APEX NMB Reversal Agents
1/64
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
65 Terms
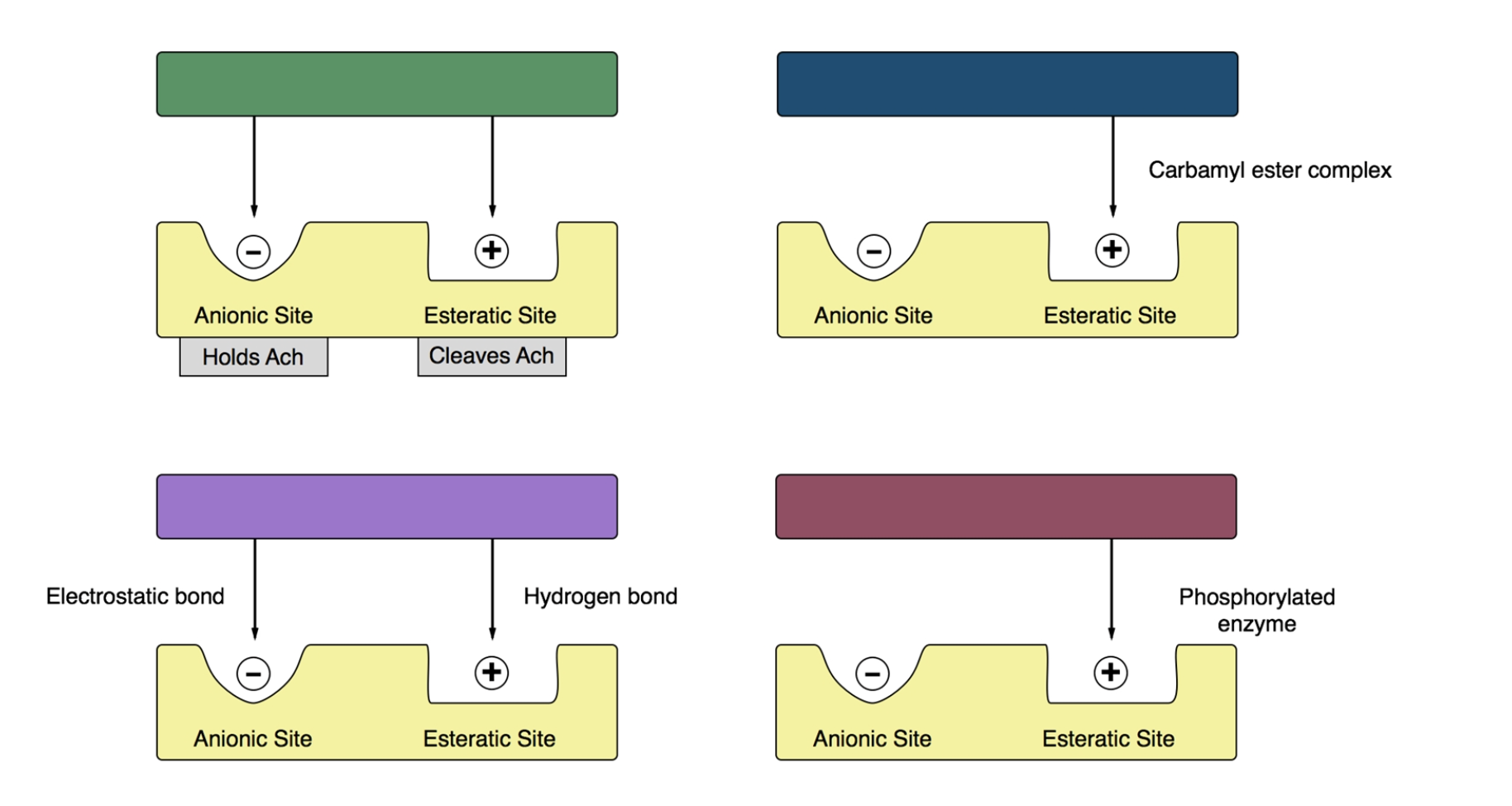
What type of bond is fromed when edrophoium binds to anionic site on acetycholinesterase
A. Electrostatic
B. Hydrogen
C. Covalent
D. Ester
A. Electrostatic
AchE terminates effect of Ach by?
Hydrolyzing into choline & acetate.
Where is the AchE enzyme located
Located around the nicotinic receptors at the NMJ
How does reversing NMB work
By giving an AChE-I at the NMJ. Since more ACH becomes available, its better able to compete for alpha binding site on nicotinic receptor and antagnoize the block.
Important to note: even though Ach concentration is inrease, NMB still needs to be eliiminated from the body
Ache-I reverses what NMBs
Edrophium,neostigmine, and pyridostigmine.
AchE-I reverse effects of NMB in what 2 ways
Enzyme inhibition
Presynaptic effects
Where does pseudocholinesterase reside
in the plasma
What does pseudocholinesterase do
metabolized succs.
inhibited by neostigmine and pyridiostime but NOT EDROPHONIUM.
