Health Behavior Exam 1
1/108
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
109 Terms
Health Behavior definition
-Those personal attributes such as beliefs, expectations, motives, values, perceptions, and other cognitive elements; personality characteristics, including affective and emotional states and traits; and overt behavior patterns, actions, and habits that relate to health maintenance, to health restoration, and to health improvement
-The actions of individuals, groups, and organizations as well as their determinants, correlates, and consequences, including social change, policy development and implementation, improved coping skills, and enhanced quality of life
*don’t just study the individual level anymore; example groups: college students; example policy development: city bike lanes; end-game=quality of life
3 categories of health behavior
-Preventative
not a big focus for sometime; preventive screening big increase recently
ex: vaccinations, wash hands, exercise, healthy eating
-Illness
when somebody feels like they are not well and does an action to identify a remedy
ex: “I’ll go to WebMD and enter my symptoms to see if I need to go to the doctor”
-Sick-role
somebody knows they are sick, and does things w/ the intention to get better
ex: take medication, go to PT for torn ACL
*barriers all 3: financial/socioeconomic, knowledge. values, motives
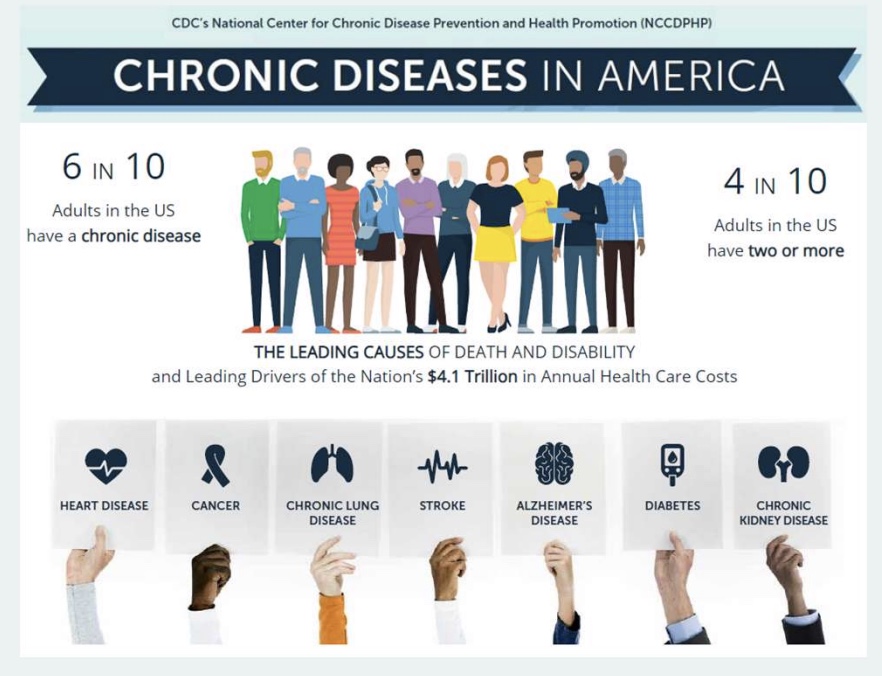
chronic disease in America (#’s and shifts)
-6 in 10 adults have a chronic disease; 4 in 10 adults have two or more
main cause of death and disability
-shift in HB bc shift in disease in our society (more chronic disease), so HB imp bc chronic disease requires ongoing decisions
key lifestyle risks for chronic disease
-Tobacco use: #1 association w/ chronic disease
-poor nutrition
-lack of PA
-excessive alcohol use
*higher interest to understand lifestyle factors; CDC and HHS

what behaviors have changed? (improved and worst)
Improved
-less smoking
-BP and Chol (use more statins)
-more water? knowledge on meds
Worst
-more OW and obesity
-lower vaccination rates
-transportation/lifestyle PA; more UP food and access to it
opportunities and challenges of HB
-opportunities: better and well-rounded understanding of factors that affect HB (ex: obesity, food, DM); more resources available
-challenges: social media and AI lack of accuracy and evidence based info
*social media and AI can fall into both
major challenge of HB
-dissemination of information (*=spreading of information)
The knowledge gained from research using theory is not often actually shared in practice, which leads to not much evidence-based practice
-Research shows most way to change behavior is theory base; research used to understand theory but general people have limited understanding in research; disconnect between research and practice getting bigger, and practice hard to put into play

theory definition
-Set of interrelated concepts, definitions, and propositions that present a systematic view of phenomena by specifying relations among variables, in order to explain and predict the phenomena/HB
how do we use theory?
-Planning: plan strategy for change
-Implementation: shape plan for person so get change
-Evaluation: how do we know it was beneficial? what measure or monitor?
*theory answers why people not following health advice, and what we need to know before do intervention
3 types of theories
-Explanatory Theories (theory of the problem)
• Describe and identify why a problem exists
• Can we predict behaviors under defined conditions?
*how do we know? can we explain?
-Change Theories (theories of action)
• Guide development of interventions
• Basis for evaluation
*did the program work?
-Implementation Theories
• Subcategory of Change theories linked to specific context
concepts vs constructs vs variables
all different!…
-Concepts: The major components of a theory - building blocks
*ex: self-efficacy main concept
-Constructs: concepts adapted or developed for a particular theory
*ex: attitude adapted based on theory
-Variables: operational forms of constructs
*ex: how measure self-efficacy? subjective, questionar, objective?
Models definition
Informed by multiple theories to help understand a specific problem in a particular context
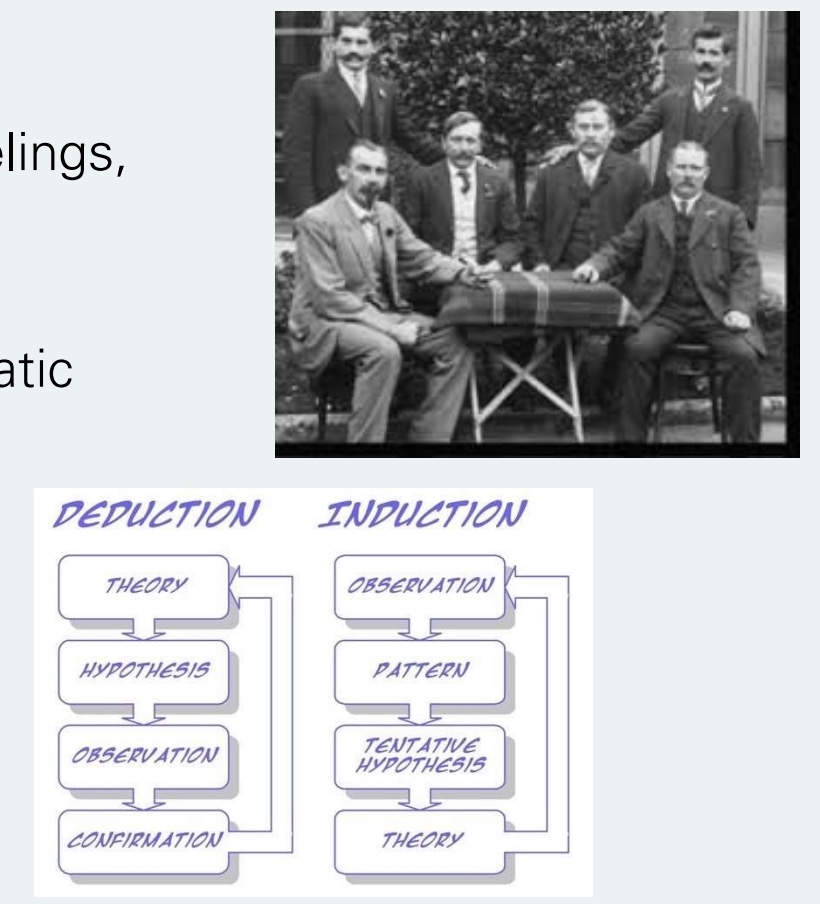
Logical Positivism (Empiricism)
-Emphasis on sensory experiences, feelings, and personal judgments as sources of knowledge
-Use of empirical methods and systematic observation
-Induction seen more often than Deduction, but push to reconcile the two
*Developed in the “Vienna Circle”; Theory gives way to intervene; how do we know what we know?
Types of Research: Quantitative vs Qualitative
-Quantitative research: systematic empirical investigation of a phenomenon via statistical, mathematical, or numerical data or computational techniques
*most common; Pro= easier to do, can get larger #’s of people
-Qualitative research: collecting, analyzing, and interpreting non-numerical data; used to study verbal descriptions of intangible or subjective variables related to human behavior and experiences
*example=interviews; Pro= deeper understanding
Types of Research: Systematic review vs Meta-analysis
-Systematic review: literature review focused on a particular research question with the aim to identify, appraise, select, and synthesize all high-quality research evidence relevant to that question
-Meta-analysis: statistical method of reviewing a body of research evidence that is both systematic AND quantitative
uses “effect size” stats
Interpretation of Effect Sizes and Benchmarking
Effect Size
-gives general understanding/overall impact of an intervention
-Cohen (1992) guidelines:
• Small: d = 0.20 to 0.49
• Medium: d = 0.50 to 0.79
• Large: d = 0.80 or greater
*indicates practical importance of a value by quantifying how much of an impact an intervention has; dif than a P-value
Benchmarking
-Description of effect sizes in real-world terms (e.g., steps taken or percentage increase)
*limit: research connects #’s to outcomes???
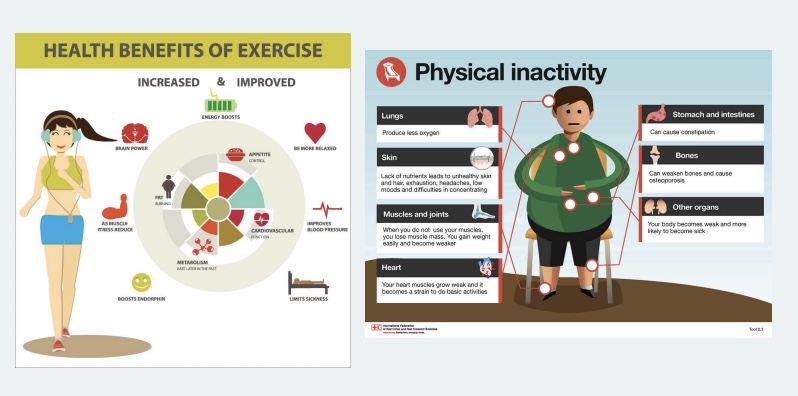
the Tomato Effect
-Phenomenon whereby highly efficacious therapies are either ignored or rejected
3 Charactersitics
Is PA good for us?
Are people aware and accepting that PA is good for them?
Are people physically active?
*background: more people use to not like tomatoes bc were afraid they were poisonous
definition PA vs Exercise
-PA: any bodily movement that increases energy expenditure/metabolic demands above resting conditions and involves the contraction of skeletal muscles
-Exercise: planned, structured, and repetitive physical activity with the goal to improve fitness
*dif factors and attitudes for both
umbrella term of PA
-exercise
-occupational PA: associated w/ a job (ex: mailman)
-transportation PA: move body from one place to another (ex: walk to class)
-leisure PA: examples include gardening, cleaning, walking with a friend
*more emphasis recently on lifestyle PA
exploring the PA tomato effect: is PA good for us?
yes!
-have data/evidence that get benefits from PA; this data led to the guidelines of 150 min/week of moderate and 75 min/week of vigorous PA
exploring the PA tomato effect: Are People Aware and Accepting that PA is Good for Them?
yes!
-94% of Americans reported that PA provides health benefits
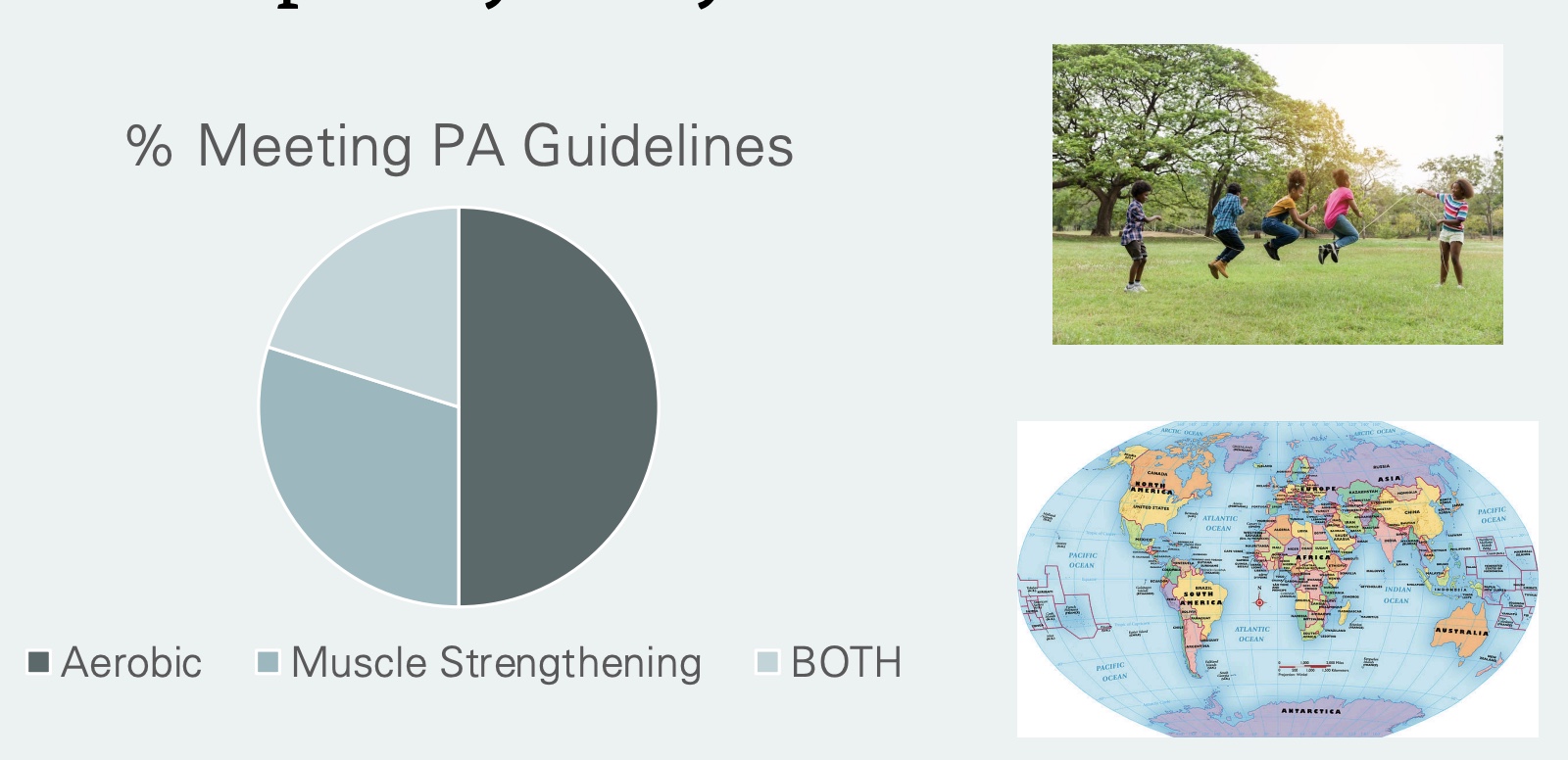
exploring the PA tomato effect: Are people physically active?
no, not the majority
-Of those that do: ~1/2 do aerobic, see small trend increase; strength ~25%; both small proportion
-children: >85% don’t do regular PA
-globally: see similar trends, but Europe has more lifestyle PA
is PA a Tomato Effect?
