PIE- Cytology
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
What is cytology?
-Cytology is the study of cells under a microscope to evaluate disease.
-It helps in diagnosing inflammatory, infectious, and neoplastic (tumour-related) conditions.
What are the key steps in cytological evaluation?
>Determine if the sample is adequate – Are there enough cells? Are they well-preserved? Has the stain been able to penetrate?
>Classify the sample – Is it inflammatory, neoplastic, or cystic?
>Determine inflammation type – Suppurative, granulomatous, eosinophilic, etc.
>Assess for sepsis – Look for bacteria and degenerate neutrophils.
>Classify neoplasia – Epithelial, mesenchymal, or round cell type.
>Determine malignancy – Benign vs malignant features.
under the microscope what do you consider on cytological examination
Low power review (x10 obj)
Good places to look at
Quality
Any/many cells?
Well/poorly preserved?
Background
Haemorrhage, granules, protein, matrix, debris, disrupted cells
Predominant cells
Neutrophils?/Other cells
Cells (x 40 or oil)
Individual or organised
Single or mixed population?
Cell size, shape, variation?
Nuclear size, shape, variation, abnormal mitoses?
What is our approach to unknown masses?
1.Is the sample sufficient for diagnosis
2.Inflammatory?
2.Septic?
3.Is there cystic content?
4.Mainly tissue cells - neoplasia (epithelial, round, mesenchymal)
5.Benign or malignant
What is our approach to known tissue?
>Known tissues may include- lymphnode, prostate, spleen, liver
>Think about the normal cell population in that tissue; does what you have on the slide match that. E.g., should it be epithelial, round or mesenchymal or a mixture, what functional cells should be present
>Think about possible pathologies (e.g., what 4 things cause lymph nodes to enlarge, what 4 things cause prostatic enlargement); which does the cytology best fit with?
>Is there evidence of inflammation
>Which of my narrowed list of possibilities fits best?
Guidance for unknown masses

How do you differentiate between inflammation, neoplasia, and cystic lesions?
Inflammation – Predominance of neutrophils, macrophages, eosinophils, or lymphocytes.
Neoplasia – Presence of abnormal tissue cells with nuclear atypia.
Cystic lesion – Presence of acellular debris, cholesterol crystals, or proteinaceous material.
What does sepsis look like in cytology?
Presence of bacteria within neutrophils.
Degenerate neutrophils (swollen, pale-staining nuclei).
Possible presence of fungal, protozoal, or yeast elements.
How do you classify neoplasia based on cytology?
Epithelial tumours – Cells arranged in clusters.
Mesenchymal tumours – Cells arranged individually or in loose aggregates.
Round cell tumours – Discrete, individual round cells.
What are cavity effusions?
Fluid in chest or abdomen or pericardial space
What are cavity effusions classified into?
-Protein poor transudate
-Protein rich transudate
-Exudate (inflammatory usually)
What cell types are significant in effusions?
Neutrophils – Indicate inflammation (degenerate vs non-degenerate, is bacteria present?).
Lining cells (mesothelial cells) – Can be reactive but not necessarily neoplastic.
Lymphocytes – May suggest chylous effusion.
Lots of epithelial cells- suggests epithelial tumour
Neoplastic cells – May suggest carcinomatosis.
why do we want to identify lining cells
The reason we want to just spot those is because they're often very reactive.
They're not happy about lining the cavity when there's fluid in it,
but the way they demonstrate their reactivity looks very like a neoplastic cell.
So we just need to be able to identify them and be comfortable that those are just reactive mesothelial cells.
What are the cellular criteria of malignancy divided into?