Therefore if succs is given after neo or pyrdo—> DOA of succs will be prolonged
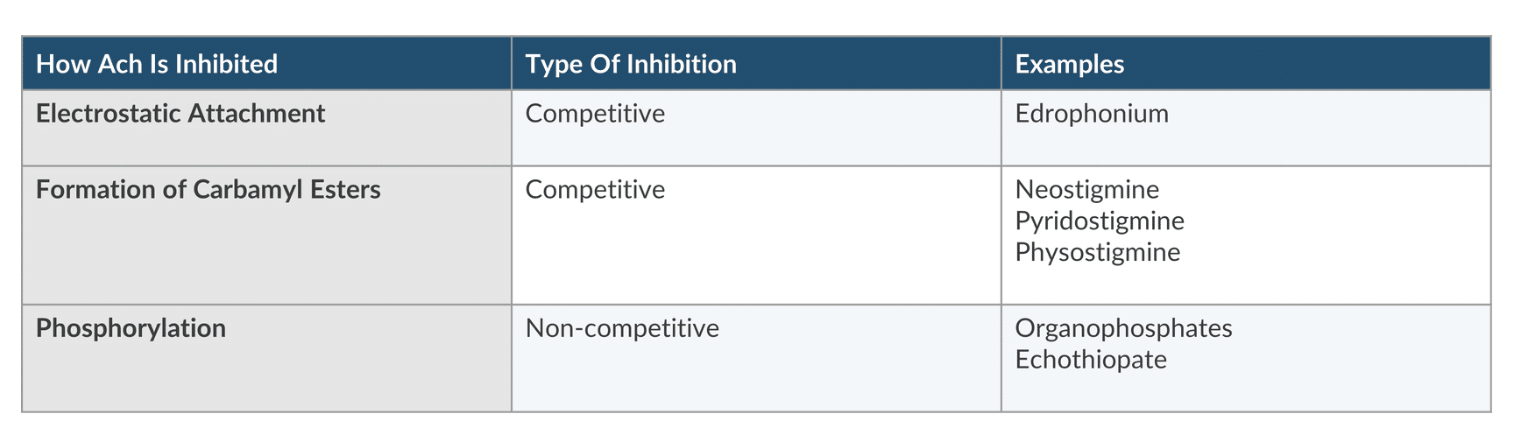
ACHE interacts with sites in 1 of three ways
electrostatic attachment, formation of caramly esters, and phosphorylation
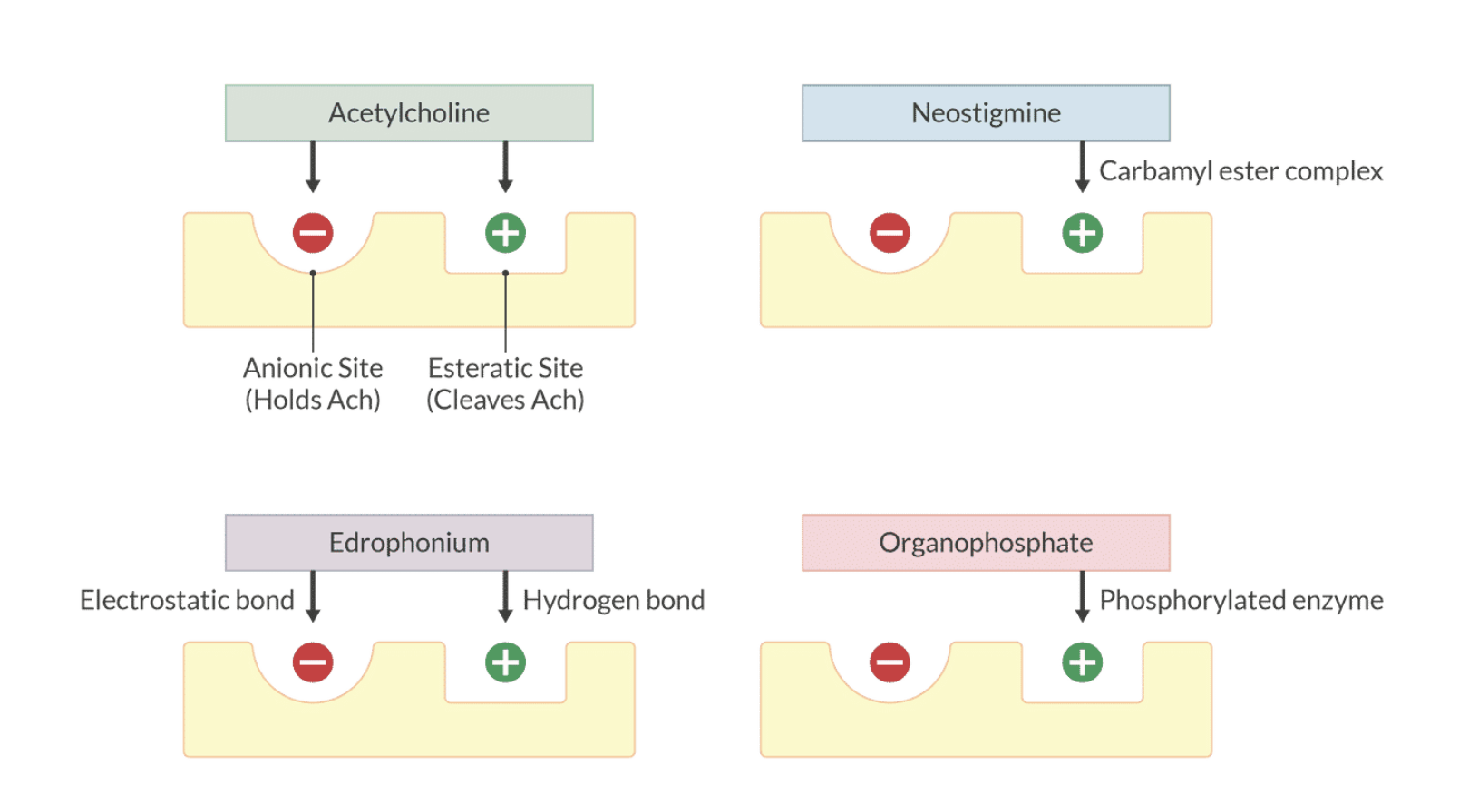
How is ACh inhibited;type of inhibition; Examples:
Electrostatic attachment
Electrostatic attachment= competitive
Ex. Edrophonium
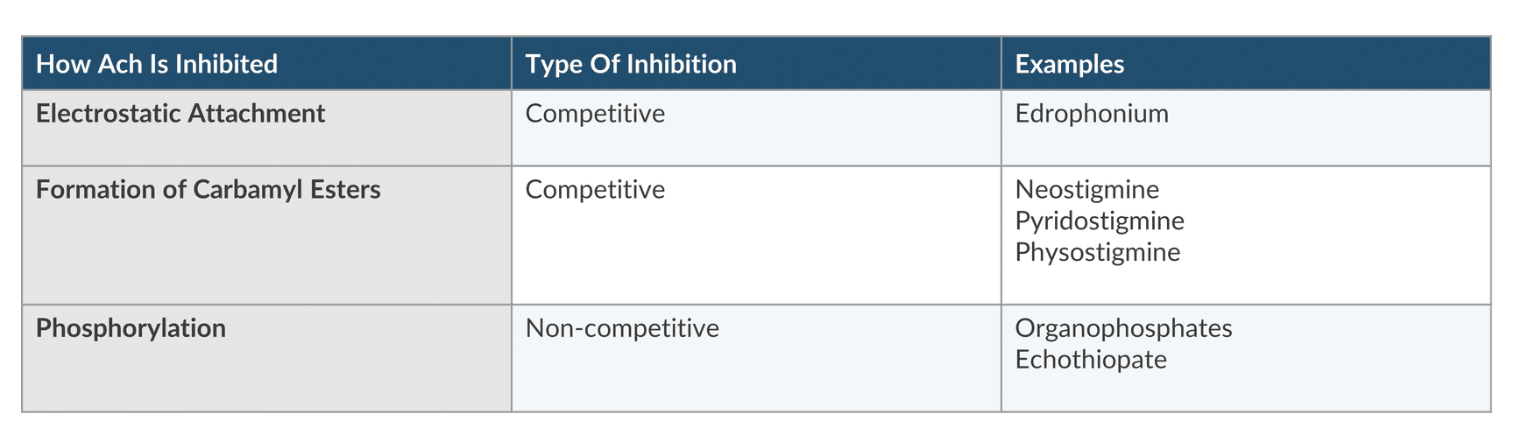
How is ACh inhibited;type of inhibition; Examples:
Formationation of carbamyl Esters
Formationation of carbamyl Esters= competitive
Ex. Neostigmine, pyridostigmine; physostigmine
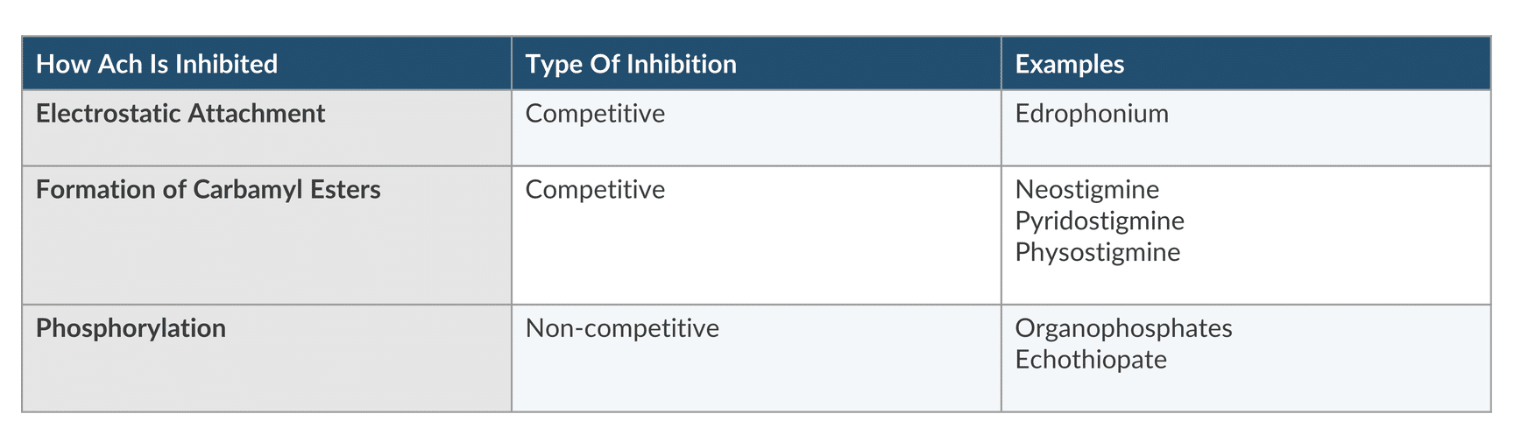
How is ACh inhibited;type of inhibition; Examples:
Phosphorylation
Phosphorylation= noncompetitive
Ex. organophosphates & echothiophate
Presynaptic site of action effects 2 mechanisms
similar to succs, AChe-I stimulate presynatpic receptors anc release more ACh
ACHE-1 near presynaptic receptor increases ACH concentration so it’s actually ACH that stimulate the receptor
— therefore MOA of edrophonium is likely presynaptic
Which statement regarding ache drugs are true 2
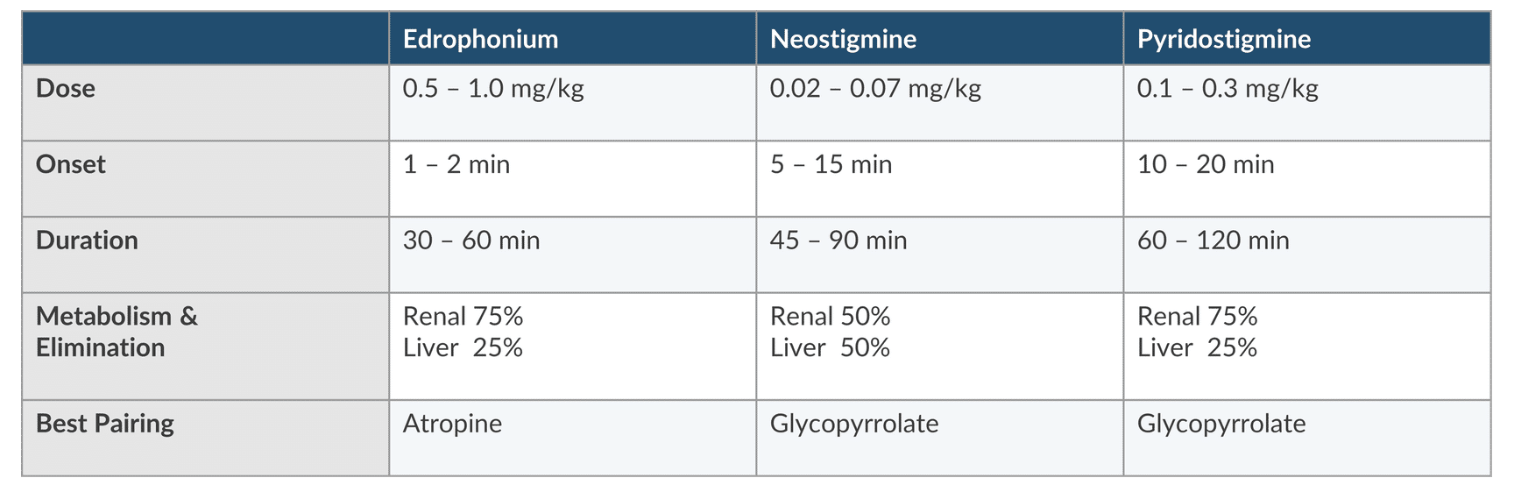
A. 50% of neostigmine is metabolized by the liver
B. Edro + neo has synergistic effects
C. Renal failure necessities second dose