YES!
-know PA is good for us, is aware of this, yet despite evidence not all do it
*research initially just on exercise and athlete based. Solution?: make it more realistic, lifestyle changes, better understand barriers
*other examples: screen time
PA Psychology definition
-Science devoted to gaining an understanding of human physical activity
*to examine and find research of PA, and form guidelines to help people become more active (how get people to be active); attitudes, moods, feelings, social and envionrmental factors, etc.
-outside EXPH
PA Psychology history/shifts
-Norman Triplet: early philosopher of PA psychology. noticed people faster if biked with another person (not conscious; similar experiments and results with kids and racing boats)
-Biomedical model → biopsychosocial model
^(early focus on phys and bio → current focus)
-started late 1800’s, but no growth until 1970’s. Slow development bc now better understand PA behavior, no just focus on athletes
-Social Facilitation: being with other people matters, will work harder if around others
what influences PA?
Dr. B
-demographics
age: less as age
sex: more if male
education: higher if more (likely bc know benefits, have more resources and $, more free-time)
-enjoyment, motivation
-envionrment and weather
-social support
Class
-motivation for fitness; knowing health benefits of PA, social, role models, enjoyment
Correlation vs Causation
Correlation
-two things associated with each other, often observe; strong or weak
-easier to do, so have most data from, but not the best
Causation
-one thing causes another to happen
-RCT most common
-gives stronger evidence
If you were asked to plan an intervention to reduce the gap of inequality in levels of PA between women and men, what intervention would you design and how would it help reduce the gap?
-women only exercise group or gyms
-coed options, more equal #’s or opportunities (title 9)
-encouraged at younger age
-more aware of benefits
-women rolemodels
*theory allows us to understand barriers, fears, etc.
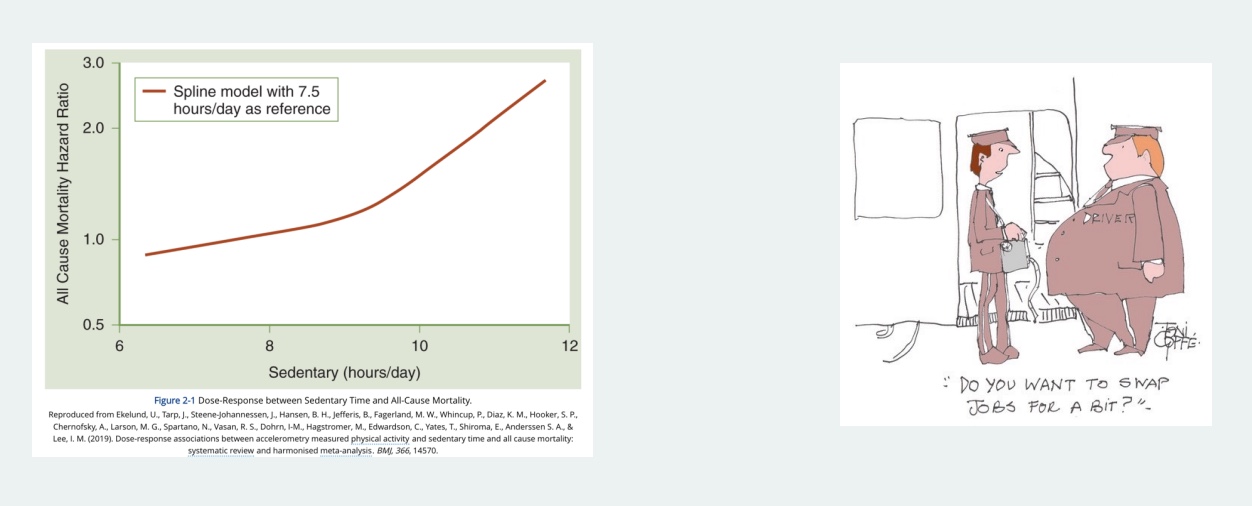
Sedentary Behavior definition, history, and health related outcomes
-Any waking behavior characterized by an energy expenditure <1.5 metabolic equivalents (METs) while in a sitting or reclining position
*doesn’t include sleep; 1MET=3.5ml/kg/min
-Associated with multiple negative health outcomes: increase SB leads to increase in all-cause mortaltiy
-Less research in general bc relatively new; “sitting the new smoking?”; see increase % time SB > time sleeping
*London Bus Study: drivers who sat more than ticket takers had more HD and OW/obesity
prevalence of sedentary behavior
-Systematic review of 125 studies examining sedentary behaviors of college students
• ~7 to 10 hours being sedentary
• Computer use was the most common (so not always bad)
• SB may be on the rise (transition as a society)
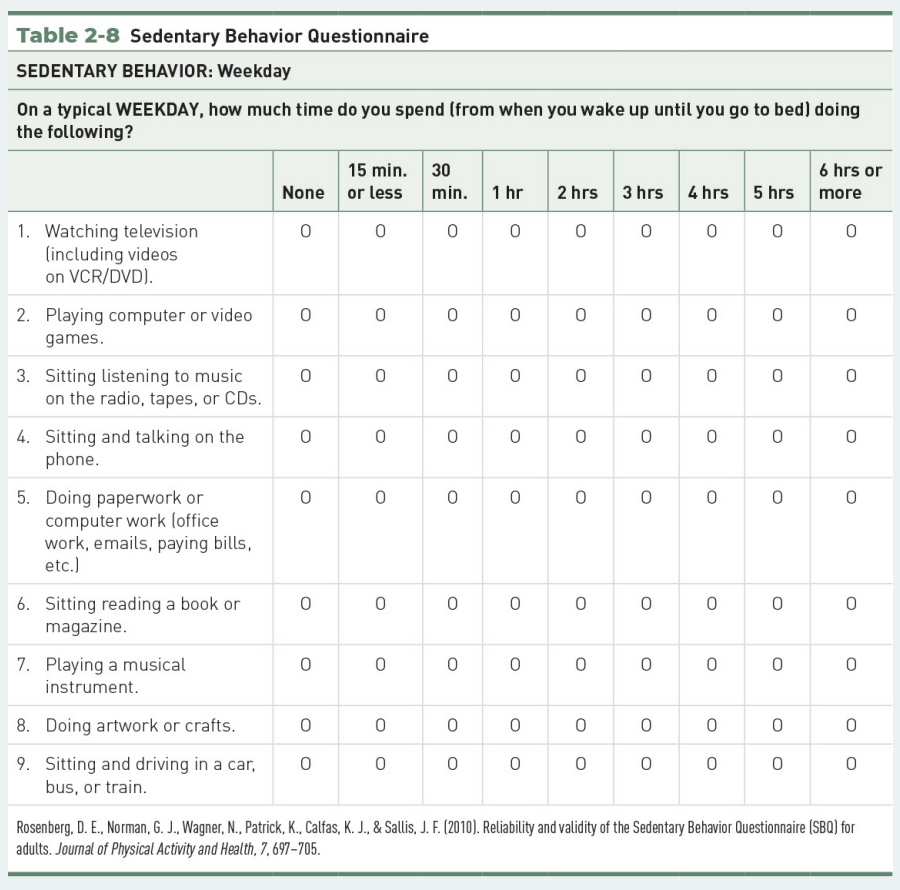
Measurement of SB
Accelerometer
-gold standard, and getting better
-measures steps AND intensity/speed (higher intensity= more beneficial)
-most accurate if worn on the hip
-doesn’t tell difference sleeping and sitting
-examples: Applewatch
*vs a pedometer: wear on hip and just counts steps

true or false: it is easy to measure SB
false!
-it is hard to measure SB, bc can be doing dif things
-+ objective measures of SB elicit higher levels of SB than subjective measures (aka people underestimate how much time they are sedentary)
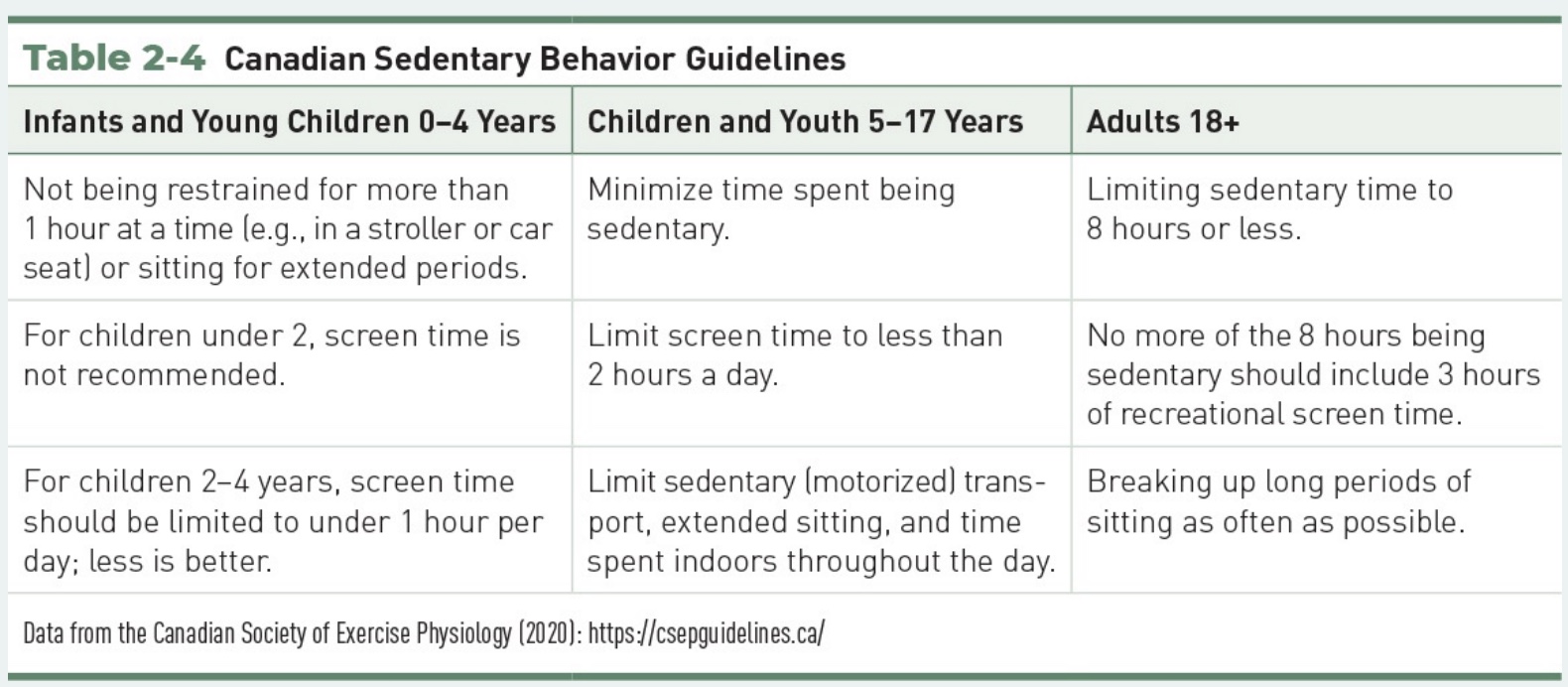
true or false: the U.S. has SB guidelines
false!
-The U.S. does NOT have SB guidelines
this is bad and good (good bc no strong evidence of what guidelines should be)
-but, Canada does have SB guidelines
*have more evidence that SB causes negative health benefits, so goal should be to meet guidelines and lower SB
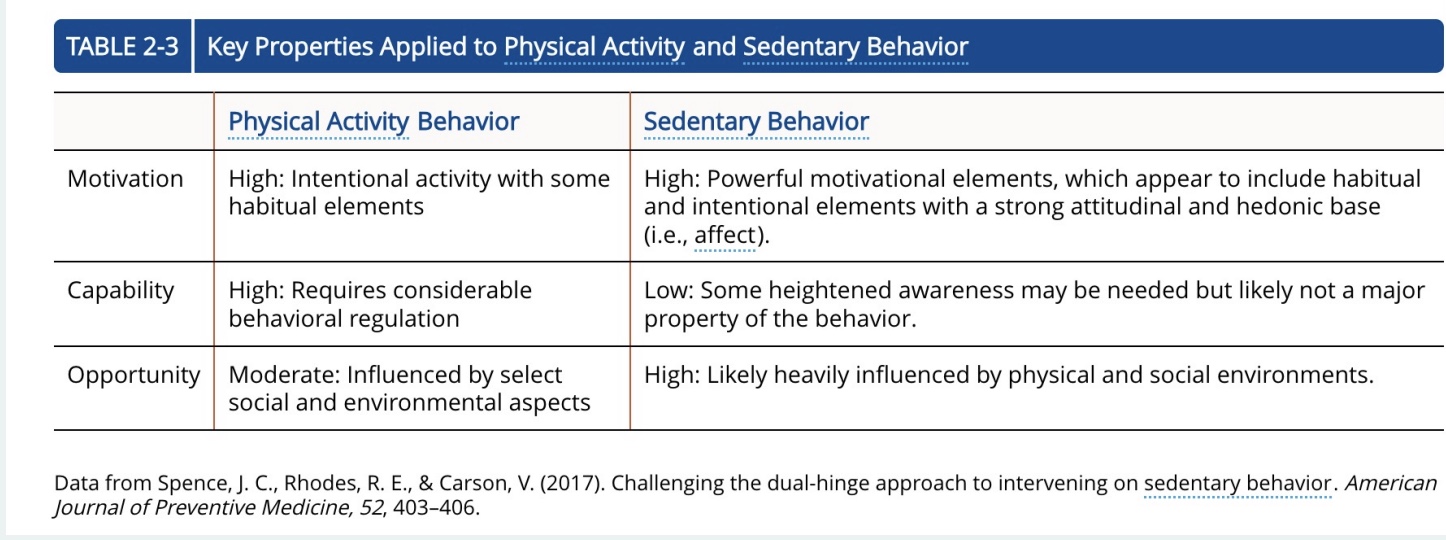
is PA the same as SB?
