H/O Lecture 14: Bone Marrow Toxicity | Quizlet
1/57
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
58 Terms
Neutropenia
low WBCs
ANC <500
OR
<1000 w/ predicted decline to <500 in 48 hours
What are the s/sx of neutropenia?
Fever (may be the only sign)
Infection
Anemia
low RBCs (Hgb <10)
What are the s/sx of anemia?
Fatigue
Pallor
Dyspnea
Palpitations
Weakness
Dizziness
Thrombocytopenia
low platelets (plt <100)
Pancytopenia
decrease in ALL 3 cell lines
What are the s/sx of thrombocytopenia?
Petechiae
Nose bleeds
Gum bleeding
GI bleeds
Easy bruising
Hematuria
What ANC level is at highest risk for infection?
<500
Nadir
when ANC is at its lowest point after chemotherapy (~7-14 days)
What are the risk factors for neutropenia?
Type of chemo regimen
Previous treatments
>65 y/o
Poor performance status
Poor nutrition
Decreased immune function
Recent surgery
Prior chemo/radiation
COPD
CV disease
Liver or kidney disease
HIV
Heme malignancy
Bone marrow involvement
Which agents pose a HIGH risk of causing neutropenia?
Cyclophosphamide
Platinum agents
Anthracyclines
Taxanes
Cytarabine
Which agents pose a LOW risk of causing neutropenia?
Vincristine
Asparaginase
Bleomycin
Which agents pose a DELAYED risk of causing neutropenia?
Mitomycin
Busulfan
Melphalan
Thiotepa
Probarbazine
Carmustine
Which G-CSF agents are available for neutropenia?
Filgrastim
Pegfilgrastim
Which cells do G-CSFs affect?
Neutrophils only
Which G-CSF is dosed daily?
Filgrastim
What do G-CSFs NOT effect for patients with neutropenia?
Mortality
Tumor response rate
Overall survival
Reaching the nadir
What do G-CSFs effect for patients with neutropenia?
Decrease incidence of febrile neutropenia
Decrease duration of febrile neutropenia
Lessen nadir period
Fewer febrile days
Shorter duration of abx
Decreased number of infections
Fewer hospital days
When is primary G-CSF prophylaxis given?
for regimens with >20% incidence of febrile neutropenia
When is secondary G-CSF prophylaxis given?
after febrile neutropenia occurs
If a patient develops febrile neutropenia while using long-acting CSF primary prophylaxis with Pegfilgrastim, should they receive more G-CSF?