D. Neostigmine is more portent than pyridostigmine
A. 50% of neostigmine is metabolized by the liver
D. Neostigmine is more portent than pyridostigmine
How do you reduce the cholinergic SE
Give anticholinergic drug with ACHE-I
Atropine is best paired with
Edrophonium
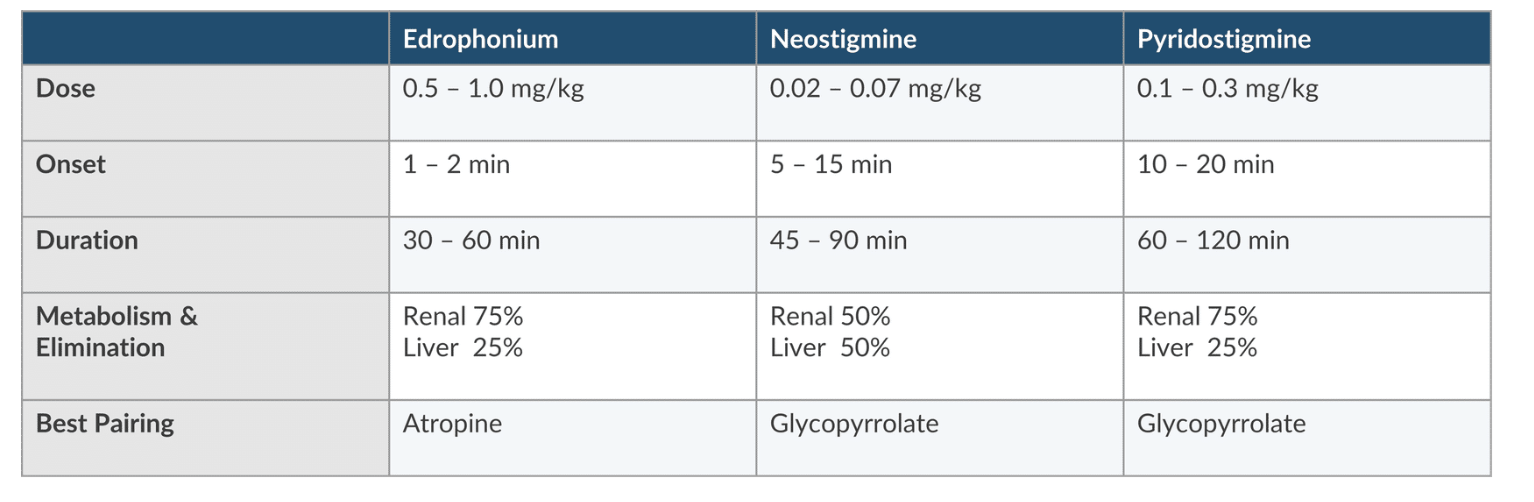
Glycopyrrolate is best paired with
Neostigmine or pyridostigmine
Do you need to renal dose NMB or ACH-I
No, renal failure prolongs DoA for both NMB and ACH-I. No need to adjust dose or re-dose it
The deeper the NMB, the
longer the onset time of the ACHE-I
ACHE-I & celiing effect
NO ceiling effect —> additional doses DO NOT produce better recovery
Which only makes SE worse
Does mixing Ach-I give synergistic effect
No
Who has a faster antagonsium with neostimgme
Faster in infants/children compared to adults
What group crosses BB
Tertiary amines (physostigmine) cross BBB
quaternary amines= Edrophonium, neostigmine, and pyridostigmine DO NOT cross BBB
What does TOF <0.9 indicate 3
Increase risk of airway obstruction, hypoxemic effects, and postop pulmonary complications
What can happen if you give excessive dose of ACH-I
can cause paradoxical weakness
Other uses of neostigmine & physiolgstimine
Intrathecal neostigmine (50-100mcg) produces analgesia. SE N/V, pruitrisits, and prolong sensory & motor block