NO! PA does NOT equal SB
-PA=don’t meet 150/75 min guidelines
-SB= <1.5 METS
-+ differences in motivation, capability, opportunity, and more
How might the correlates for sedentary behavior and physical activity differ?
*2 dif behaviors w/ common correlates, and dif than exercise
-increase SB as age
-no dif sex and gender
-socioeconomic: increase PA if $, mix evidence for SB (blue collar limits SB more than white collar)
-family life: lower PA and SB if have kids
-occupation (manual labor vs office)
Social Ecological Model
-how people react to their physical, social, and cultural envionrments
*”social”=people, outside and inside; “ecological”=humans interaction w/ the envionrment
-progressive topic; (1960’s) direct effect envionrment and behavior
Social Ecological Model levels
-framework, different levels
-how incorporate different theories and models
-to maximize HB change, need knowledge
-limit: gives idea, but doesn’t tell us which variable to intervene (but a good start)
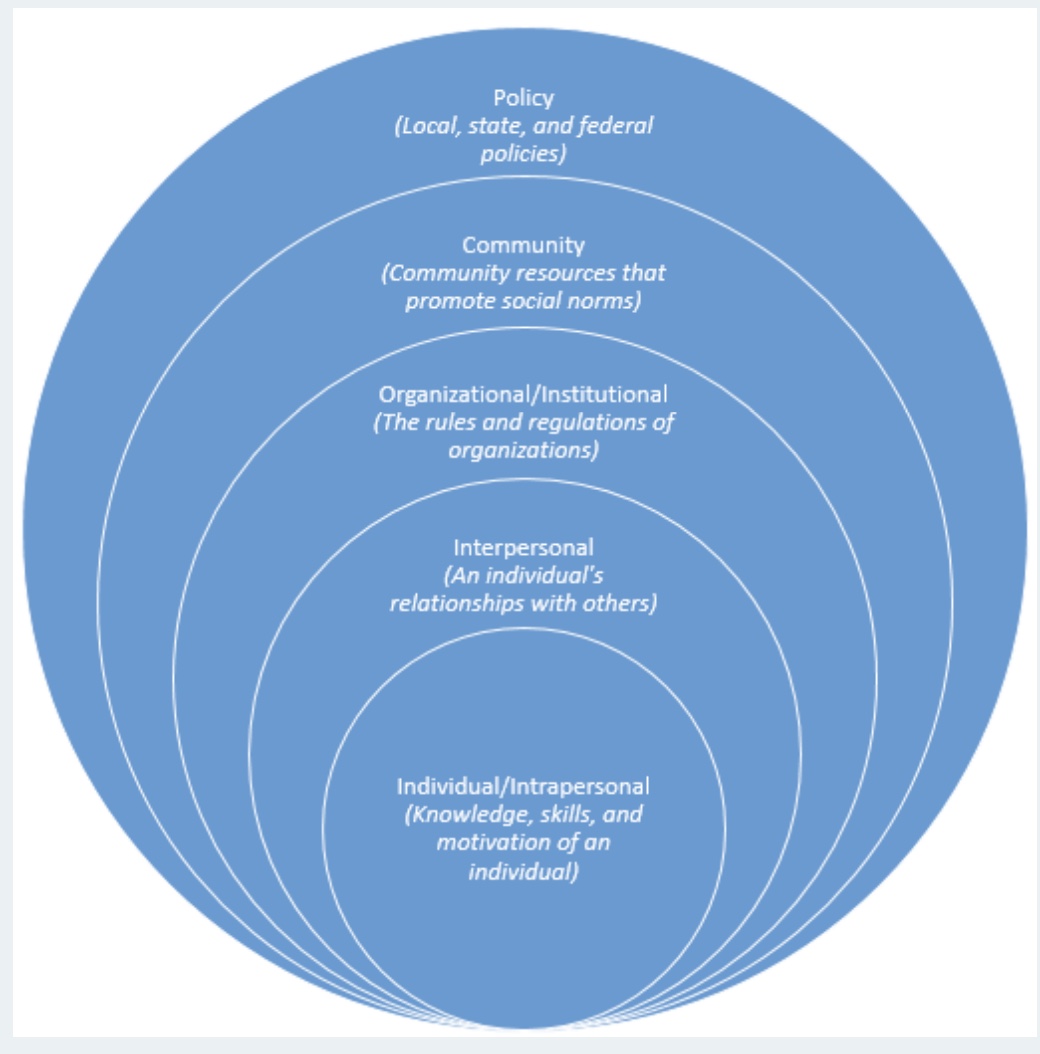
5 Principles of SEM (list)
P1: Multiple levels of influence
-Factors at multiple levels influence health behaviors
-different than other theories bc considers multiple levels
-ex: PA
P2: Environmental context determines behavior
-Behaviors may be better predicted by environmental contexts than by individual characteristics
Behavior settings: social and physical environment
May restrict or promote certain behaviors
*ex: HS vs College and impact on HB
P3: Interactions across levels
-Variables interact to influence behavior

P4: Behavior Specific
-Require tailoring to specific health behaviors
*lessons learned one HB don’t always apply to others
P5: Multi-level interventions most effective
-May promote long-term change AND affect more people
-changing knowledge usually not enough (ex: tomato effect)
*ex: just say increase fruit and veggies in store not enough, also $ problems, etc.; only been a big focus in the last decade
true or false: it is difficult to identify which factor is most important?
true! but targeting all factors more effective than just one alone
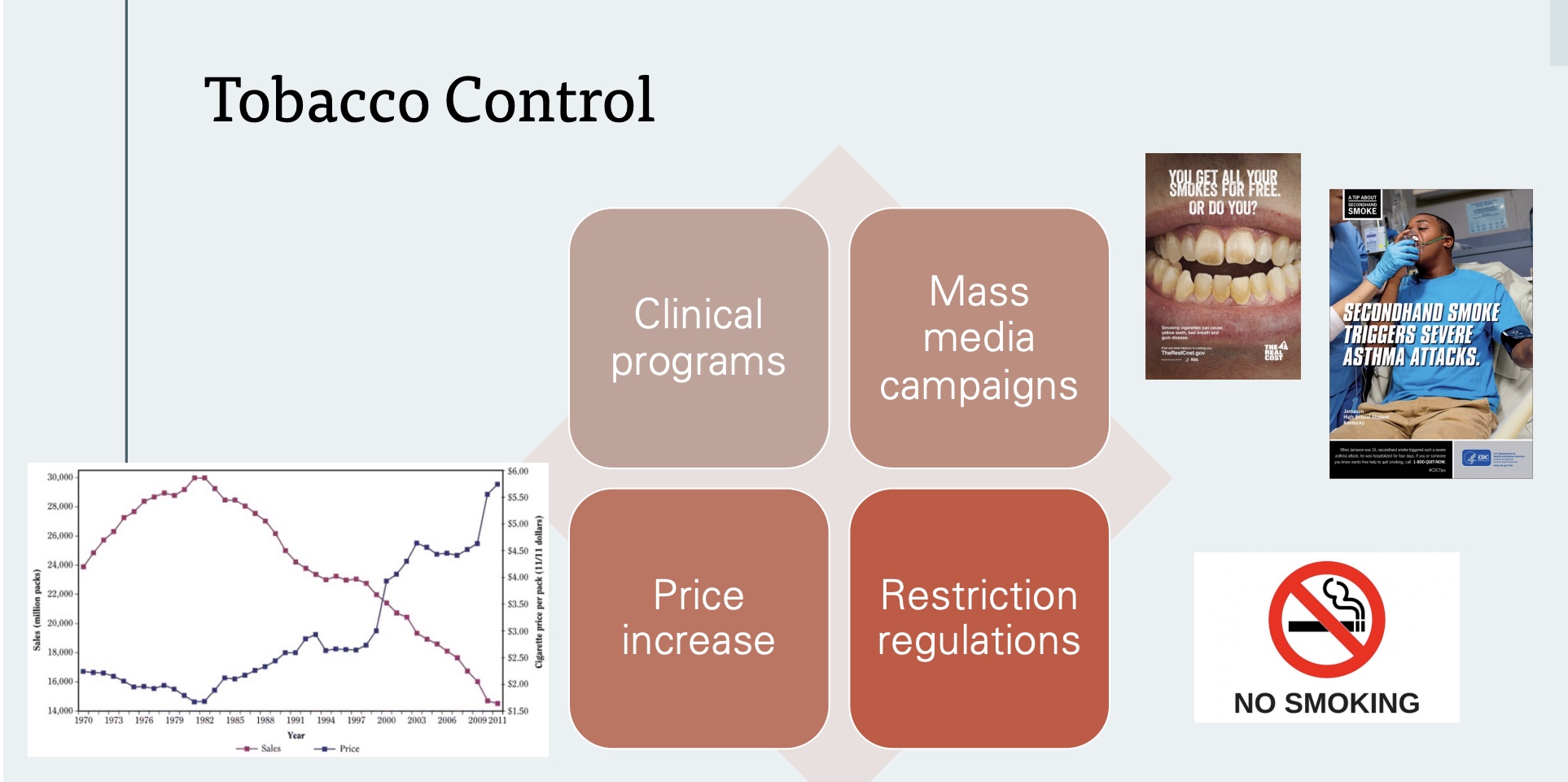
Applications: tobacco control
-big public health victory, bc…
1) Clinical Programs: often where start; education/knowledge, but doesn’t make large change
2) Mass Media Campaigns: individual → envionrmental and policy level; helped people understand negative impacts
3) Restriction Regulations: policy level resrictions; ex=planes, resturants
4) Price Increase: most effective
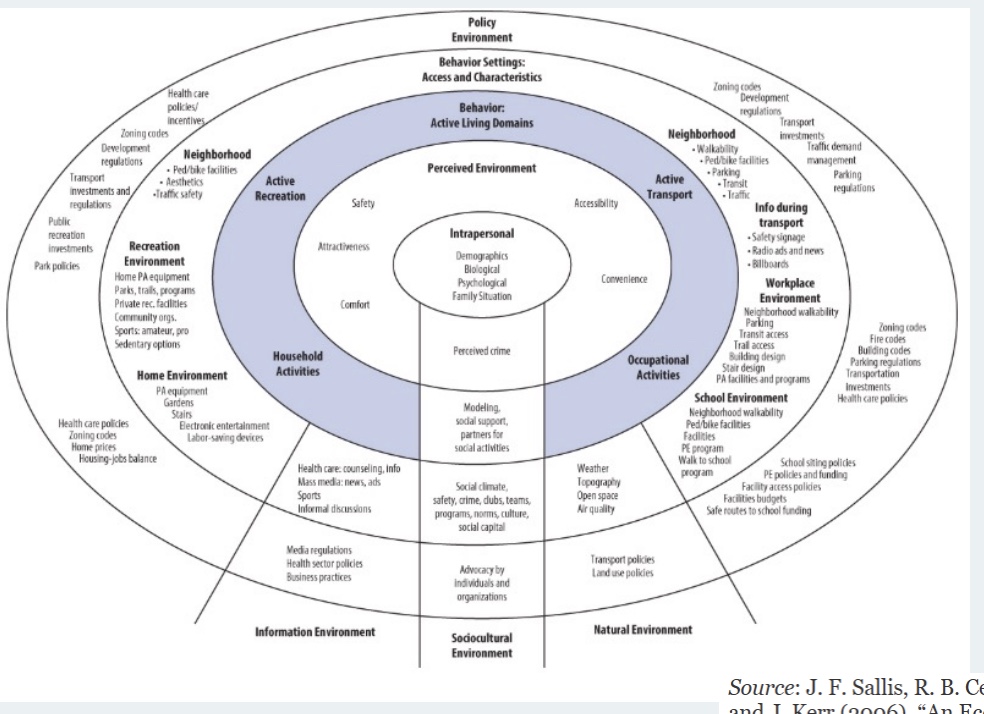
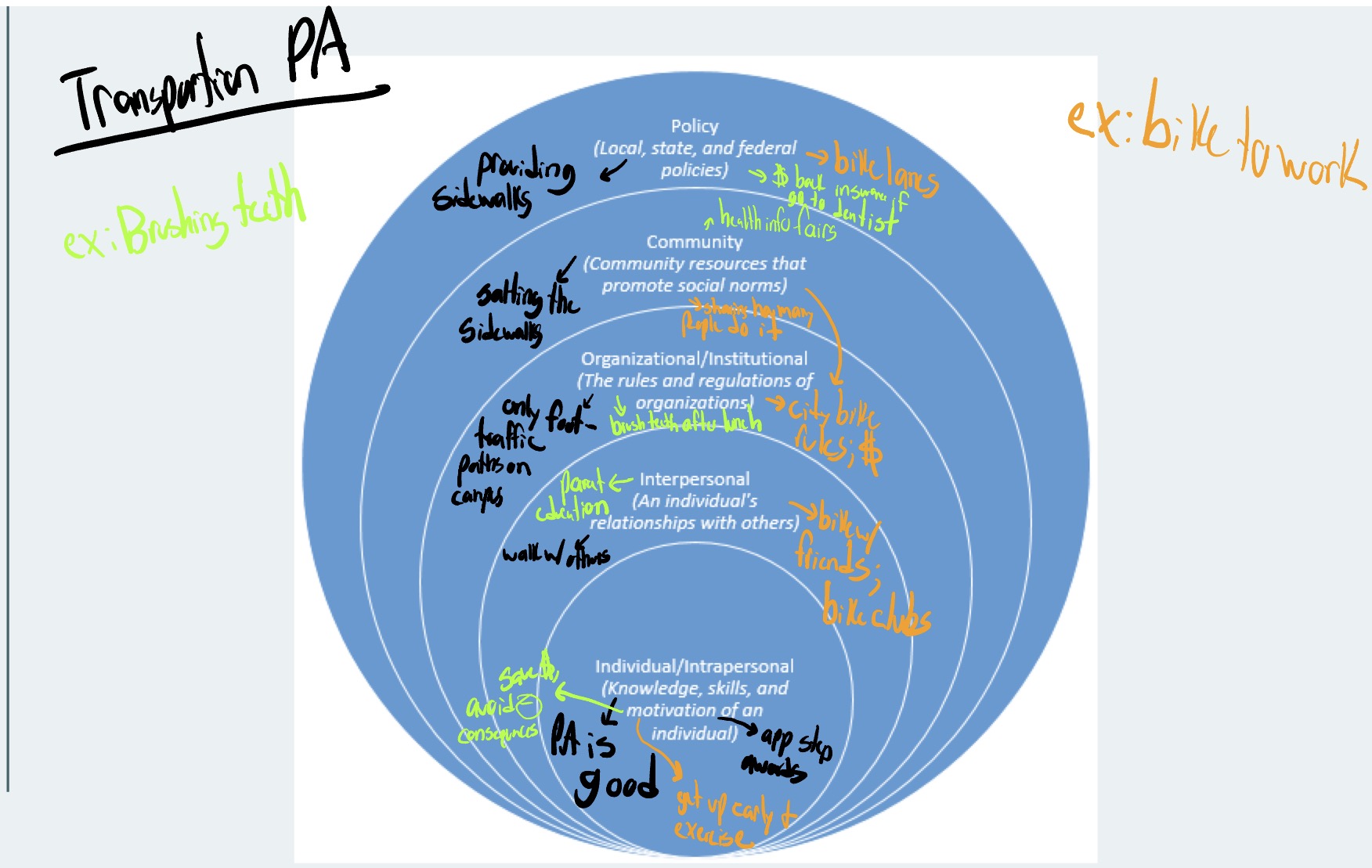
Social Ecological Model Applications: Physical Activity
-different types of activity
-relatively recent idea to focus beyond intrapersonal
-intrapersonal, envionrment, behavior domains, behavior settings, policy envionrment
Applications: Obesity Epidemic
-obesity=characteristic
-on the rise, but why? (mainly PA and diet?)