§Cellular
§Nuclear
§Cytoplasmic
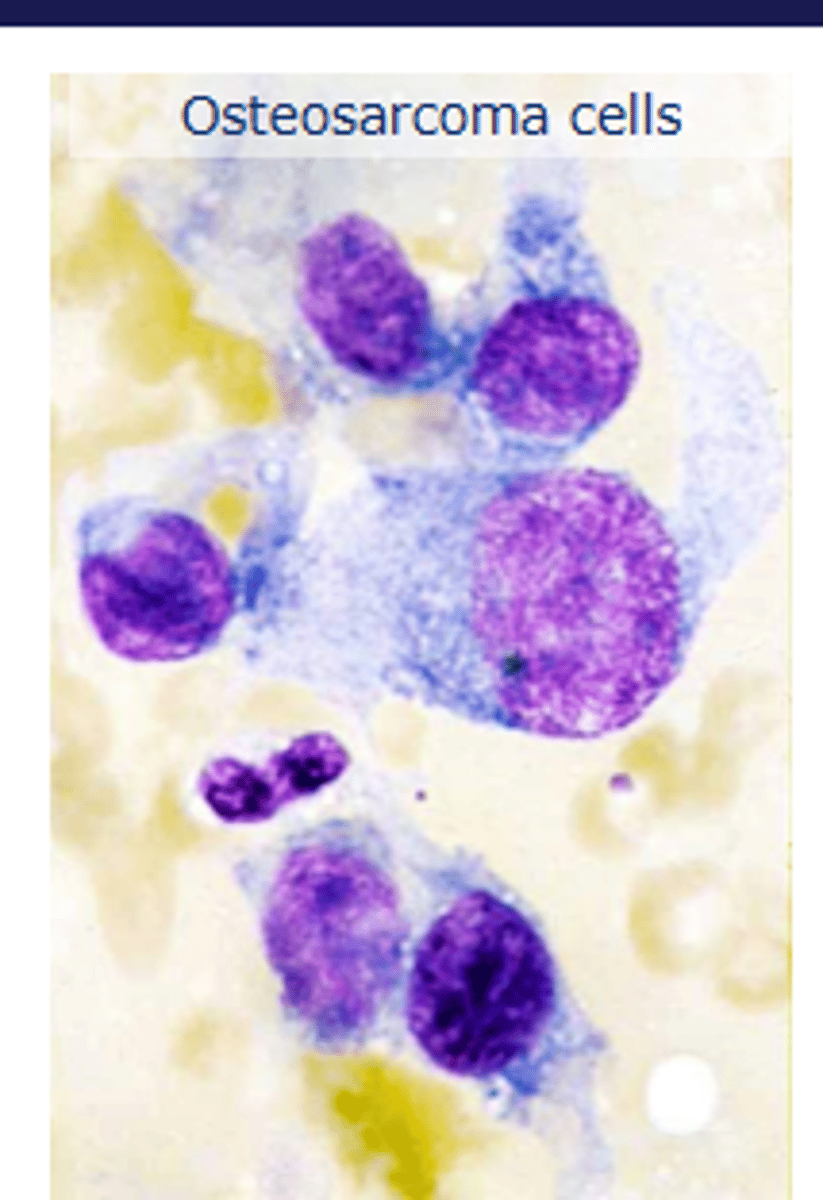
what is this
cellular malignancy
osteosarcoma
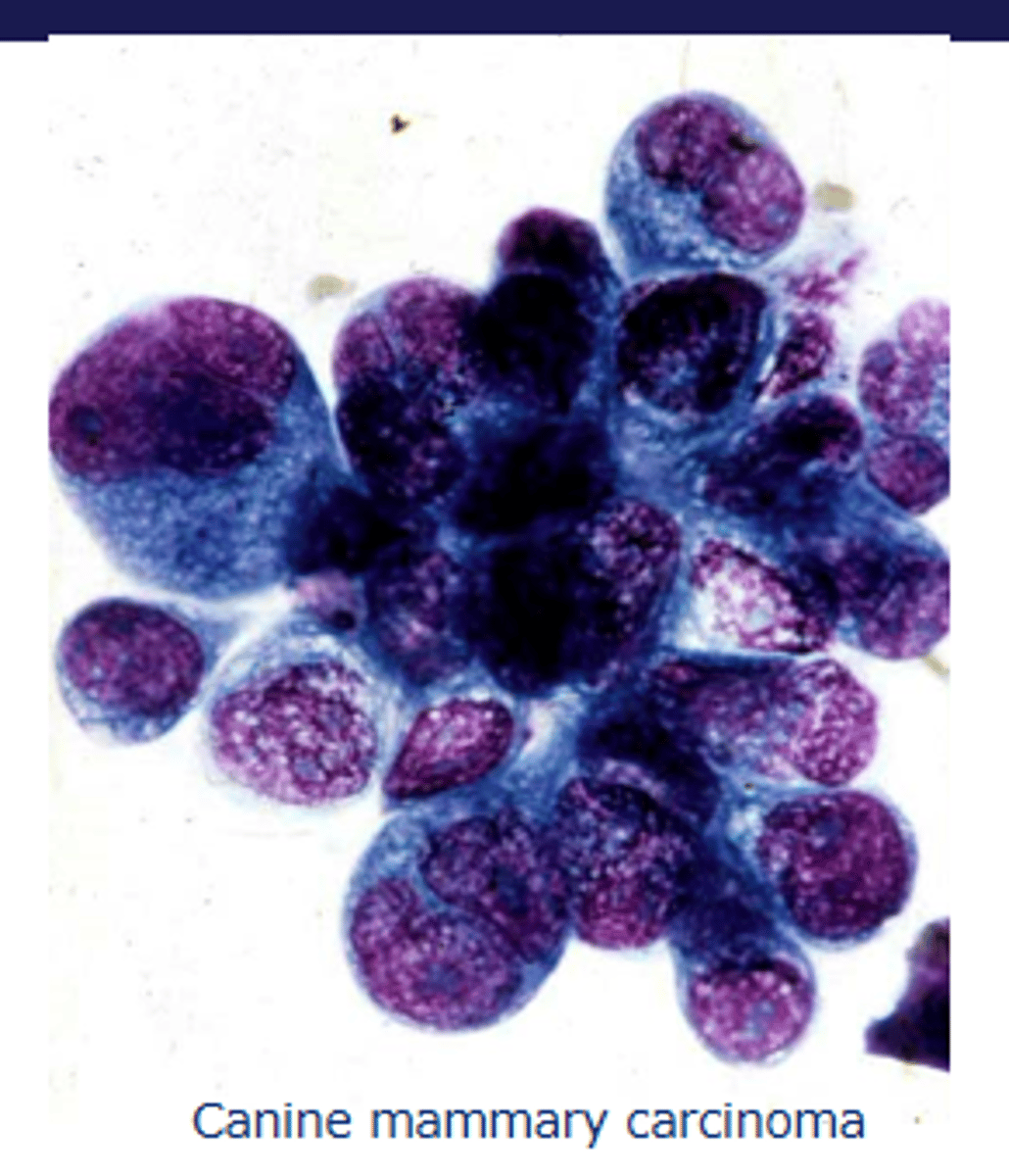
what is this