Physostigmine (40mcg/kg) reduces post op shivery. Efficacy= meperidine and clonidine (Dex also reduces shivering)
What SE is LEAST likely to occur after neostigmine admin
A. bronchospasm
B. mydriasis
C. Nausea
D. prolong QT interval
B. mydriasis
Neostigmine causes miosis not mydriasis
Why do Cholinergic SE occur
increasing ACH concetnratin at musarinc recepor—> causes parasympathetic SE
What are the cholinergic SEs & pneumonic
DUMBBELLS
Diarrhea, Urination, Miosis, Muscle Weakness, Bradycardia, Bronchoconstriction, Emesis, Lacrimation, Salivation.
Compared to atropine, glyco is MORE likely to cause
A. Tachycardia
B. Xerostomia
C. Sedation
D. Mydriasis
B. Xerostomia
Atropine & scopalamine
naturally occurring tertiary amines
They are lipophilic (nonionized) can easily cross lipid membranes (I.e placenta, GIT, BBB—> so think CNS SE)
Glyco
quaternary ammonium derivative
Ionized
Does not cross cell membrane (placenta)
NO CNS activity
Small doses of atropine can cause
paradoxical bradycardia
due to inhibition of presynaptic M1 receptor on vagal nerve endings. M1’s jb is to reduce ACH release via negative feedback loop. Blocking Presynaptic M1 receptor turns off feedback loop and allows for continued ACH release and l/t bradycardia
Previous heart transplant vs muscarinic effects
muscarinic antagonists do not effect s/p heart transplant plts so HR is not affected.