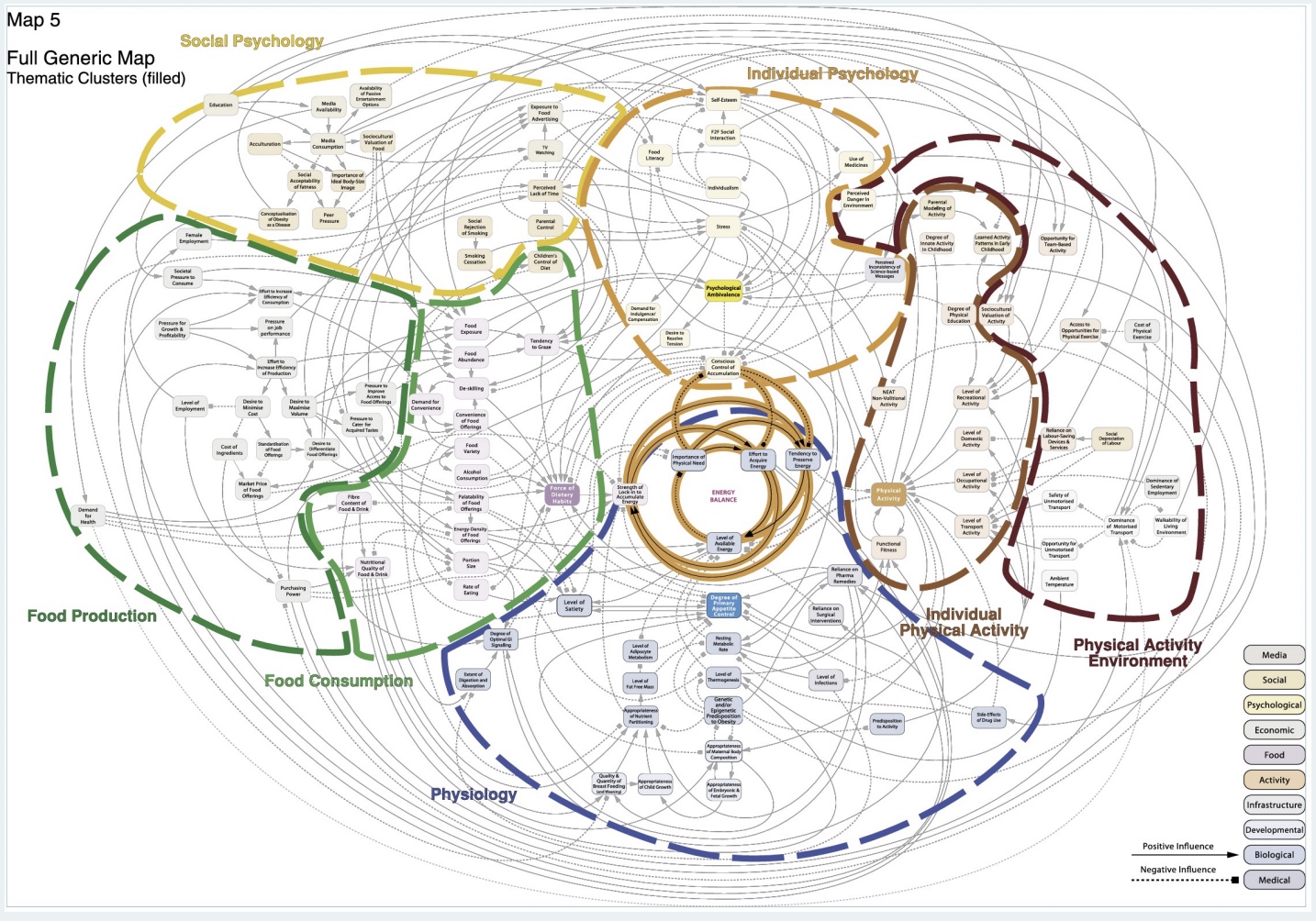
Complex Symptoms Model
-shows many factors that contribute to overall energy balance and increase obesity
-arrows are bi-directional, positive feedback loops
-bottom line: no easy answer!
If you were to design an intervention to change one variable to improve the childhood obesity epidemic in the U.S., what would you choose to target?
-subsidize healthy food/increase access (knowledge not enough; new food guidelines)
-education (for parents)
-after-school fitness programs
-decreased screen time (too stimulating? what is it replacing?)
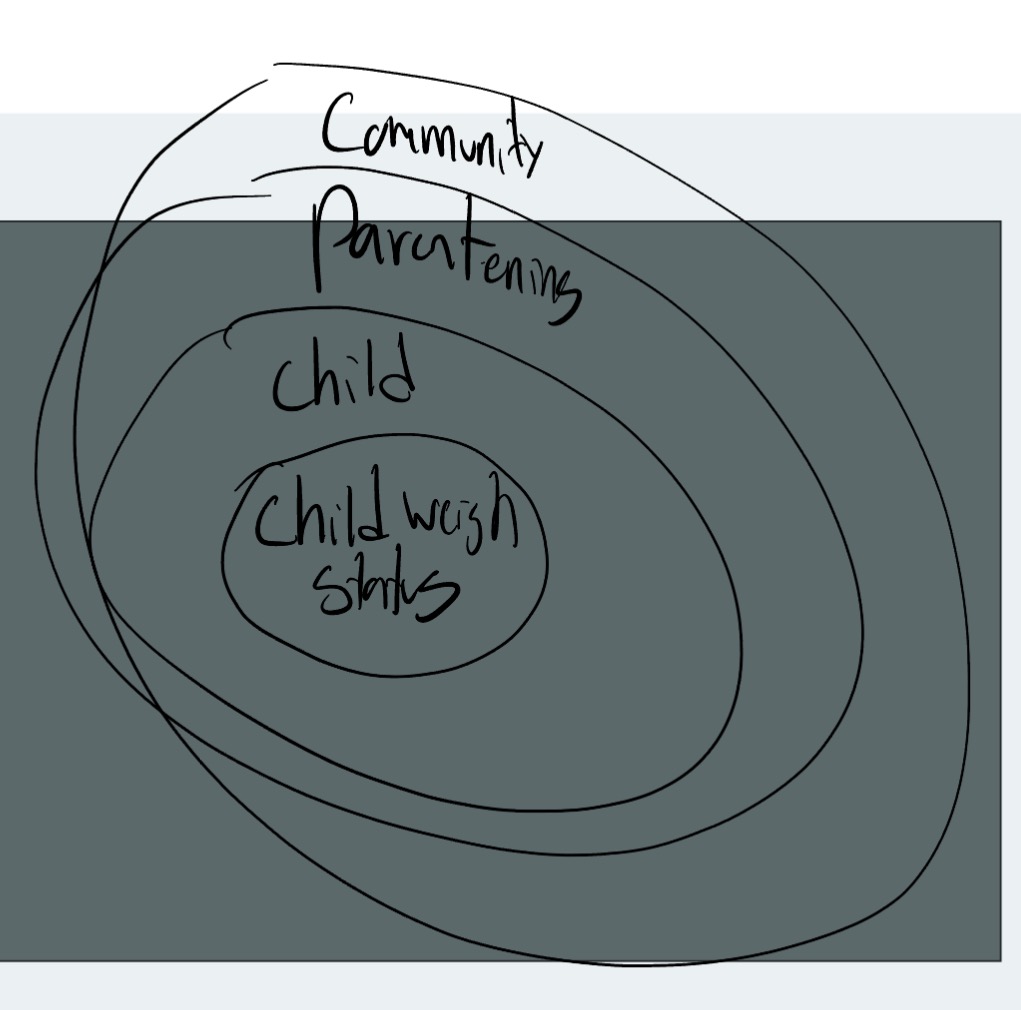
SEM Application: Child weight status
-impacted by the child, parenting, and community
-modifiable and unmodifiable
Class Examples of HB Social Ecological Models
defining personality
-“Individual differences in characteristic patterns of thinking, feeling and behaving”
*not just behavior
-Enduring and consistent across lifespan (*static trait, often stabilize early adulthood)
-Potential biological and genetic basis
-Culturally and environmentally conditioned
history: Socrates
-Four basic types of people (bodily humours)
Sanguine (optimistic)
Phlegmatic (calm)
Choleric (irritable)
Melancholic (depressed)
*400 BC; “Nature of Man”; said people differ
history: Fundamental lexical hypothesis
-Gordan Alpert, 1970’s, “grandfather of personality research”
-Fundamental lexical hypothesis: all important feelings, characteristics, and behaviors are present in our language
*have words to describe it
-Identified 18,000 potential human traits
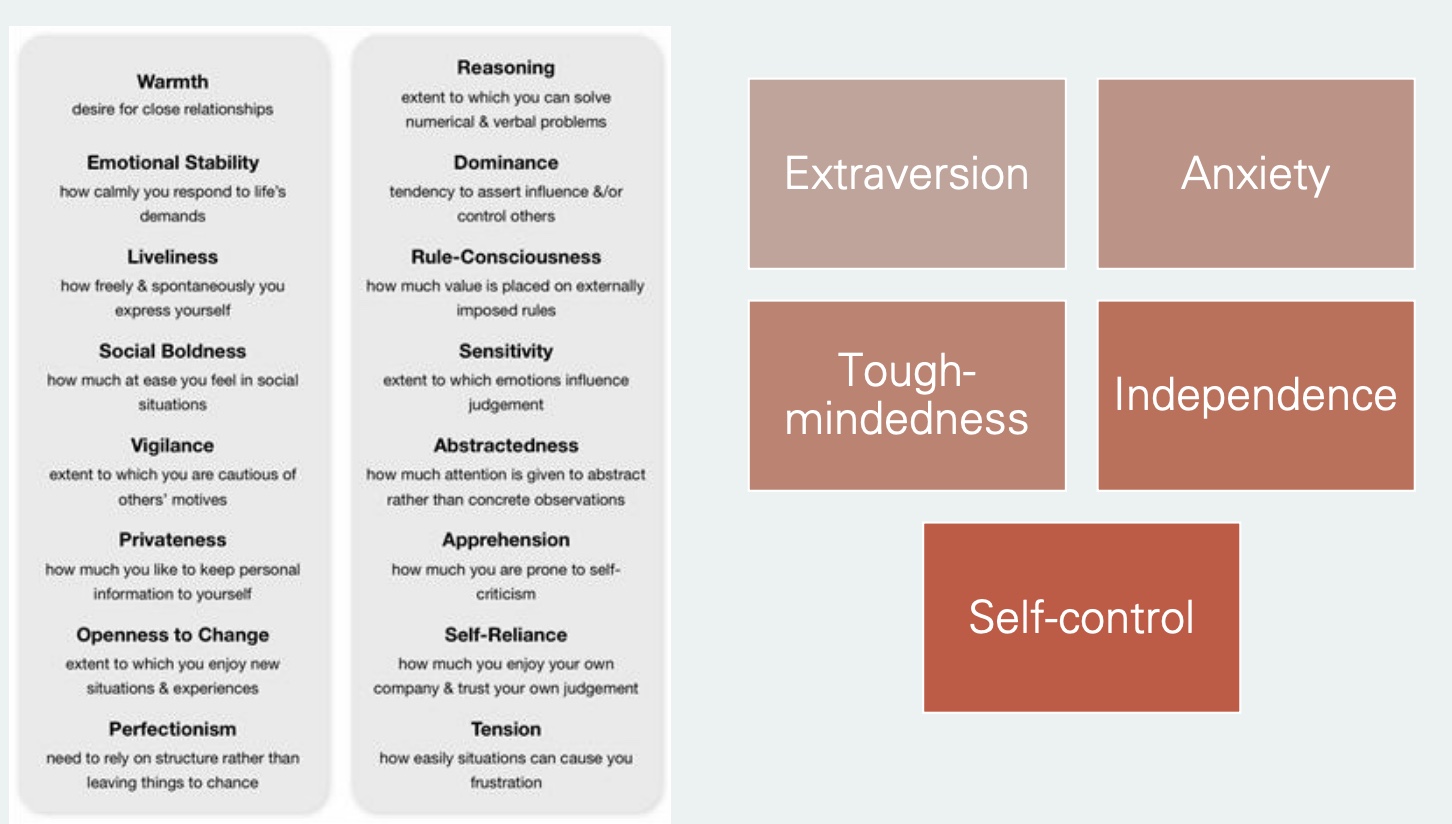
history: Factor Analysis
-break down, some overlapp
-Raymen Contrel, 60’s (18,000 → 16 traits) → 80’s further broken down in to 5
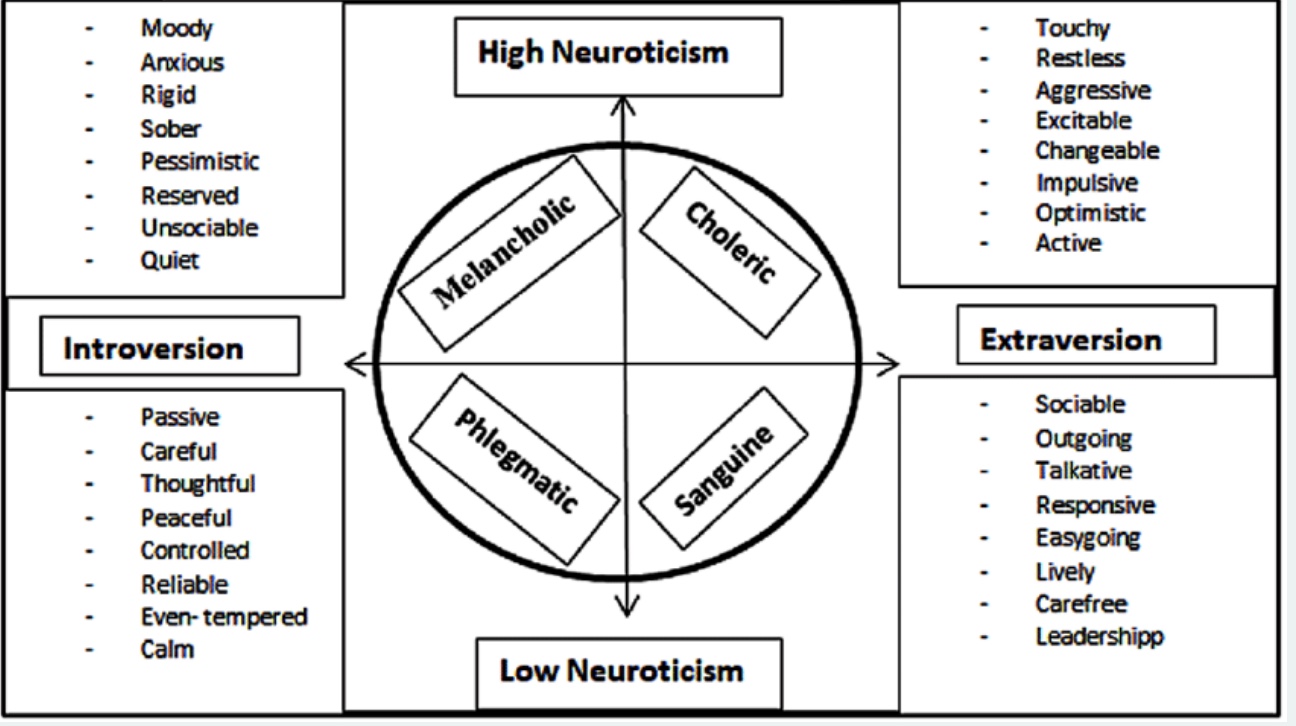
Eysenck’s Theory
-common one
-Neuroticism and Introversion or Extraversion
*neuroticism= emotional stability
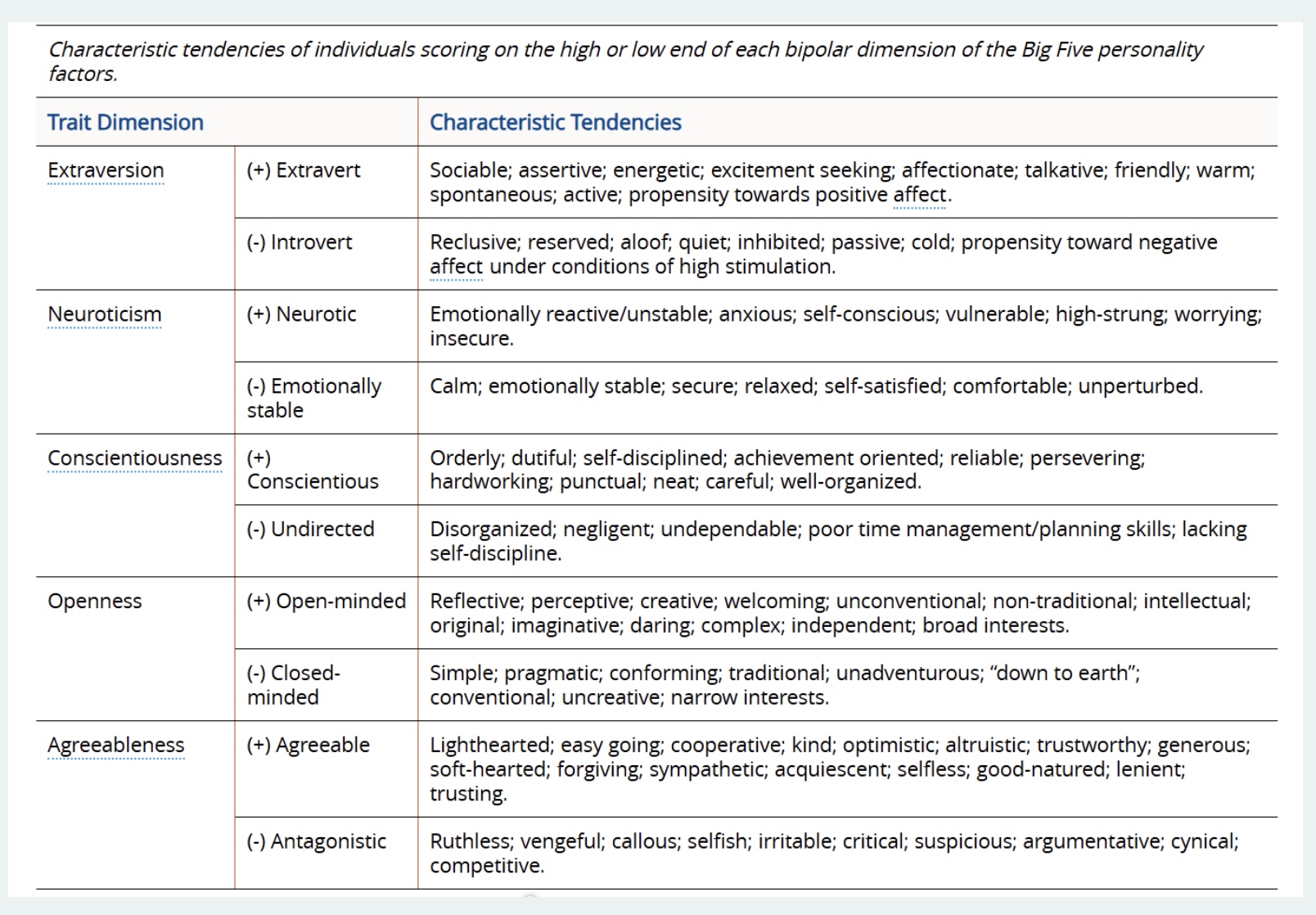
5-Factor Taxomy
-most common
-”OCEAN”=openness, conscientiousness, extraversion, agreeableness, neuroticism
-limit: could fall into both subcategories
Personality and Health: Psychophysical vs Behavioral
*2 ways to think…
-Psychophysical: effect of psychological events on physiological, neuroendocrine, and metabolic processes (*body processes, direct effect)
-Behavioral: overt actions and inactions that influence exposure to pathogenic agents/disease
most research; personality affects health
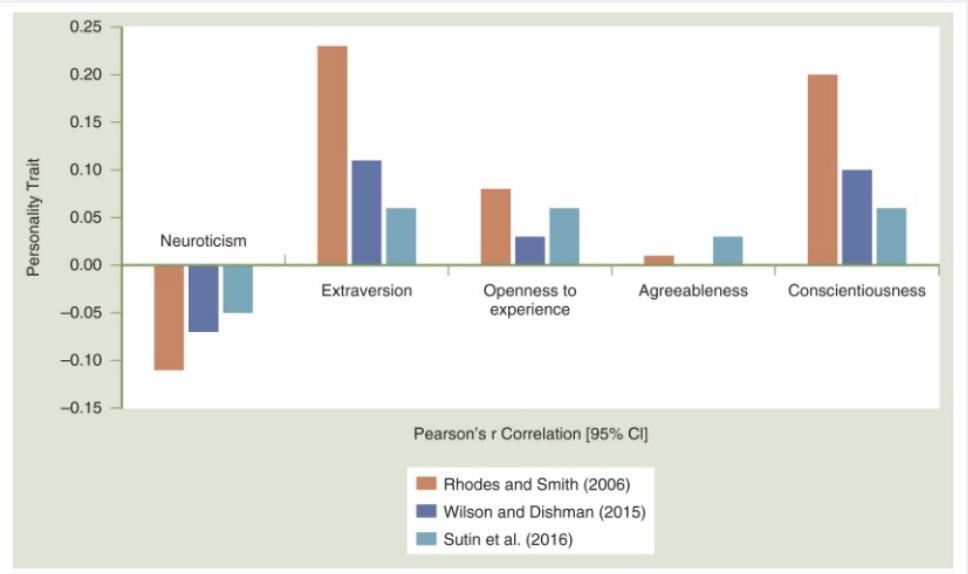
Personality and PA: correlation