nuclear maliganancy
mammary carcinoma
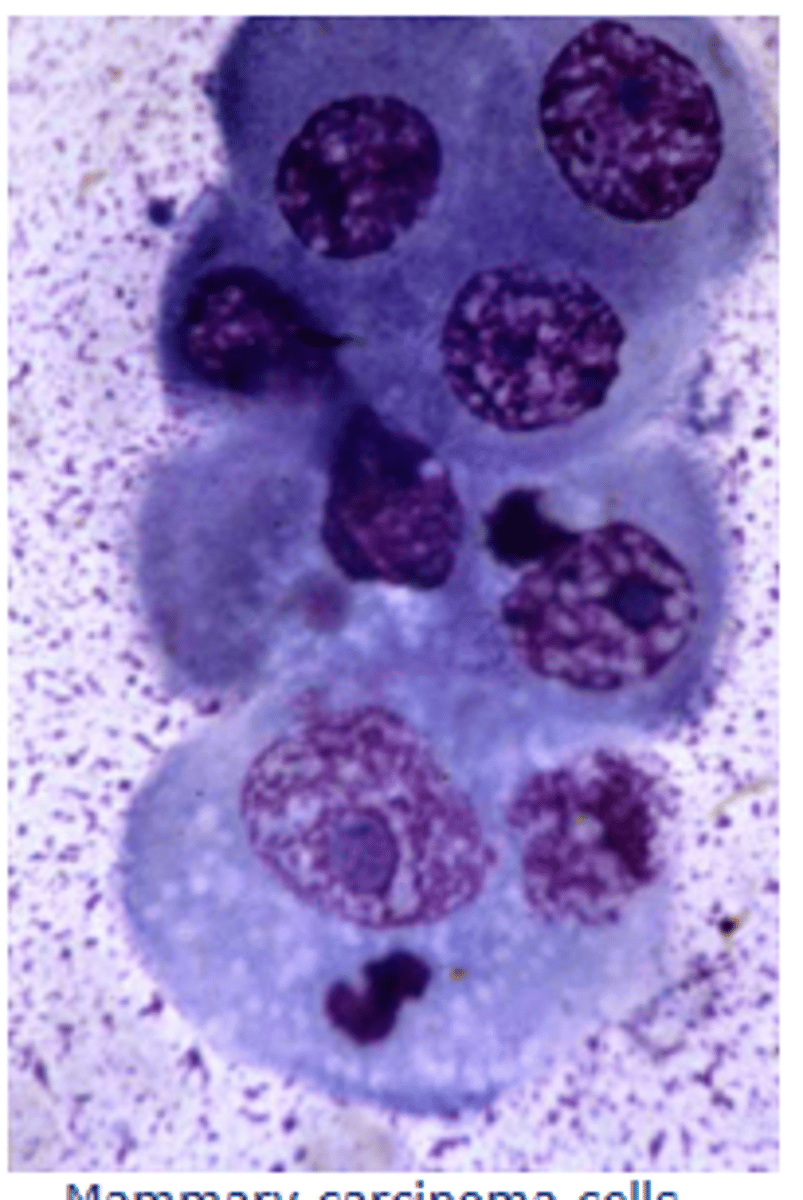
what is this
cytoplamic malignancy
mammary carcinoma
What are key features of cellular malignancy?