HOWVER, they can still experience other cholinergic effects from ACHE-I so you still have to give muscarinic antagonists with ACHE-I
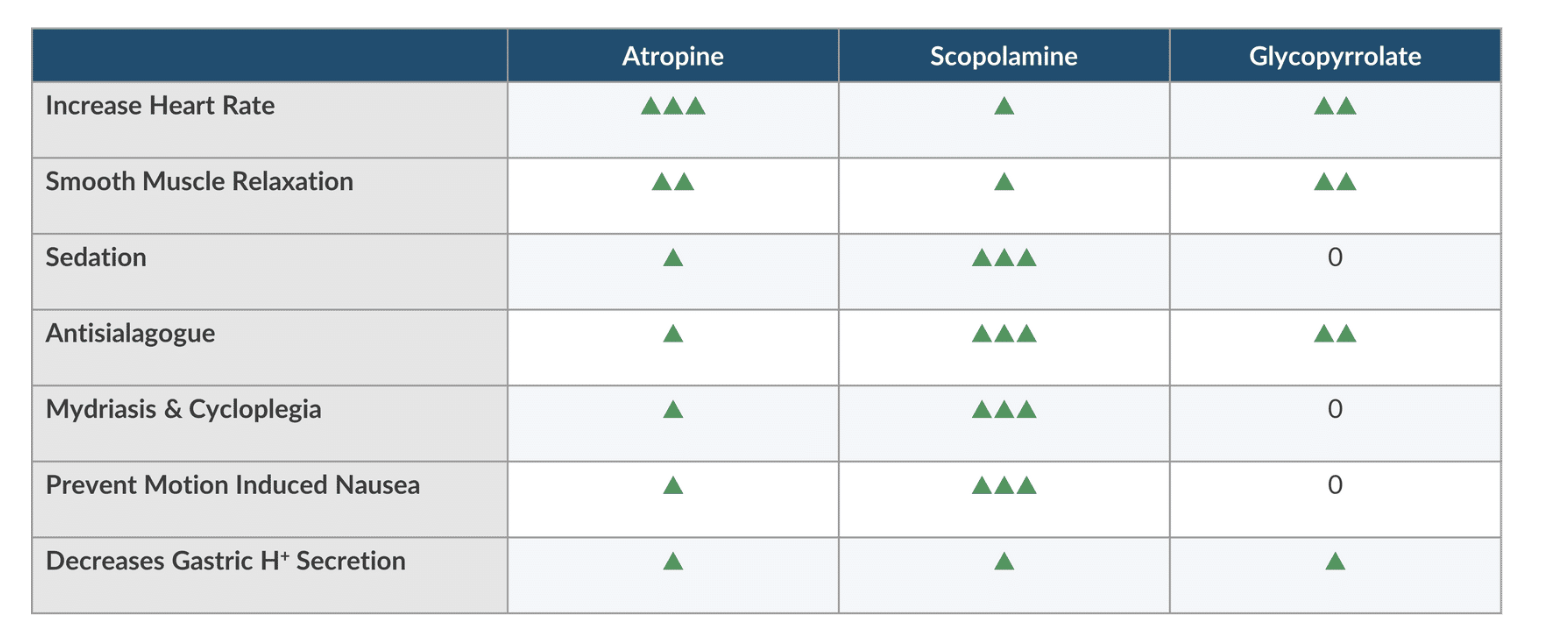
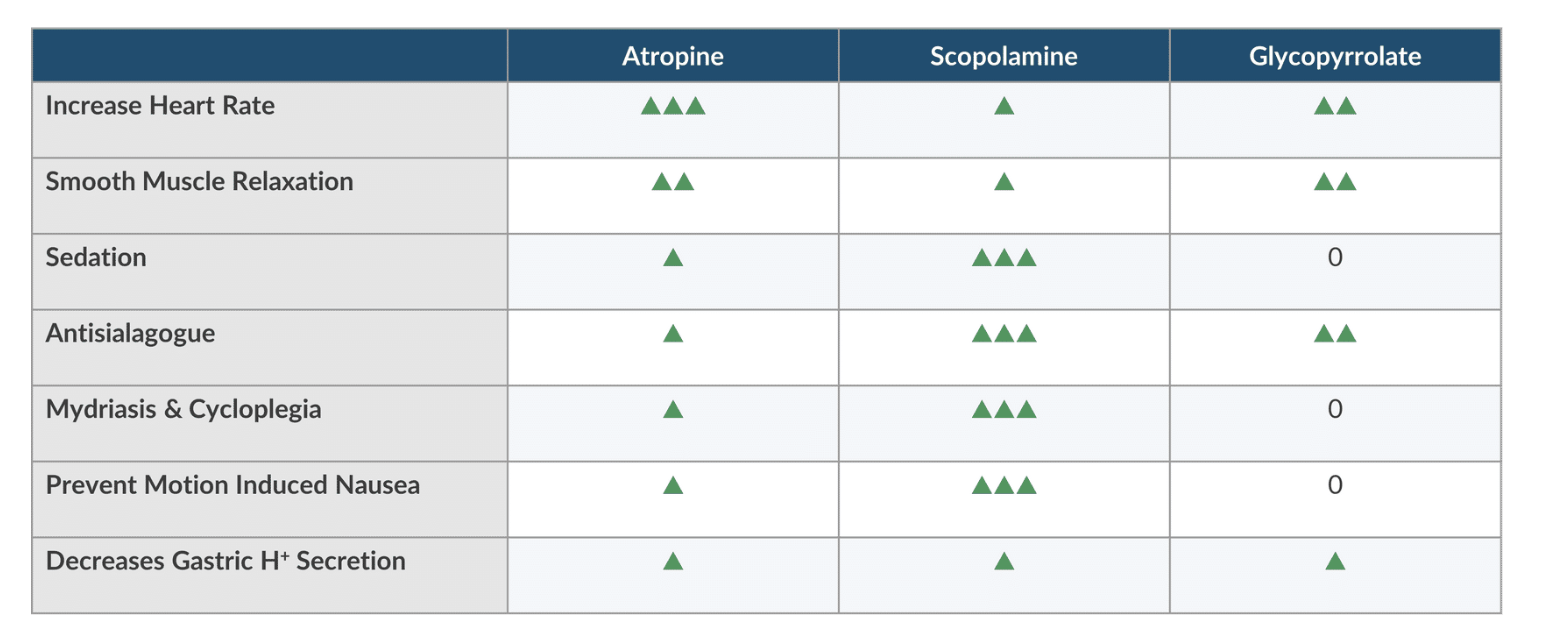
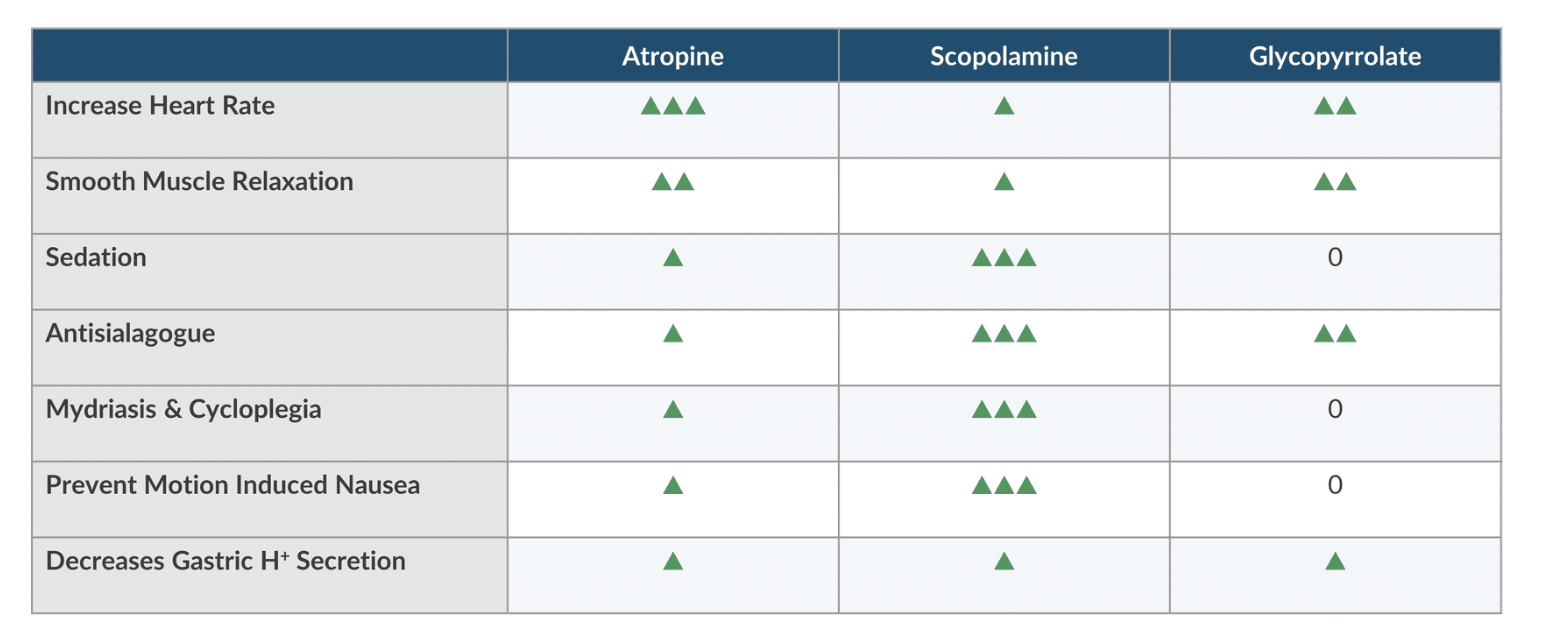
Atropine vs Scopolamine vs glycopyrrolate
Which one increases the HR the most
Atropine> glyco> Scop
Atropine vs Scopolamine vs glycopyrrolate
Which one has the most smooth muscle relaxation
Atropine & glyco> scop
Atropine vs Scopolamine vs glycopyrrolate
Which one causes the most sedative effect
Scopalamine> atropine
Glyco has not sedative effect
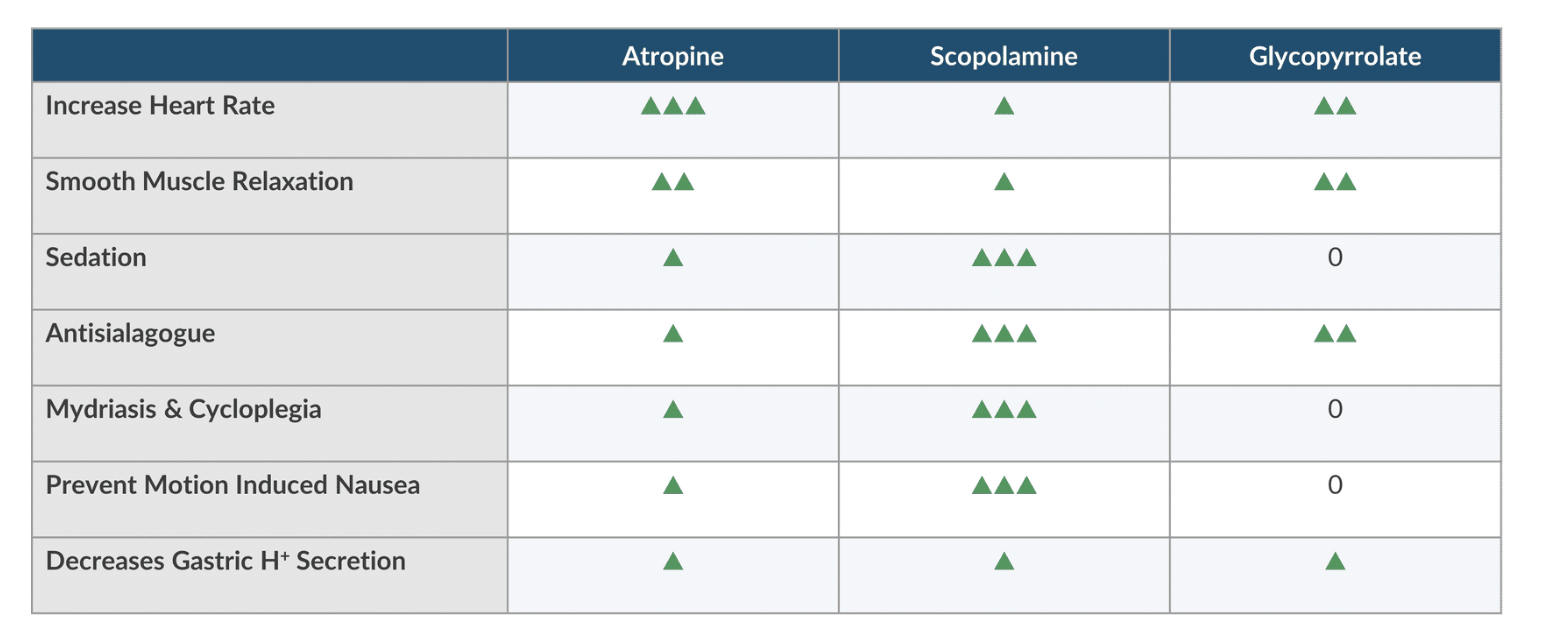
Atropine vs Scopolamine vs glycopyrrolate
Which has the most antisialoguse
Scop>glyco> atropine
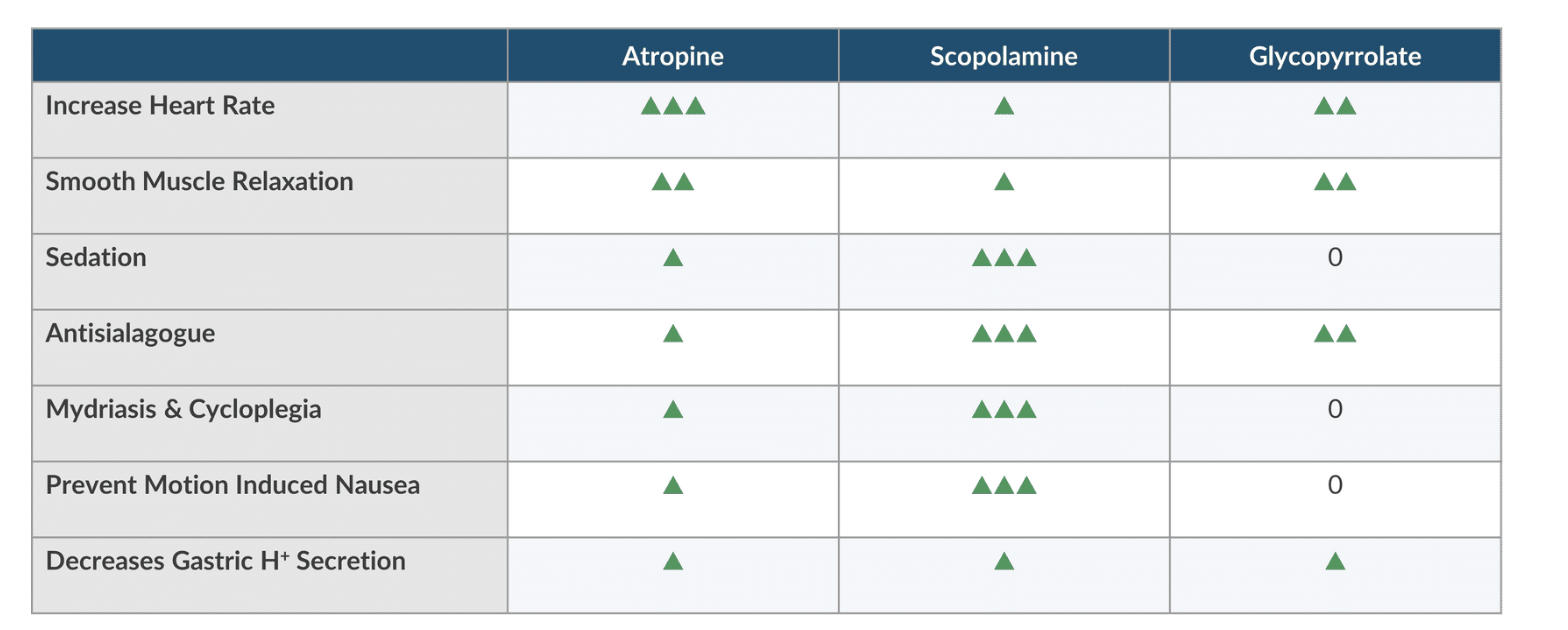
Atropine vs Scopolamine vs glycopyrrolate
Which has the most mydriasis (pupil dilation) & cycloplegia ( temporary paralysis of the ciliary muscle in the eye, which prevents the lens from adjusting for near vision)
Scop> atropine