-Extraversion and Conscientiousness have positive association w/ PA, though small correlation
Conscientiousness: bc self-disciplined, have a purpose? one of the most imp factors for health (live longer); Extraversion: activity > social facet
-Openness and Agreeableness don’t have a strong correlation
-Neuroticism has a negative correlation
*graph: increase # = increase levels PA; 1=perfect correlation
Personality and PA: extraversion and conscientiousness correlations to PA intensity and frequency
-Extraversion and PA → larger for moderate-vigorous PA (r = 0.13) compared to mild-to-moderate PA (r = 0.04)
*MVPA higher correlation though not strong; bc more sports events, requires more effort; mild-moderate bc more individual activities
-Conscientiousness and PA → larger for frequency (r = 0.21) compared to quantity (r = 0.06) or volume (r = 0.07)
*bc like routines, checklists
Personality and PA: Type A
-Type A personality: positive, small-to-medium association w/ PA
*higher narcotic, extraverted, and consciousness, lower agreeableness
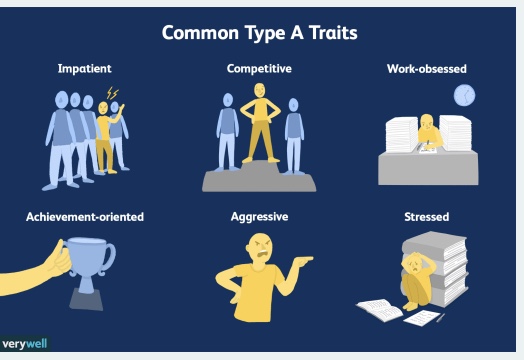
Type A behavior is most well-known for its link to heart disease. What factors may be associated with physical activity and what factors may not?
*factors can differ (positive or negative) depending on the situation
-prone to stress
-workaholic so less time for PA
-want everything perfect, if thrown off plan increase stress
-Higher BP and HR
research on resilience
-new research; ability to bounce back
-positive, but also negative bc in stressful envionrment
why Extraversion link with PA?
activity > sociability
-Activity facet: positive, medium-to-large association
like moving more
-Sociability facet: related but not independent of extraversion
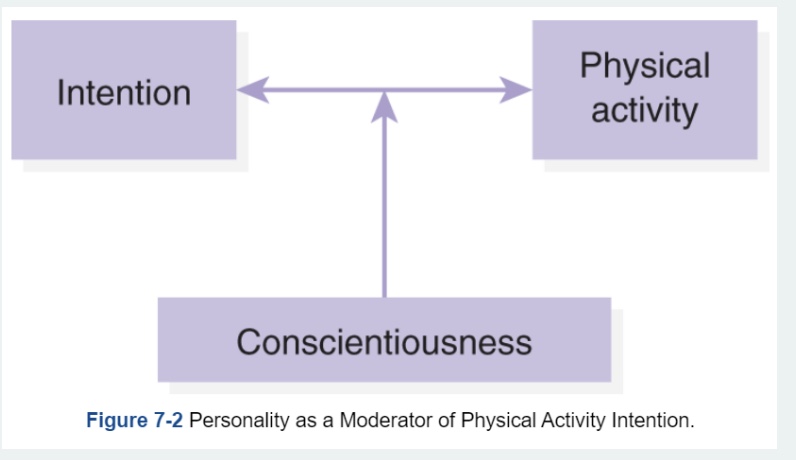
HOW does personality affect PA?
-Personality influences behavioral perceptions, expectations, and cognitions
-more indirect assessments/effects (through other factors such as planning, intention, motivation, etc.)
-”Intension action gap”: breaks down somewhere
intention: pre-cuser to engagement and behavior
conscientiousness: helps keep intention (similar w/ extraversion)
genetics of personality and PA
-Heritability of PA: 48% to 71%
-Heritability of personality traits: 41% to 61%
-Potential link between heritability of extraversion and neuroticism and PA (2 characteristics high association w/ genetic component)
*modifiable, but genetics as well
Longitudinal Associations + do PA and personality affect each other?