Cells present in a location where they shouldnt be
pleomorphism within a cell type
Variation in cell size (anisocytosis).
EXCEPT lymphoid
Monomorphic population in tissues expected to be diverse.
High nuclear-to-cytoplasmic ratio.
What are key features of nuclear malignancy?
Variation in nuclear size (anisokaryosis, >1.5x difference).
Multiple, fragmented, or moulded nuclei.
Clumped chromatin
irregular nucleoli.
Abnormal mitotic figures.
how can you asses nuclei size
find one of the smallest nuclei in a cluster,
then we try to decide how many of those fit into the largest nucleus.
Something less than 1.25. To 1.5. would be kind of hyperplastic and not particularly concerning,
but if we fit more than 1.5 times the small nucleus into the large nucleus, then that is a criteria of malignancy.
What are key features of cytoplasmic malignancy?
Increased basophilia or hyperchromasia (becomes darker blue)
Cytoplasm becomes a darker blue
Presence of vacuoles, granules, or phagocytosed material.
High cytoplasmic-to-nuclear variation within the sample.
Lymph Node Cytology
What are the main causes of lymphadenopathy (enlarged LN)?
Reactive hyperplasia – Increase in small lymphocytes with occasional large lymphocytes and plasma cells.
Lymphadenitis – Presence of inflammatory cells (neutrophils, eosinophils, macrophages).
Metastatic neoplasia – Presence of tumour cells from another location.
Lymphoma – Increased numbers of immature lymphoid cells (>50%).
what is Lymphadenitis
(Inflammation of gland itself)
What would Lymphadenitis look like
Increased neutrophils (>5%) or eosinophils (>3%)
Macrophages (>3%)
Incl epithelioid and multinucleate giant cells in granulomatous inflammation
Inflammatory cells may be mildly increased or completely replace normal structure
Lymph node pathology:
Eosinophilic - allergic (e.g., insect bites, FAD)
Granulomatous or pyogranulomatous - fungal and protozoal
whats this
Lymphadenitis
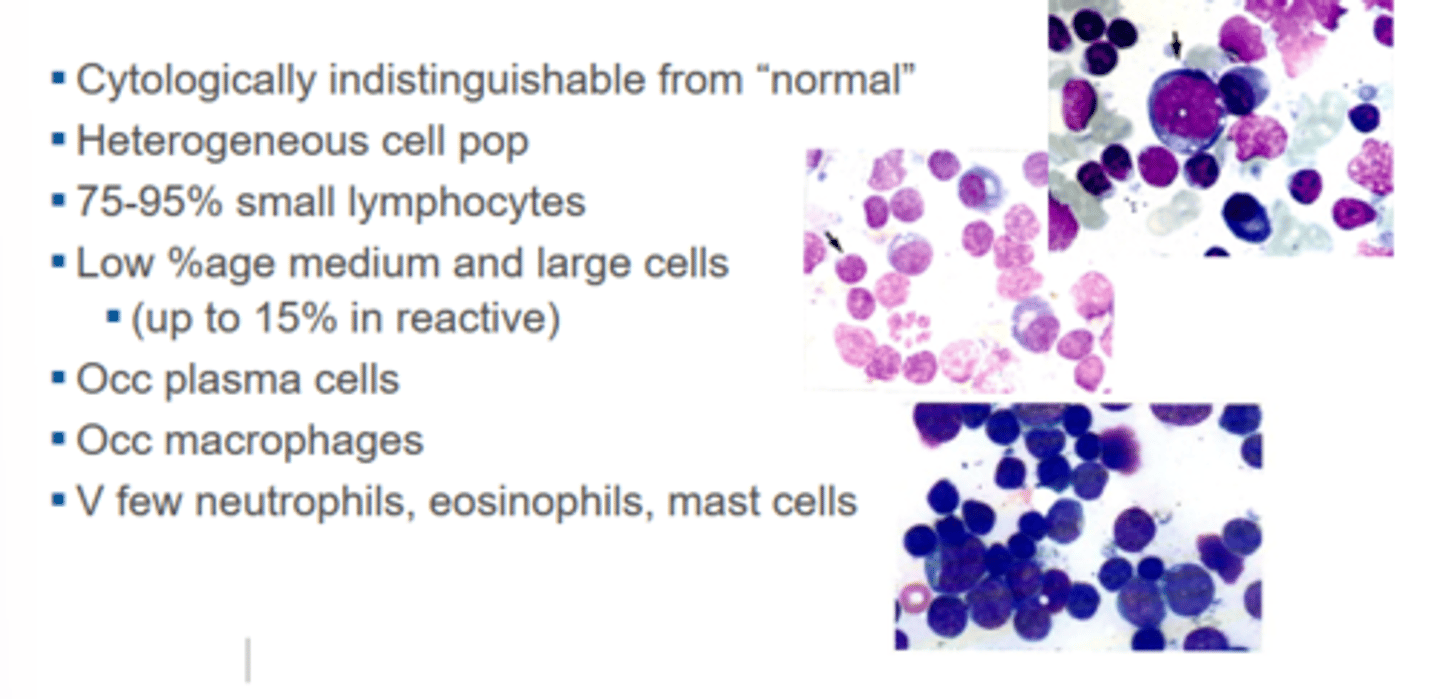
What would hyperplasia look like?