Glyco has no affect
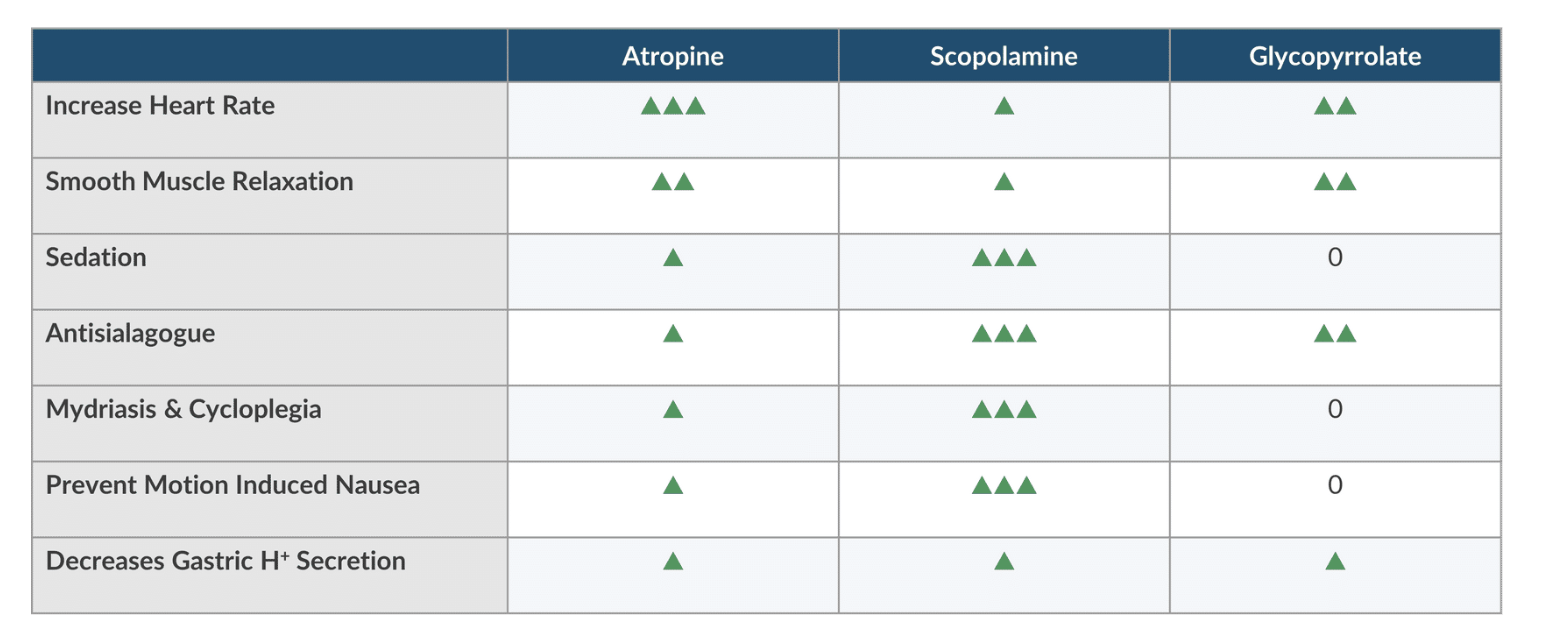
Atropine vs Scopolamine vs glycopyrrolate
What prevents the most motion induced nasuea
Scop> Atropine
Glyco has no effect
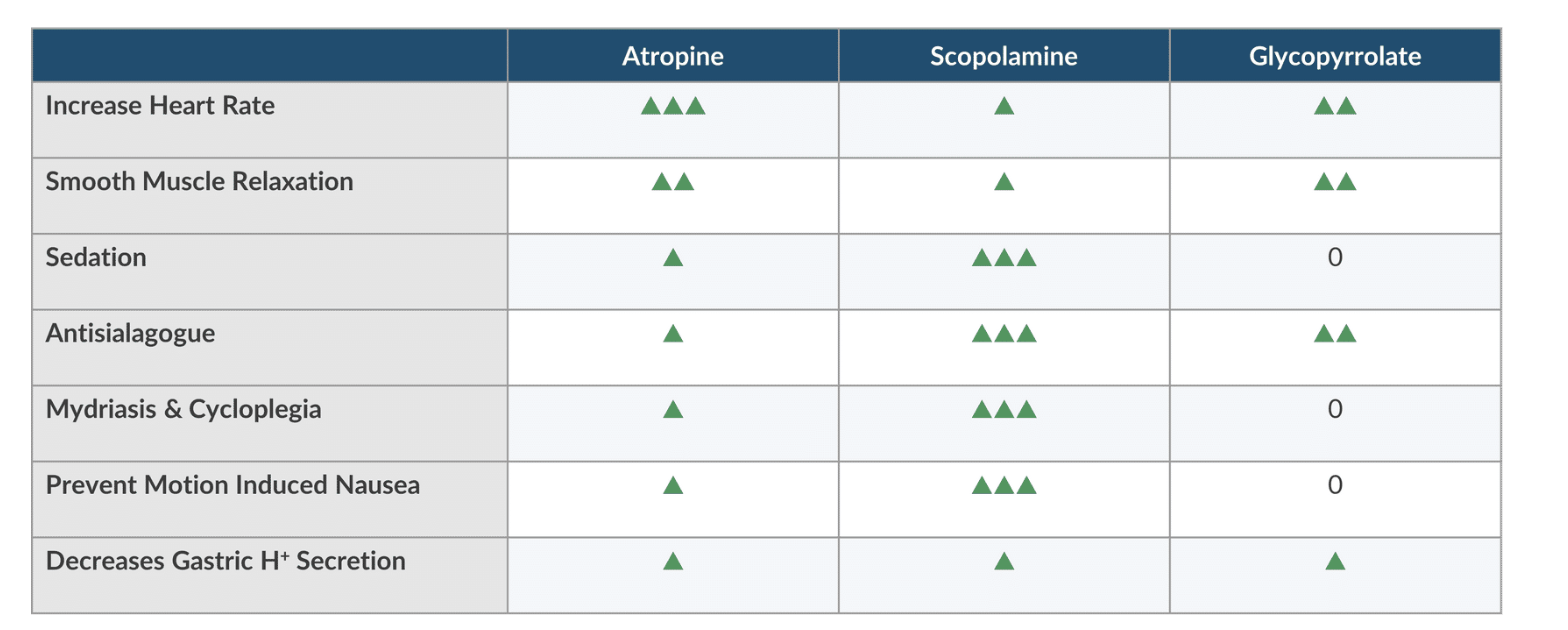
Atropine vs Scopolamine vs glycopyrrolate
What decreases Gastric H secretion the most
Trick question= they all have slight effect
Which NMB is MOST effectively antagonized by sugammadex
A. Mivacurium
B. Rocuronium
C. Cisatracurium
D. Succs
B. Rocuronium
How does sugammadex work
Selectively binds to aminosteroid ND NMB (Roc>Vec> Panc)
No effect on succs of any benzylisoquinolines (atracurium, cisatracurium, mivacurium)
Suggamadex MOA
Gamma cyclodextrin made of 8 sugars in assembled in a ring. Ring encapsulates NMB, making it inactive and unable to engage with nicotinic receptors.
Analogy= febreze for aminosteroid NMB
Encapsulating Roc reduces concentration in plasma which augments concentration gradient between NMJ and plasma therefore increasing rate of transfer of Roc to NMB toward plasma. Affinity for roc is strong but can be reversed