-Relationships are fairly stable across the lifespan
-Bidirectional?= Can PA effect personality?… YES! (increase PA improves consciousness)
*overall: easy research, gives correlations, maybe do survey research
how do healthcare providers use these personality data?
-how motivate each patient
-transition health care system biomed → biopsych result in better care?
Personality-matched PA Intervention
-Goal-setting interventions for PA in low conscientiousness individuals
generally a good behavior change strategy for all people; use specific and small goals
-Social comparison apps for high extraversion and neuroticism individuals
-but, some approaches not beneficial for everybody; ex: if motivated by knowing health benefits or negative consequences of physical inactivity differs person to person
*little to no research in practice
what about personality and SB?
-not much data, limited research
-positive correlation neurotic and SB; negative correlation consciousness and SB
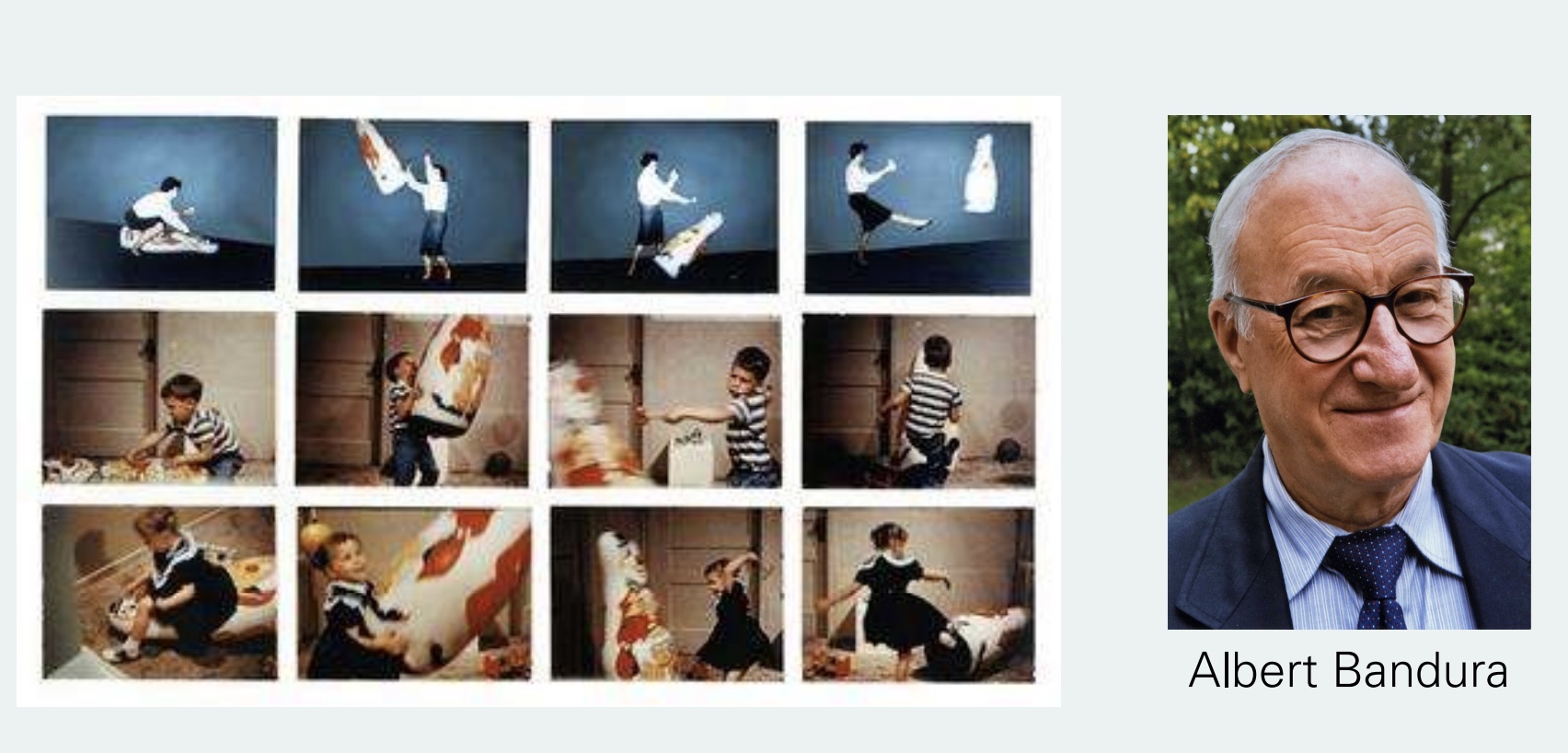
Social Learning Theory
-Bandura, 1977
-Behavior is mediated by cognitive processes that occur through observation of social modeling
*how we learn to engage in certain behavior
-Departure from previous stimulus response models (*ex: Pavlov’s Dogs)
Albert Bandura
-psychologist and researcher; Social Learning Theory
-”Bobo Doll” experiment: 1960’s, showed how learn and why engage in some behaviors, “observational learning”
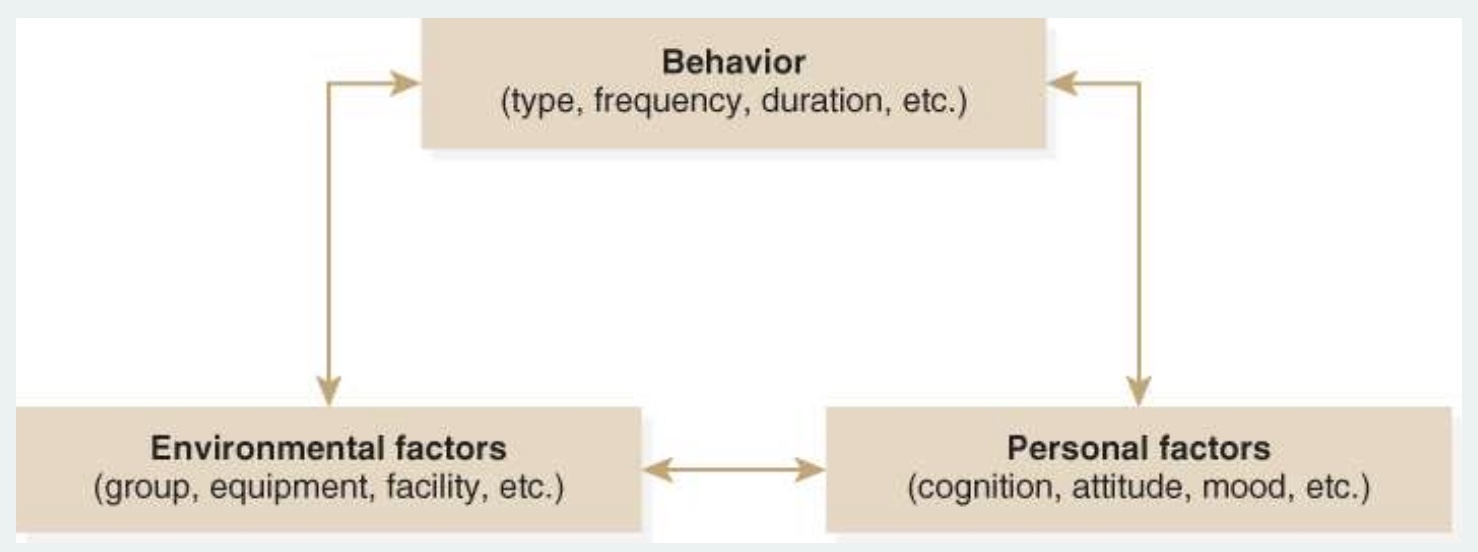
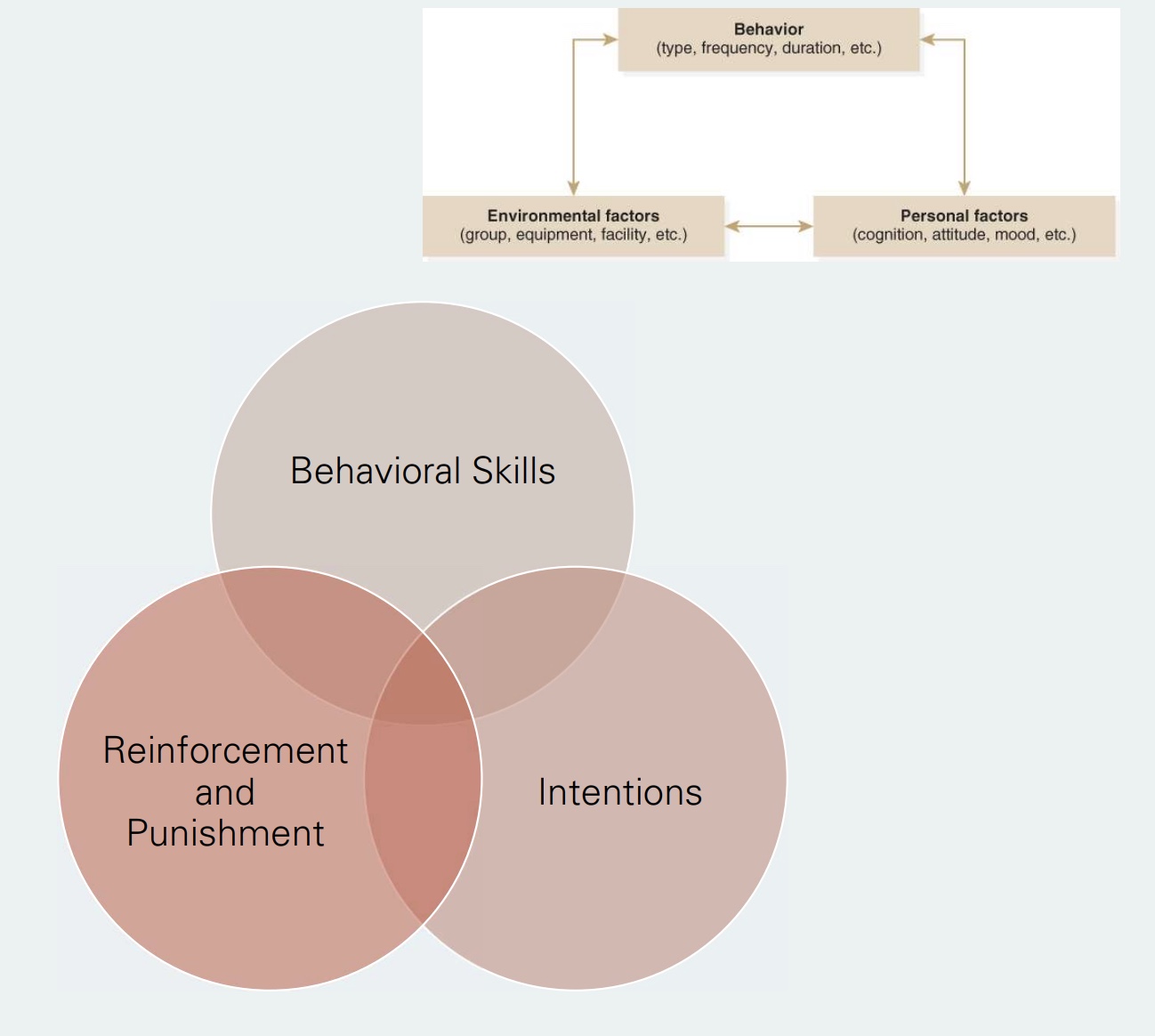
Social Cognitive Theory 3 components/framework
-behavior, envionrmental factors, personal factors
-bidirectional arrows=Reciprocal Determination=affect and interact with each other
Personal Factors (list)
3 strong associations with HB
-self-efficacy
-outcome expectations
-knowledge
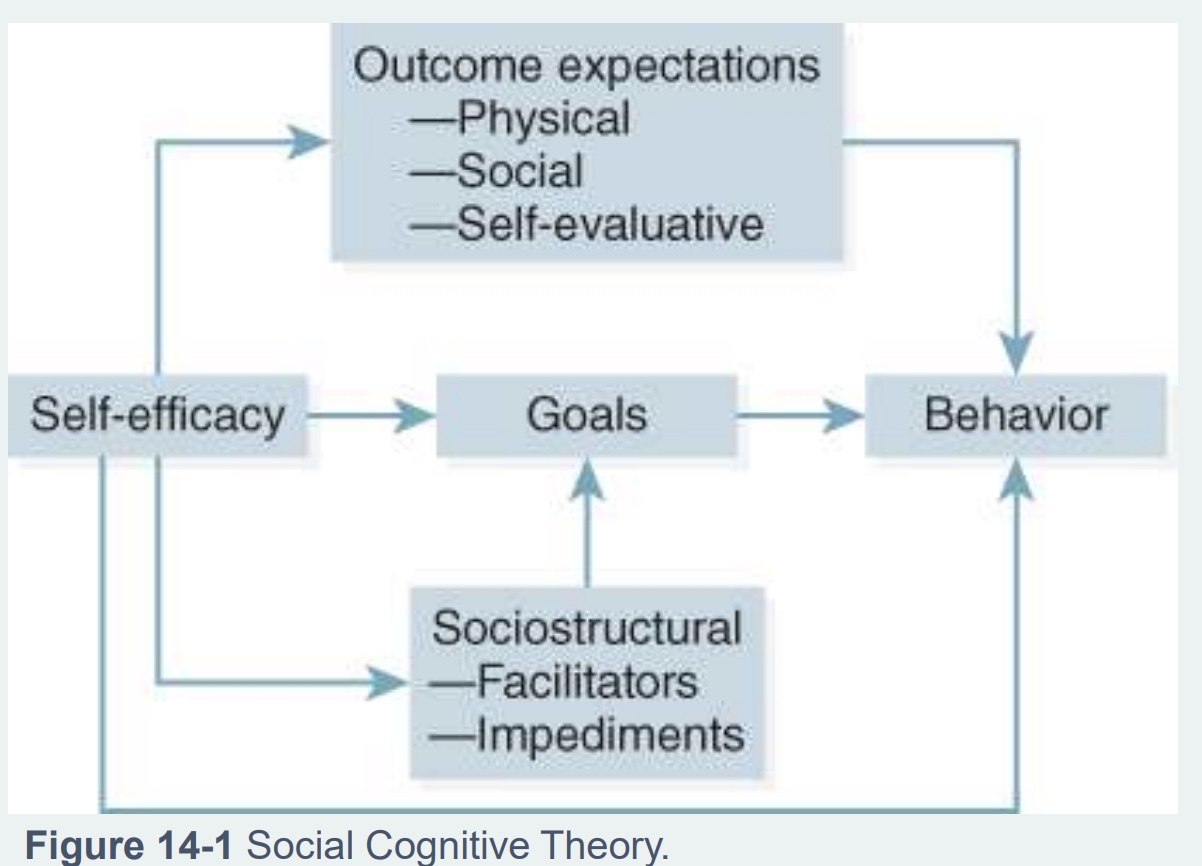
Personal factor: Self-efficacy
-Person’s confidence in ability to perform a behavior that leads to an outcome
-Regulates processes that enhance or impede behavior
*ex: my confidence and ability to walk 20 min vs run a marathon
-picture: self-efficacy impacts multiple things besides personal factor; can we change self-efficacy?=imp w/ patients
Sources of self-efficacy
*can all be changed…
-Mastery experiences: highest source/most imp; previous experience w/ sources; to get there start w/ smaller goals
-Vicarious experiences: see someone achieve success or engage in behavior; individual doing the experience with matters, if more like you/share similarity
-Verbal persuasions: “cheerleader”
*next 2 hand in hand…
-Physiological states: what changes physiologically from engaging in behavior; can be positive or negative (ex: if exercise and increase HR, maybe glad to see HR increasing or worried that higher HR means you’re out of shape)
-Mood states: how feel with certain behavior; “emotional arosel”
Self-efficacy measurement
-Level: belief in ability to do task, yes or no
-Strength: how strongly confident
-Generality: can it be transferred to other task
-Barrier vs. Task efficacy: ability to complete task despite barriers (social, personal, envionrmental) vs confidence completing a task
*research differs on the two