(Mostly young, large lymphocytes but some mature cells)
Cytologically indistinguishable from "normal"
Heterogeneous cell pop
75-95% small lymphocytes (so mature)
Low %age medium and large cells
Occasional plasma cells
Occasional macrophages
V few neutrophils, eosinophils, mast cells
whats this
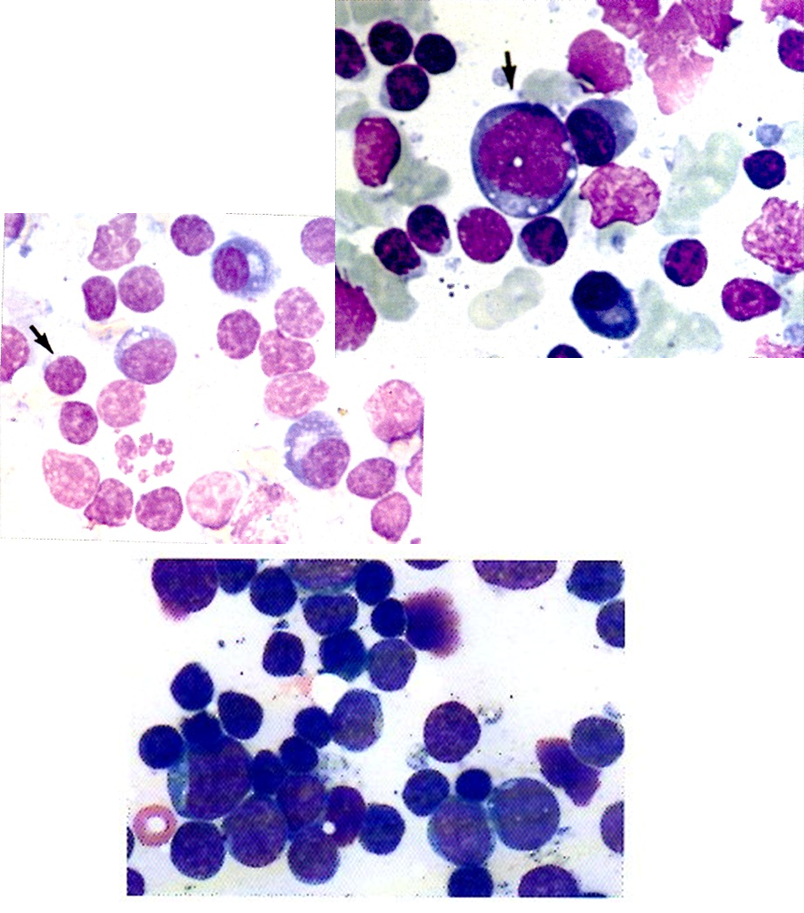
Reactive hyperplasia of ln
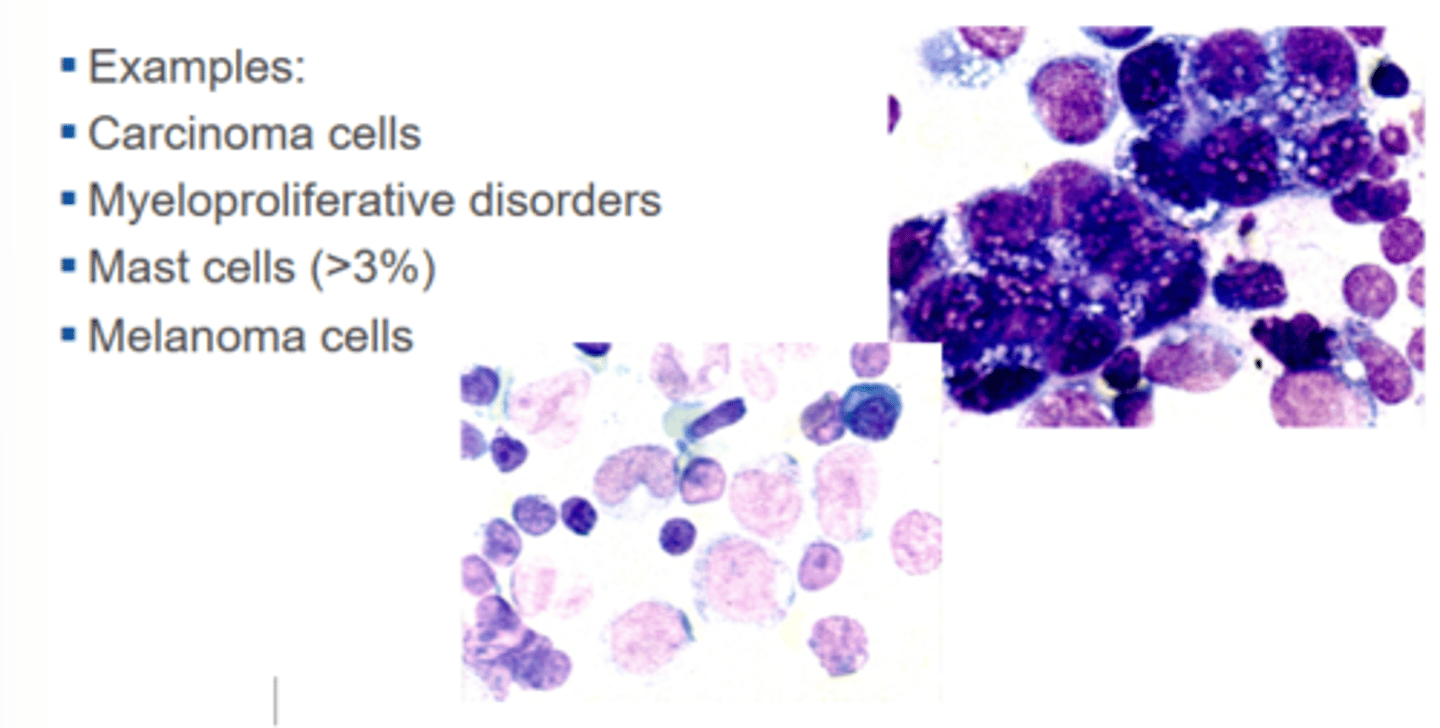
Examples of metastatic neoplasia
Carcinoma cells