No
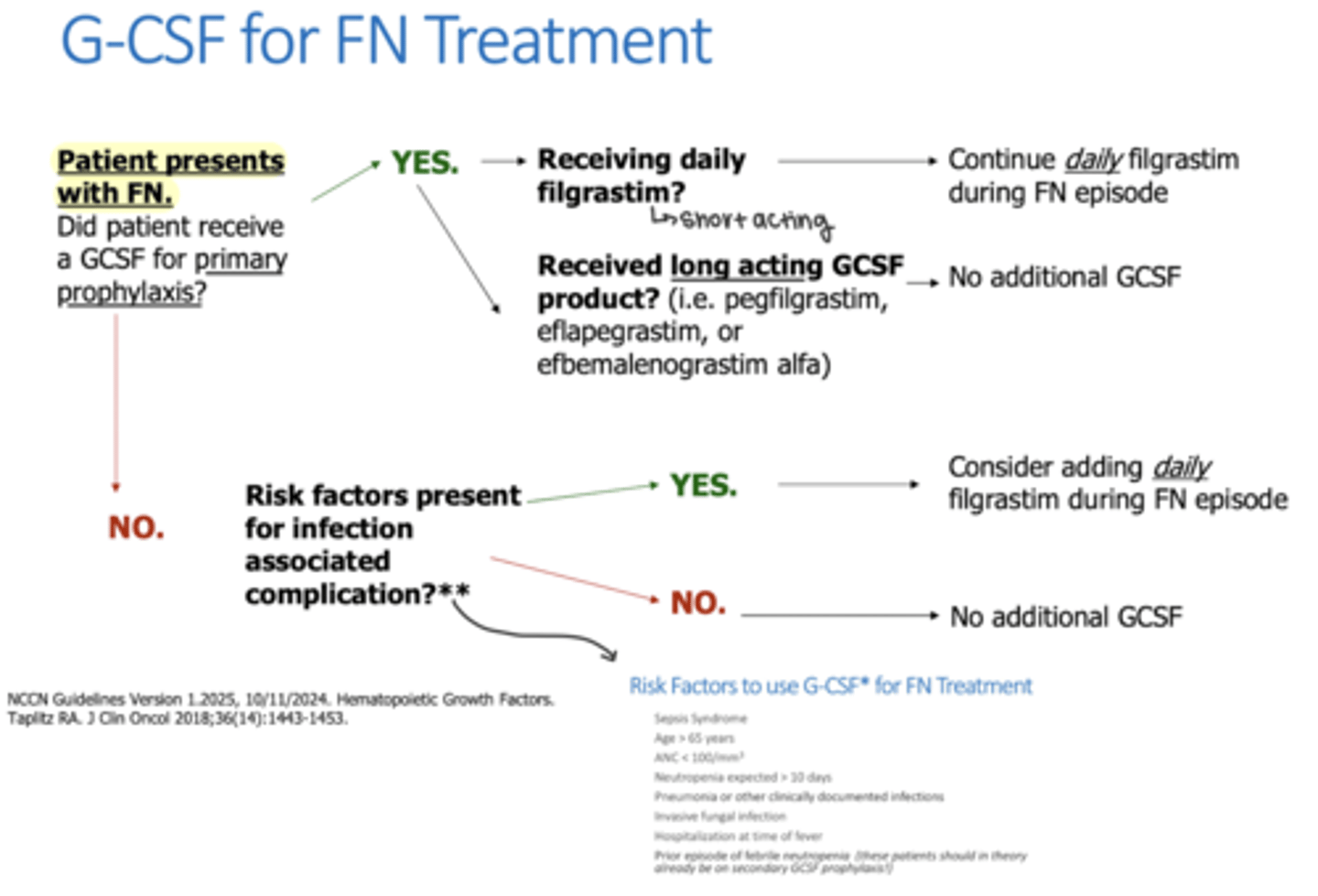
If a patient develops febrile neutropenia while using short-acting CSF primary prophylaxis with Filgrastim, should they receive more G-CSF?
Yes, Filgrastim is dosed daily during FN episodes
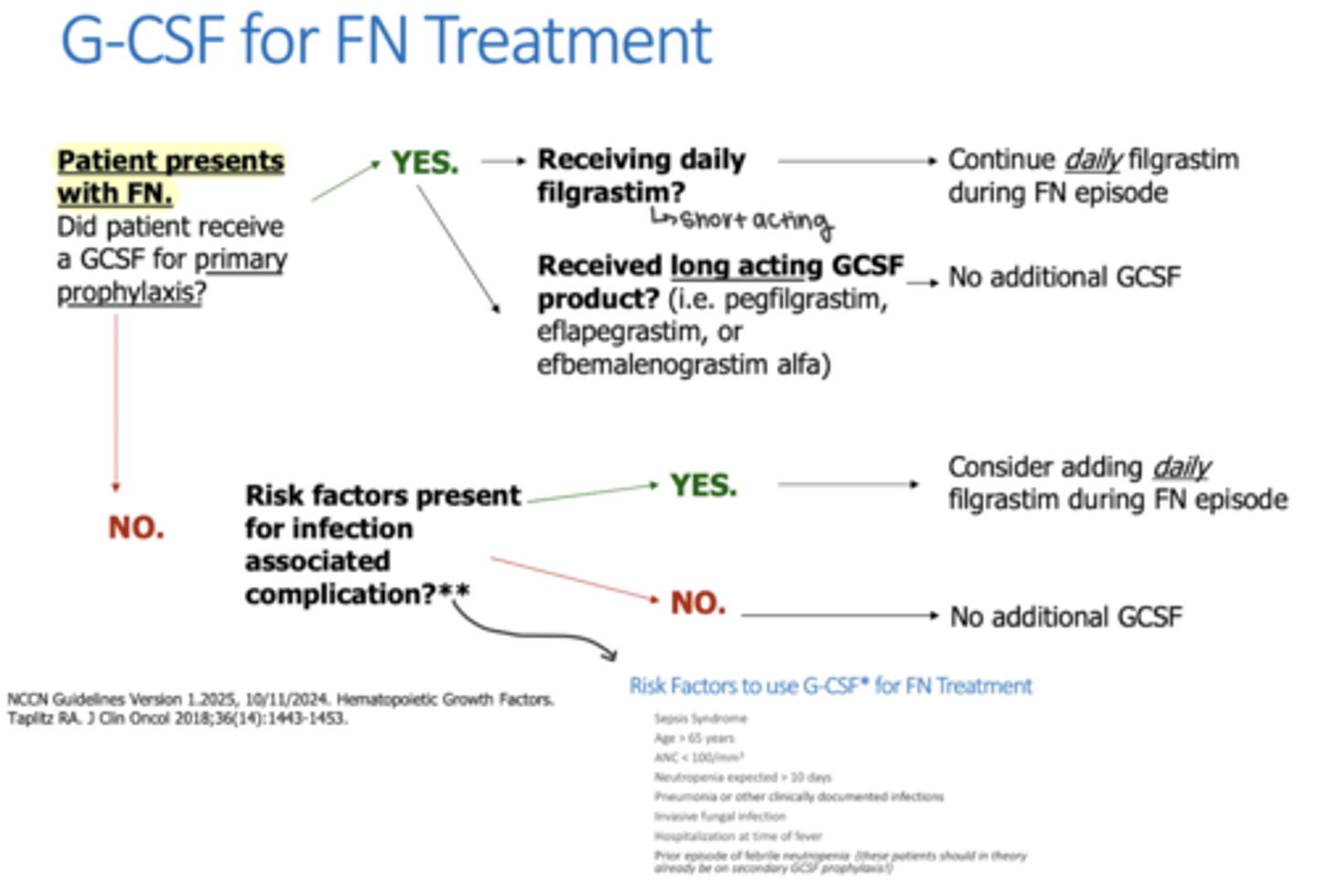
If a patient develops febrile neutropenia with no primary G-CSF prophylaxis, when would they recieve G-CSF treatment?
If they have risk factors present for infection associated complications
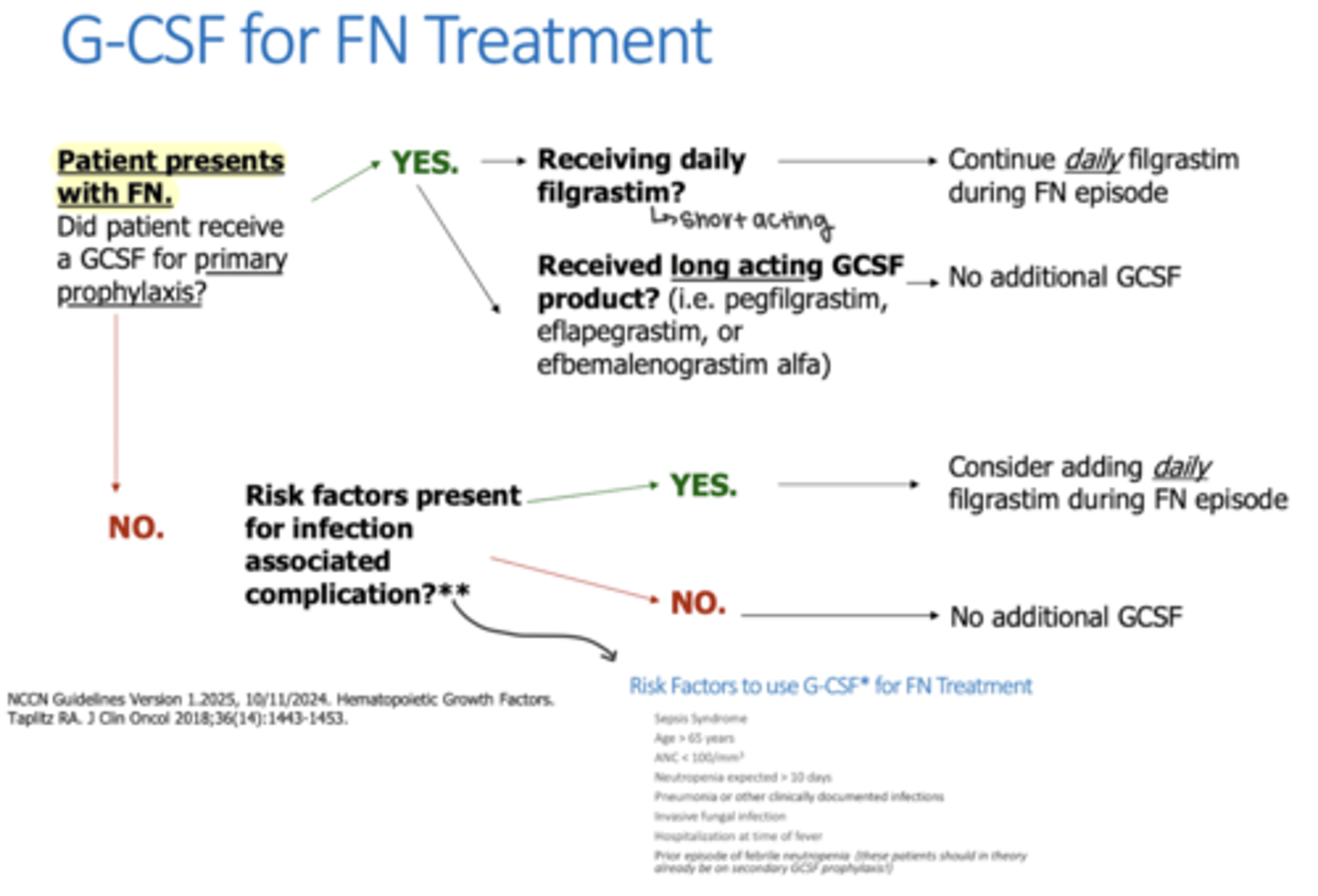
What factors put someone at risk for infection that warrant G-CSF treatment for febrile neutropenia?
Sepsis
>65 y/o
ANC <100
Neutropenia expected >10 days
Pneumonia for other documented infections
Invasive fungal infection
Hospitalization at time of fever
Prior episode of FN
Which G-CSF agent is indicated for the treatment of febrile neutropenia?
Filgrastim
Which G-CSF agent is only for prophylaxis of febrile neutropenia?
Pegfilgrastim
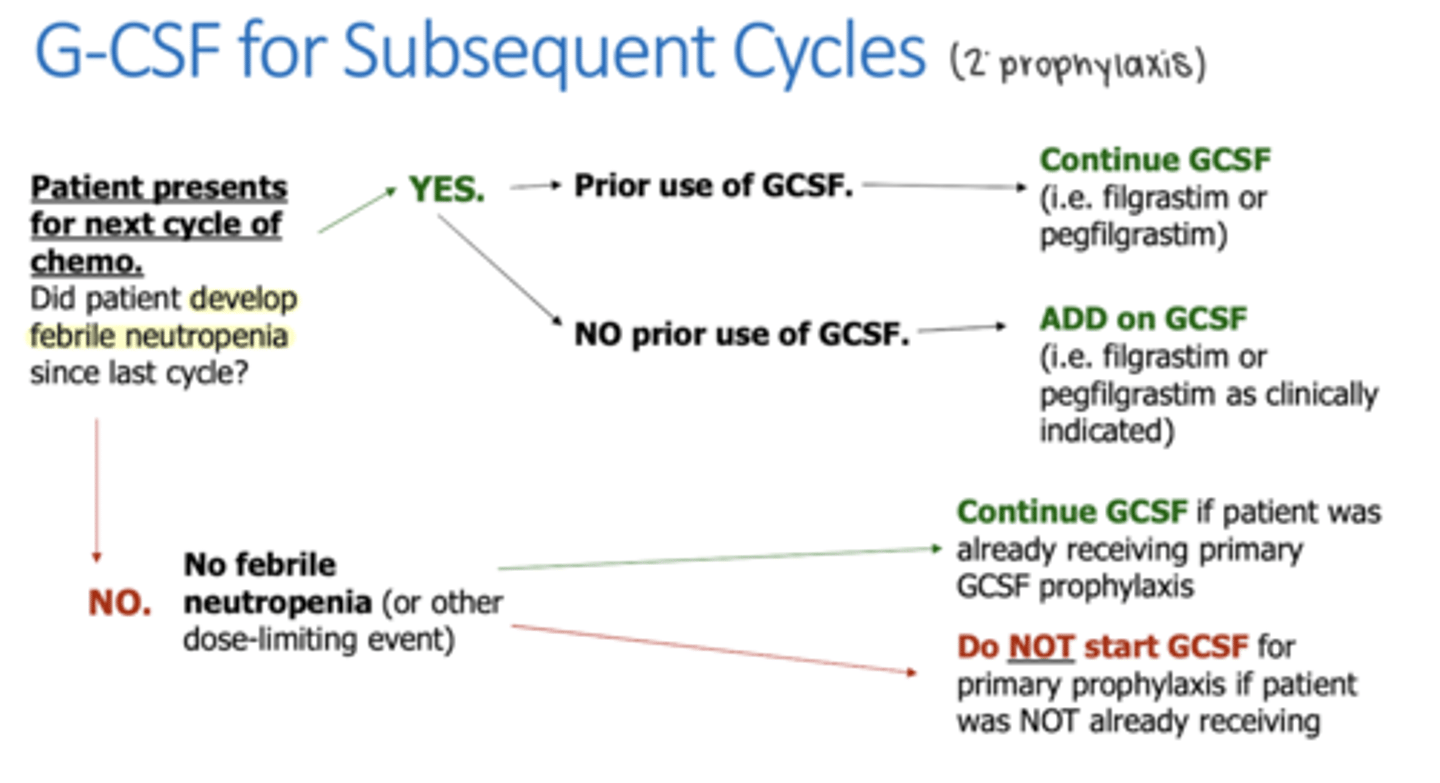