Barrier vs Task self-efficacy
-hard to separate motivation from self-efficacy
-task imp beginning, barrier more overtime
-”I can exercise if I want to”
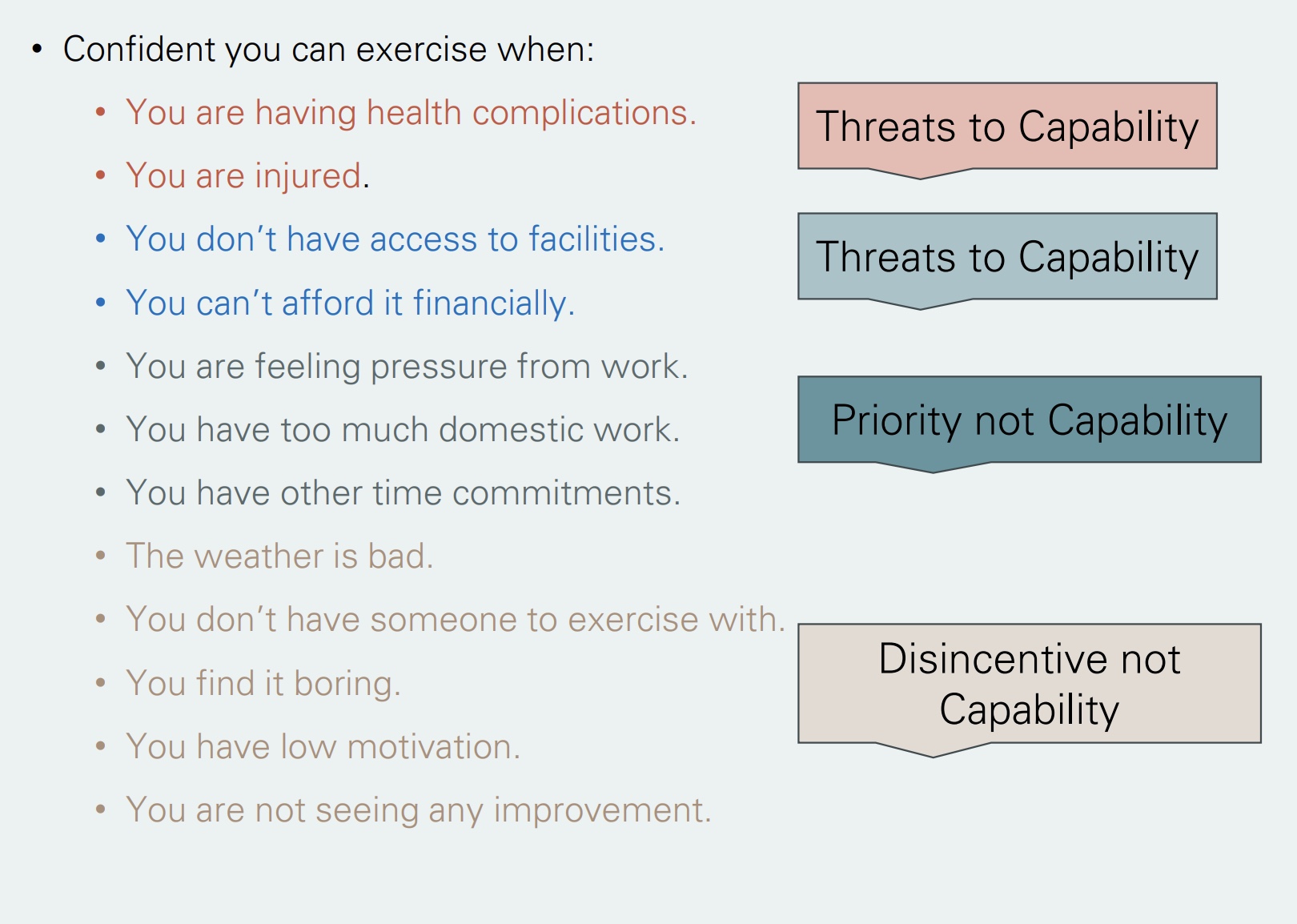
examples task vs barrier self-efficacy
-threats to capability=task efficacy
-blue=social and envionrmental
-tan=barriers
*don’t memorize examples, but be able to explain difference task and barrier self-effiacy; important to know what sources impacting efficacy
Self-efficacy and PA
-most validated and consistent correlate
-Meta-analysis of 67 studies: 60% support a significant direct relationship (*don’t memorize number, know increase confidence=increase PA)
Personal factors: outcome expectations
-engage in behavior for a reason; associated if engage in behavior or not
physical: most common, short and longer term; ex: increase muscle size, lose weight, lower BP and chronic disease
social: meet new people, w/ friends
self-evaluative: how feel about self; feel better about body, achieved someting; compare
Personal factors: knowledge
-Understanding health risks and benefits of practices and information necessary to perform behavior
-“Precondition for change” → usually insufficient alone to change (especially for long term change)
*knowing benefits but not doing behavior not enough, but “health literacy” still improtant
environmental factors (list)
*perceived or actual physical envionrment
-observational learning (*what theory based on)
-normative beliefs
-social support
-barriers and opposites
observational learning
-People learn by observing behaviors and consequences
-Influenced by characteristics of the role model and learner
*how much pay attention to it? important to me?
normative beliefs
-Perceived prevalence and social acceptability of a behavior
social acceptability may differ w/ cultures (Ex: smoking)
-Motivation to comply influenced by social consequences and self-evaluative consequences
-often overestimate undesired behaviors (ex: think more people drink than actually do)
*recently new
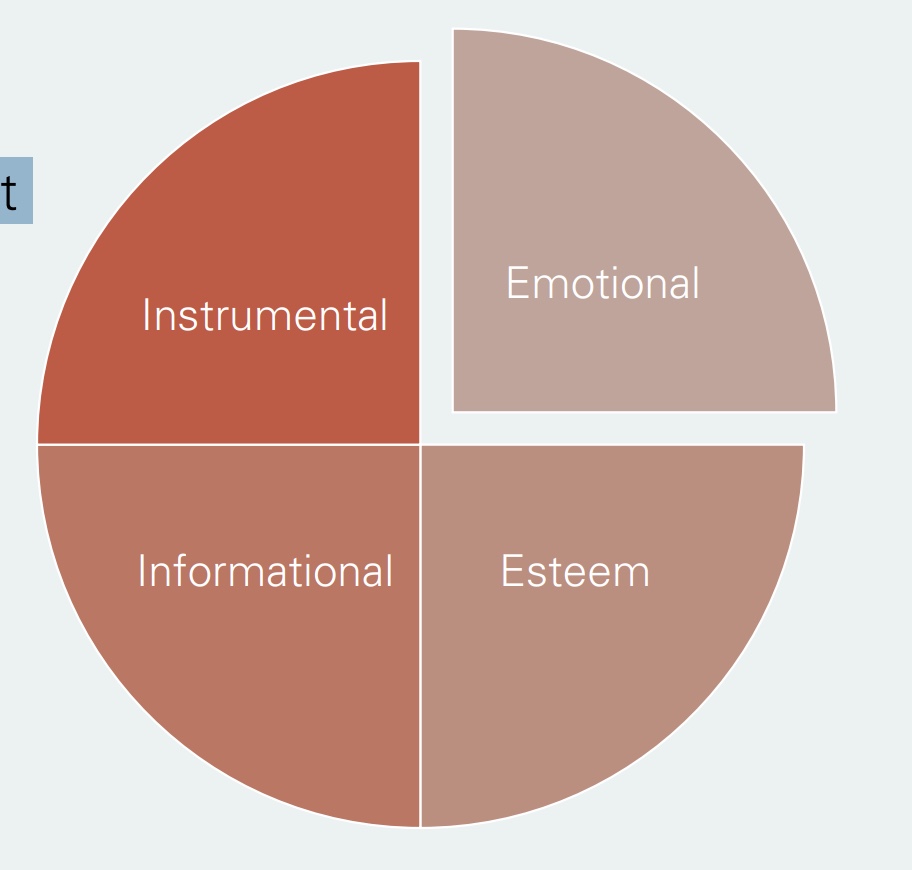
social support
-Process by which interpersonal relationships promote and protect individual’s well-being
Different Sources
-Emotional: ex=talking w/ friends
-Esteem: encouragment, validation
-Informational: lot w/ health care providers
-Instrumental: provide material or equipment necessary for behavior
^*instrumental and info used to be only 2 health are provides did, but all 4 imp
*lot of research, big driver of health; process=develop over time; dif support want to receive person to person
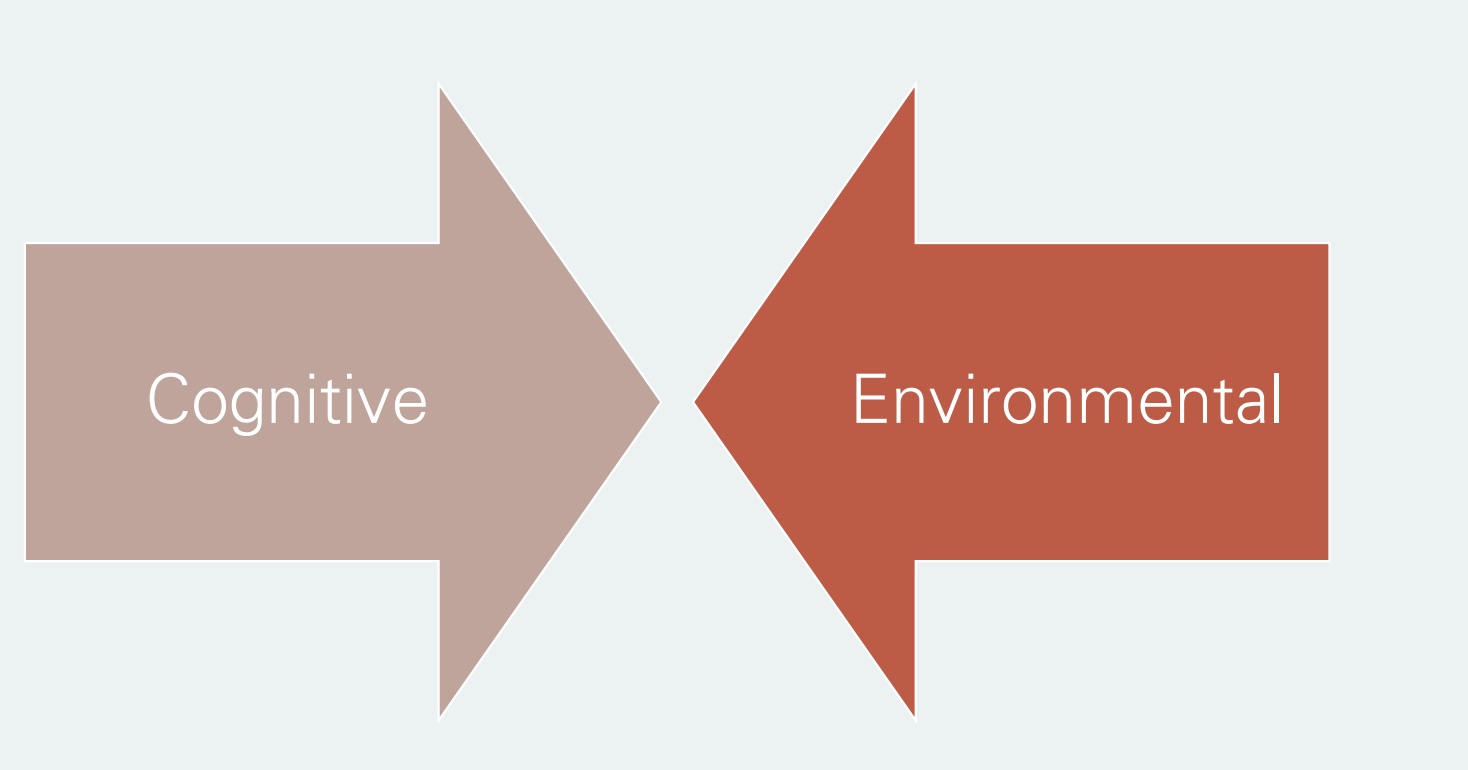
barrier and opportunties
-different and overlap; opposites of each other
Cognitive
-harder to determine, understand, and fix
-ex: low motivation, self-efficacy, fear, knwoeldge
Environmental
-what we think of more, focus in the past
-ex: weather, not safe area, no gym
Behavior components (list)
behavioral skills
*directly associated w/ behavior; studied extensively; often in intervention
-Self-monitoring: most widely applied, beneficial; tracking the behavior
-Goal Setting: lot of research; something to strive for; hand and hand w/ outcome expectation
-Feedback: provide and receive; how utilize given feedback?