Myeloproliferative disorders
Mast cells (>3%)
Melanoma cells
how does metastatic neoplasia affect the ln
it metastasises to the LN
whats this
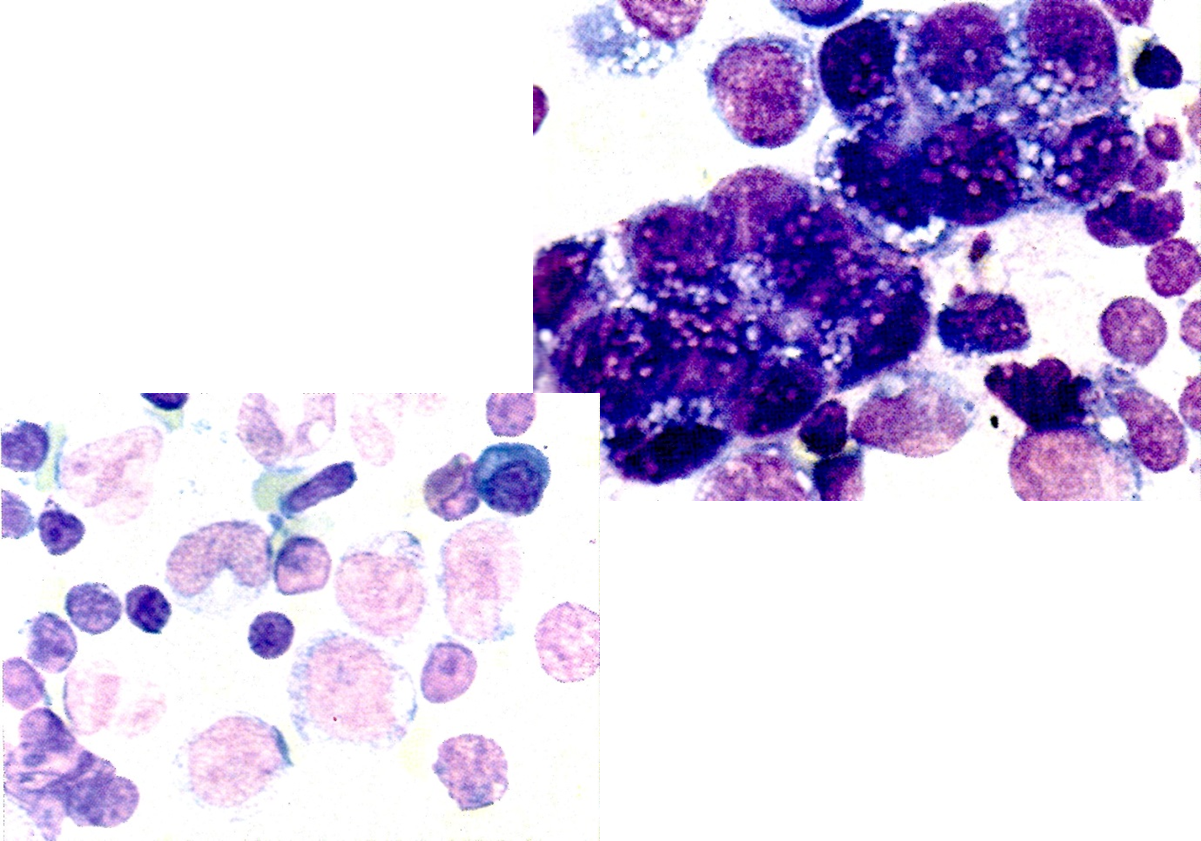
Metastatic neoplasia to ln
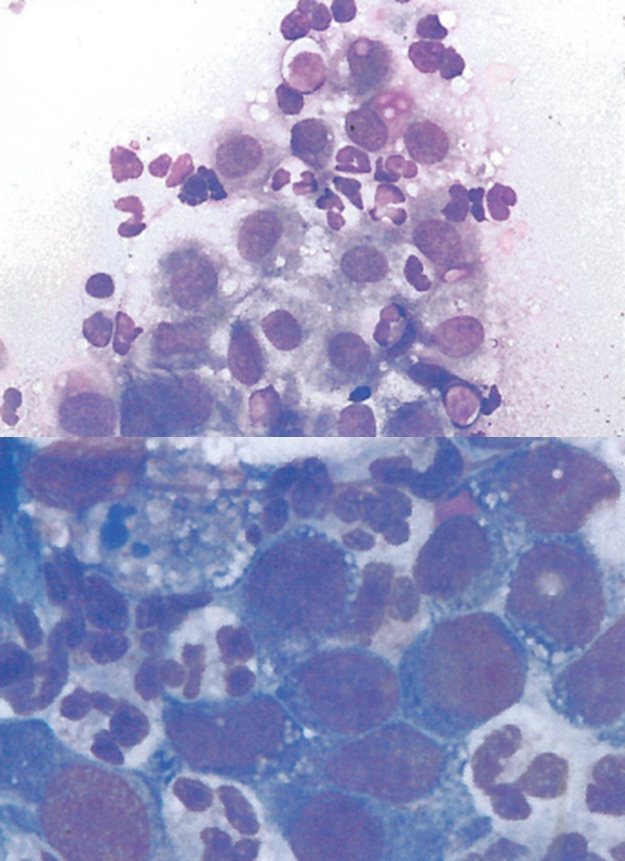
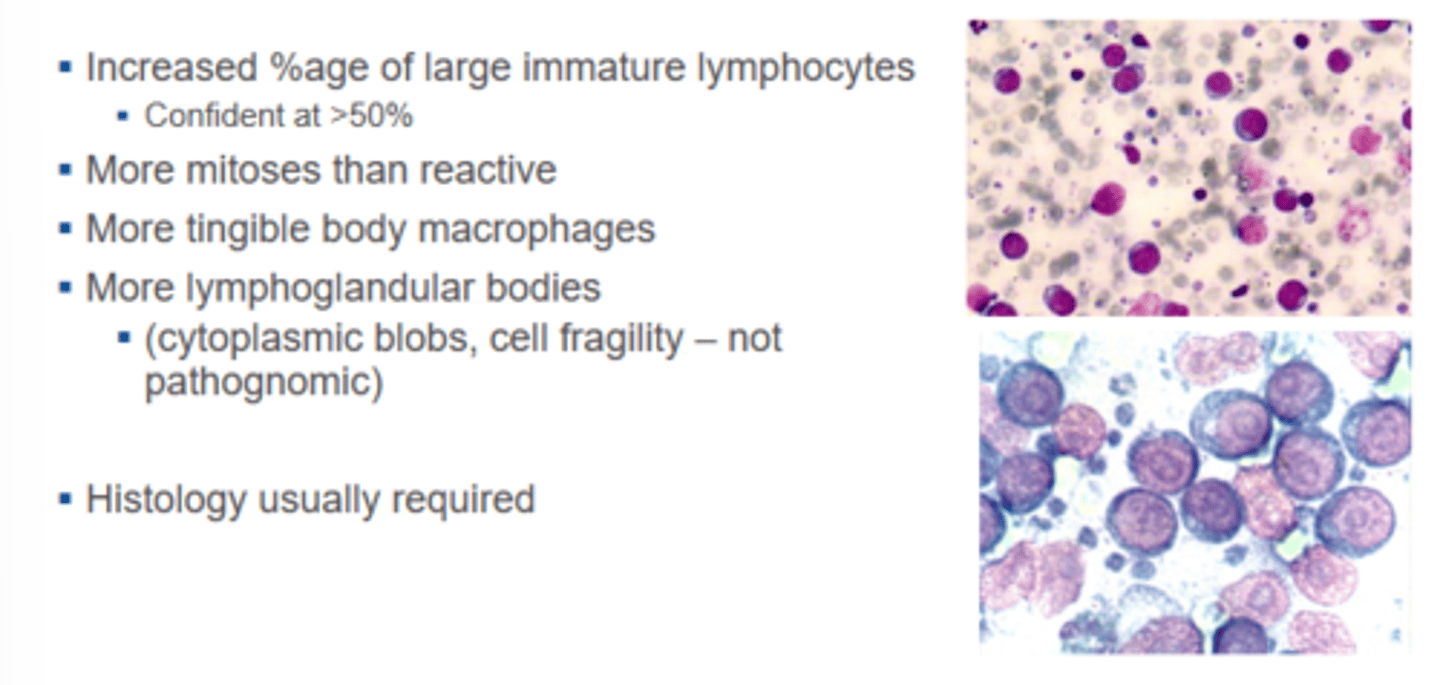
What would lymphoma look like?
Increased %age of large immature lymphocyte
confident at >50%
More mitoses than reactive
More tingible body macrophages
More lymphoglandular bodies
