paddle
used for visual detection
can help with large openings and inaudible emissions
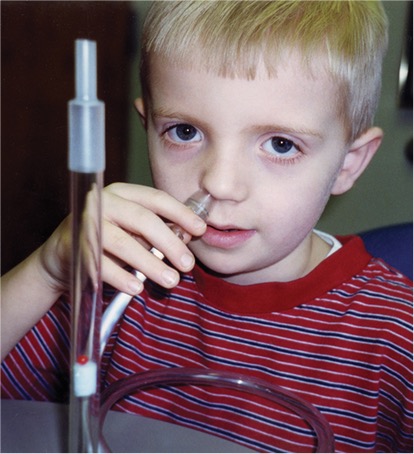
What is this?
see-scape
used for visual detection
very pricey
single client purpose only

What is this?
a form of tactile detection feeling the vibration of the nasal alae
What is the best form of detection?
auditory

What is this?
cul-de-sac test (nose pinch)
used for auditory detection
tests for hypernasality

What is this?
stethoscope
used for auditory detection
drum is removed and the tube in inserted into the nasal cavity

What is this?
a listening tube
used for auditory detection
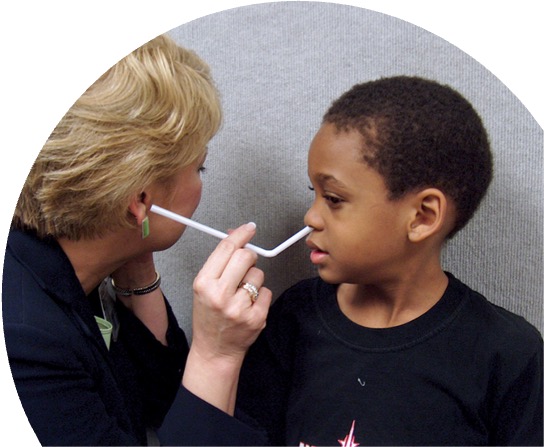
What is this?
straw
can function as a listening tube
used for auditory detection
Recommendations for VPI (insufficiency or incompentency)
surgery or prosthesis
speech therapy after correction of VPI for compensatory productions
Recommendations for VP mislearning
speech therapy only
What should always be done as a part of a speech or resonance evaluation?
an orofacial examination
Structural factors often contribute to…
the deviant speech or resonance characteristics
What can we evaluate during the orofacial exam?
oral structures and function, cannot evaluate velopharyngeal structure or function
tools for an intraoral exam
gloves
flashlight
dental mirror
tongue blades
sanitizing wipes
hand sanitizer

How to position a toddler or infant for an orofacial exam
place in parent’s lap facing the parent
have the child lay back so the head is over the parent’s or examiner’s knees
sit across from parent
close child’s nose if necessary (they will have to open their mouth)
crying helps (mouth is wide open)

Which structures should you see?
tonsils and palatal arch (vault)
What should we tell the patients to do and say?
have them say /æ/ (hat) instead of /ɑ/ (father)
tell them to stick their tongue out and try to touch their chin during phonation
What is palatal palpation used for?
to find the submucous cleft
When is a notch felt?
when the submucous cleft has extended all the way to the bone (overt cleft)
should feel the posterior border of the palate (palatal spine)
Examination of the oral cavity using a dental mirror
to examine the hard palate and see a fistula
tongue blade can be used to elevate the upper lip off the teeth or pull both lips back
provides a better view of the teeth and occlusion
Characteristics of oral-motor dysfunction
drooling
open-mouth posture and dropped jaw
anterior tongue position
history of feeding problems
difficulty executing oral-motor movements
Key factors of infection control
frequent handwashing
using antibacterial soap or antimicrobial gel
using gloves
disinfection of materials, equipment, and furniture