If a patient did NOT develop febrile neutropenia with their previous treatment cycle, should they receive G-CSF for their subsequent cycles?
Yes if they have been recieving primary prophylaxis
No if they have not been using primary prophylaxis
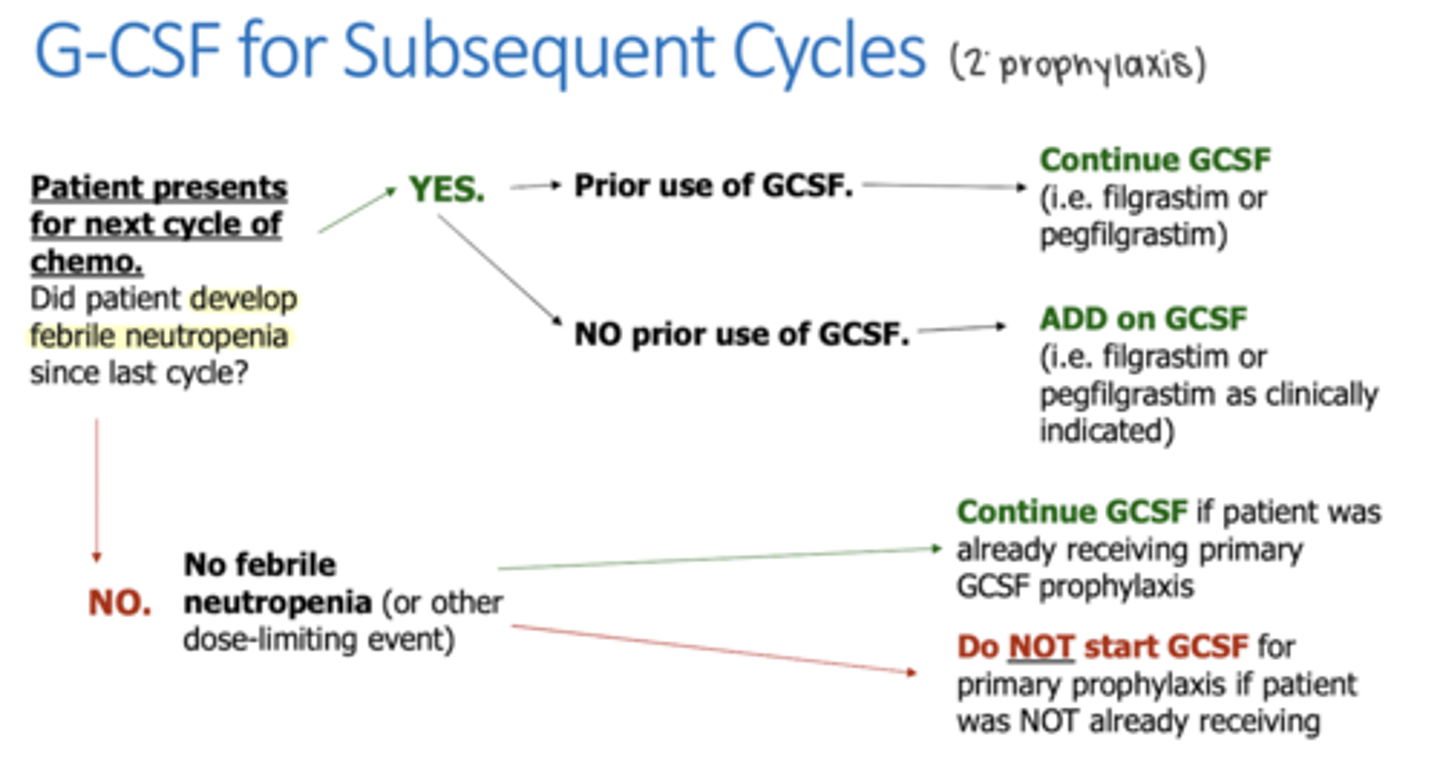
If a patient developed febrile neutropenia with their previous treatment cycle, should they receive G-CSF for their subsequent cycles?
Yes - doesn't matter if they have recieved primary G-CSF prophylaxis for not
How is Pegfilgrastim dosed?
once each cycle 24-72 hours after chemo
How is Filgrastim dosed?
Daily 24-72 hours after chemo
How long must patients wait between doses of Pegfilgrastim?
at least 12 days
Can patients get doses of Filgrastim if they have gotten Pegfilgrastim within the last 2 weeks?
No - need to be >12 days since Pegfilgrastim
What are the class effects of CSF?
Bone pain
Splenic rupture
Bruising
Inj site reactions
Generalized rash
Sickle cell crisis
What can be done for patients who experience bone pain with CSF?
Antihistamines (Loratadine)
NSAIDs if PLTs are okay