cytoplasmic blobs, cell fragility – not pathognomic
How do you differentiate lymphoma from reactive hyperplasia?
Lymphoma: Increased large, immature lymphocytes (>50%), more mitotic figures, and more tingible body macrophages.
Reactive hyperplasia: Predominantly small lymphocytes (>75%), few mitotic figures, occasional plasma cells.
what is usually needed for lymphoma
histology
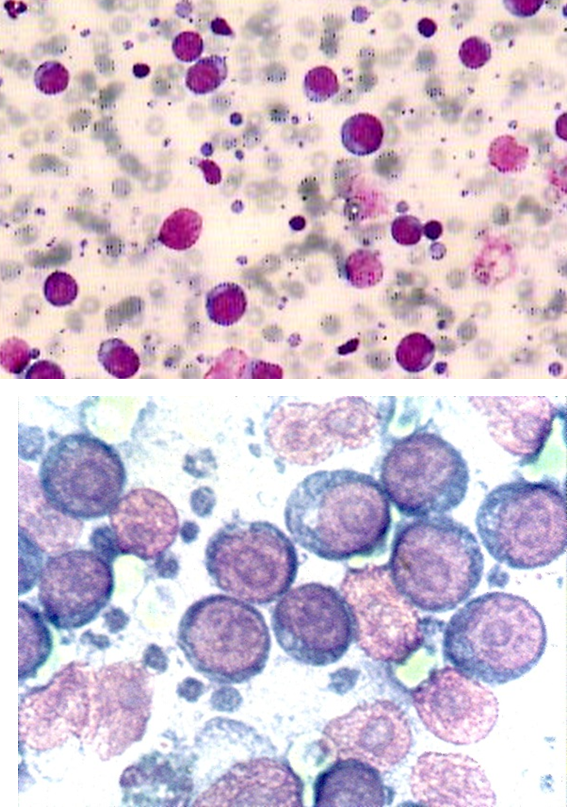
whats this
lymphoma
what are tingible body macrophases
are large phagocytic cells that have numerous
bits of phagocyto's nuclear debris called tingable bodies.
These are also seen in reactive hyperplasia, but more may
be seen in lymphoma.
what are lymphoglandular bodies
are the little blue dots scattered in between cells.
They are burst cytoplasm that then reforms into little blobs
where the phospholipid bilayer has membrane of the outer cell
wall just loops back on itself and makes a little bleb of cytoplasm.