-Self-reward: treat self; physical or acknowledge success to motivate to continue program
-Self-critique: critique self appropriately
intentions
-Indicator of readiness to perform behavior
-Operate through capacity for forethought (*plan for own future) and goal setting (*ex: learning)
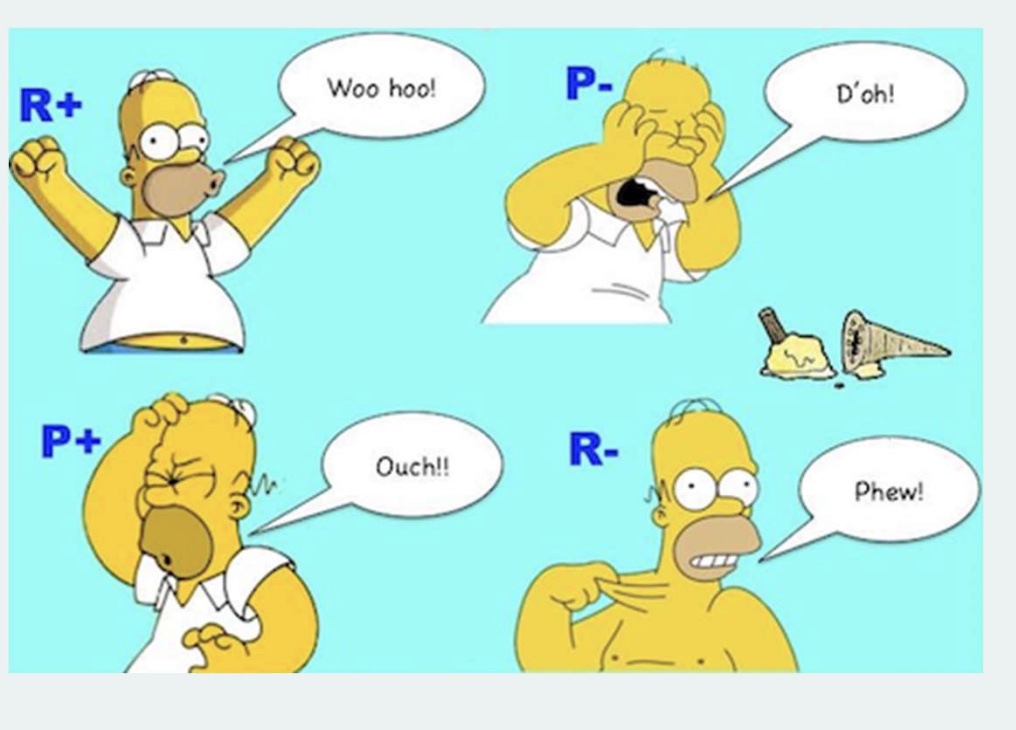
reinforcements and punishment
-2 different ways to respond; positive and negative; huge in behavior change, and debated for many years
-both to get behavior want to see; repeated cognitive awareness and understanding
Reinforcement: encourage wanted behavior
-positive: encourage by giving something; add good; ex=ice cream, “star jar”
*better for long run
-negative: take something away so continue behavior; remove bad; ex=seat belt stops once click
Punishment: stop unwanted behavior
-positive: add something on as punishment for behavior not suppose to do; add bad; ex=runs at practice
-negative: stop behavior by taking something away; remove good; ex=take phone away
What do you think comes first in terms of PA? If you were asked to develop a PA intervention, what factor would you start with in your program?
-target envionrmental, social support, or attitude?
-hard to understand where interject
interventions and SCT
-how intervene using SCT, specifically self-efficacy?
-”CATCH”=example how utilize SCT to intervence and evaluate/measure; uses theory to see how measure and see what matters; example how strategies used to change behavior, have to intervence at multiple aspects
can SCT be applied to sedentary behavior?
-not much research to say yes or no
-different than PA bc promote PA, but limit SB
-why harder to study?: are we more motivated by outcome expectations? don’t know enough about SB, and trying to limit it
-have lot evidence on screen time
underlying assumption of TPB
-underlying assumption of TPB is that intention is the best predictor of behavior
Principle of Compatibility
-need to distinguish attitude towards that of object and of behavior
*often think attitude → object is associated w/ behavior, but they differ
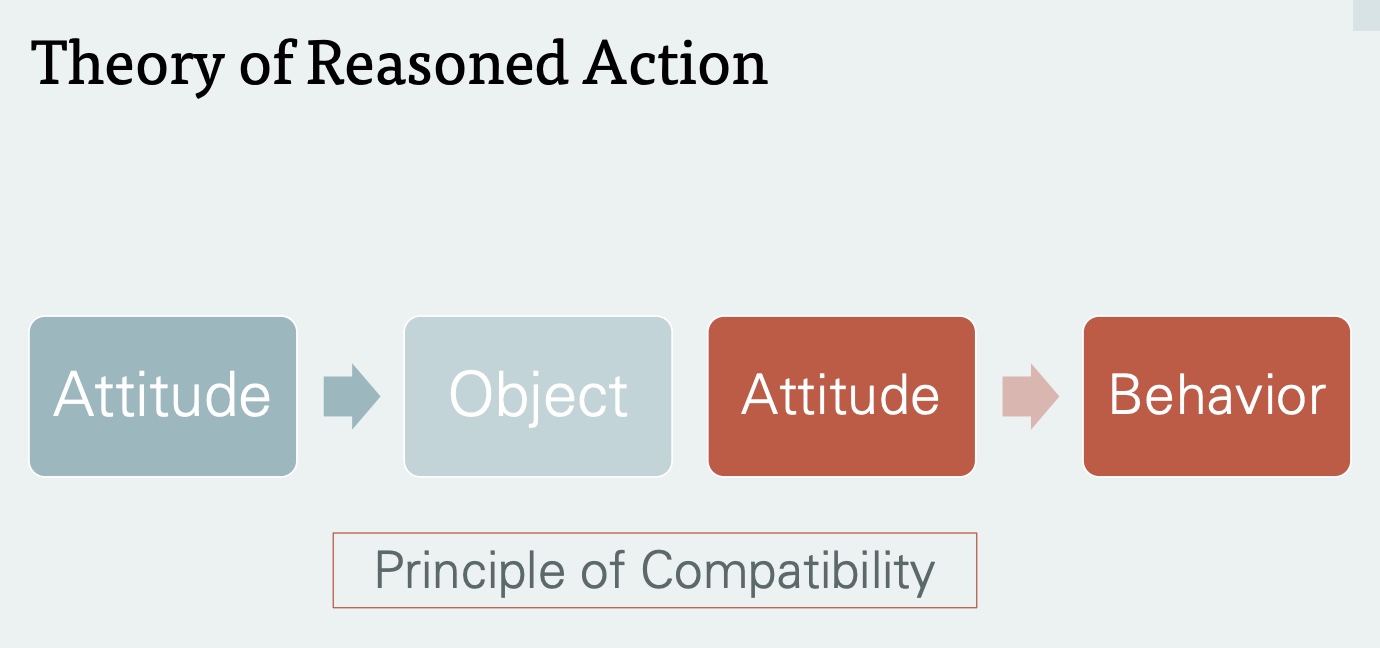
Attitude
determined by expectations or beliefs concerning attributes of the object or action, and evaluation of those attributes
*evaluation=is it important?; → “Principle of Compatability”
Expectancy-value conceptualization
-what do I expect to happen if I do a behavior, and how much do I value that?
-strong expectation + strong value= more likely do
*ex: go to class to learn, but is learning important to me?
Theory of Reason Action vs TPB
-Theory of reason action does not consider perceived control, and assumes people have volitional control over their behavior (you have autonomy); understanding of reasons why take or don’t take a certain action
-TPB accounts for factors outside of individual control
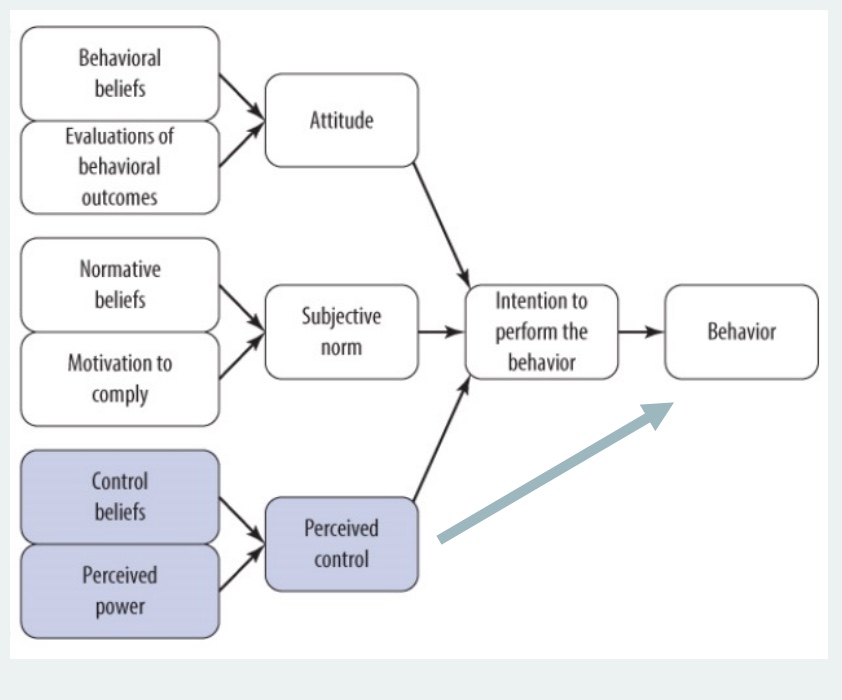
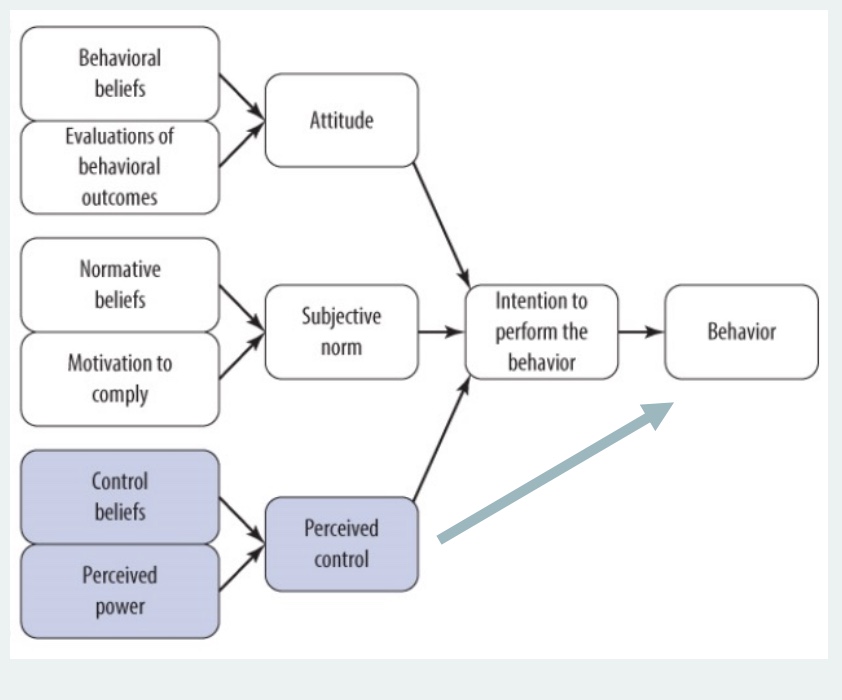
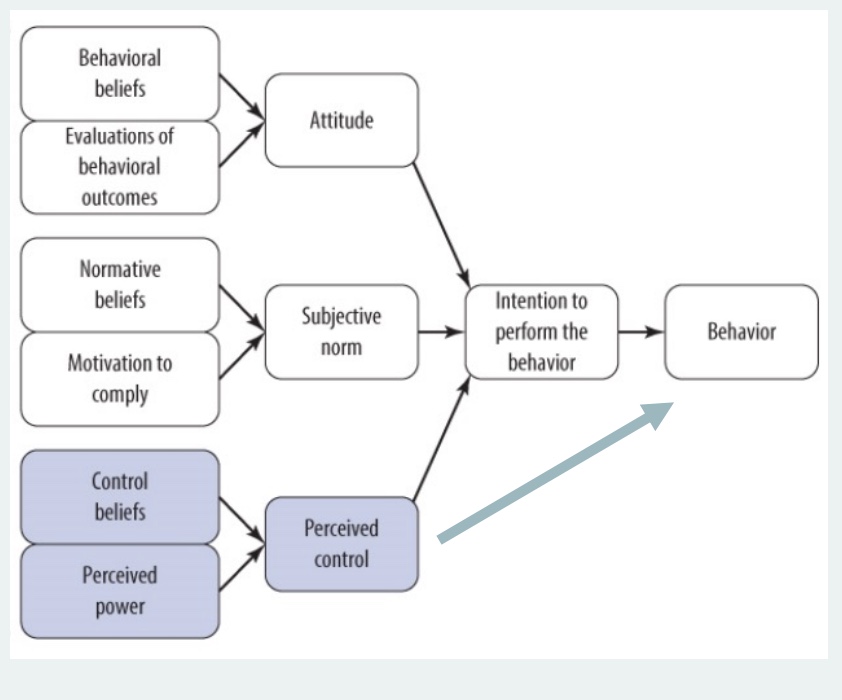
TPB (flow chart)
*can all differ based on individual
Attitude
-Behavioral beliefs: expectations if do behavior
-Evaluations of behavior outcomes: important to me?
^both=Expectancy-value conceptualization
Subjective Norms
-Normative beliefs: what do people who are important to me think what I should be doing?
-Motivation to comply
Perceived Control
*what sets TPB from Theory of Reason Action; =self=efficacy
-Control beliefs: things outside my control that effect my ability to control behavior (ex: PA and unsafe gym)
-Perceived power: how strong are these things? how much do they impede behavior?
-*has a strong, direct influence if do behavior (blue arrow)
how is TPB similar to SCT?
-Perceived control similar to SCT self-efficacy (construct SCT)
-strong, direct influence if do behavior (blue arrow)