APAP
When are blood transfusions given to anemic cancer patients?
if Hgb <7-8 and symptomatic for rapid correction
What is considered moderate (grade 2) anemia in cancer patients?
Hgb 8-<10
What is considered severe (grade 3) anemia in cancer patients?
Hgb 6.5-<8
Why are ESAs controversial in cancer patients?
concern for progression of cancer
What are the risks of blood transfusions?
Iron overload w/ frequent infusions
Infusion reactions
What is used to treat iron overload?
Iron chelation agents
When should supplemental iron be given with ESAs?
Serum ferritin <500
AND
TSAT <50%
What are the ADRs of ESAs?
HTN
Pure red cell aplasia
Thrombosis
BBWs of ESAs
Risk of tumor progression
Increase risk of death from MI, stroke, VTE
Increase risk of CV associated death if given to CKD patients with a Hgb <11
What is the recommendation for ESA use in cancer patients
Must be on palliative chemotherapy
Use lowest dose needed
Hgb <10
Who is an ideal oncology candidate for an ESA?
Co-morbid CKD
Palliative chemo with frequent transfusions
Refuses blood products
Which formulation of iron is superior in cancer patients?
IV iron
What is the recommended dose of iron for cancer patients?
~1000mg IV iron
At what level of platelets are patients at high risk of bleeding?
Plt <20,000
When should patients recieve a platelet transfusion for thrombocytopenia?
Plts <10k
OR
Plts <20k AND symptomatic
1 unit of platelets would increase platelet levels by approximately how much?
~30K
What level of platelets is required for surgery?
>20-50k
TPO Receptor Agonists
Eltrombopag
Romiplostim (Nplate)
Are the TPO receptor agonists approved for use in cancer patients?
No - currently used off-label
ADRs of Eltrombopag
Hepatotoxicity
Thrombosis
ADRs of Romiplostim
HA
Arthralgia/myalgia
Thrombosis
Myelofibrosis
Should surgeries be delayed if a patient's platelet levels are below 20-50k?
No
What is the mainstay treatment of thrombocytopenia in cancer patients?
Platelet transfusions
When are TPO receptor agonists used in thrombocytopenic cancer patients?
If patients are refractory to platelet transfusions