How is roc and sugammadex excreted
Roc= primarily excreted by biliary system
Sugammadex- roc complex excreted unchanged by the kidneys
How does sugammadex improve safety 3
Can be used for difficult intubation without drawbacks of succs
Cna reverse DENSE NMB quickly reducing risk of residula arlaysis
ALlows for dnese blockated until end of sx without delaying extubation
Dosing for sugammadex for Roc and Vec
ACTUAL BODY WEIGHT
if Roc or Vec with TOF 2 or better—> 2 mg/kg
If Roc or Vec with TOF 0 + 2 PTC or better—> 4 mg/kg
If ROC > 3min after admin at 1.2 mg/kg or less —> 16mg/kg
What if the patient needs to be paralyzed after suggamadex
Use a non-aminosteriod NMB or redose roc or vec (sometimes works)
Use non-aminosteroid NMB (Succs, atracurium, cisatracurium, mivacurium)
Can be given regardless of when sugammadex was administered
This is the only option if 16 mg/kg of sugammadex was given within 24 hours of the need for addition MR
If <4 mg/kg of sugammadex was administered→ can redose roc or vec
The patient received suggammed 5 min-4 hrs→ give Roc 1.2mg/kg
If patient receiving sugammadex> 4 hrs ago—> give rock 0.6 mg/kg or Vec 0.1mg/kg
Risks of sugammadex 3
analphyalsiz (0.3%)
bradycardia and cardiac arrest— anticholinergics useful in this context
Reduces hormonal contraception up to 7 days. so use backup method
After administering 50mg of roc to an 80 kg patient, CRNA encounters can’t intubate and can’t ventilation situation. How much sugammadex should be administered at this time
16 mg/kg x 80kg= 1280
What type of bond is formed when neostigmine binds to ache
A. covalent
B. electrostatic
C. Ester
D. Hydrogen
C. Ester
What SE is LEAST likely to occur after neostigmine administration
A. prolong QT interval
B. Miosis
C. Bronchodilation
D. Nausea
C. Bronchodilation
Compared to scopolamine, atropine is more likely to cause
A. tachycardia
B. cycloplegia
C. Xerostomia
D. sedation
A. tachycardia
What statements regarding ache drugs are true 2
A. Pyridostigmine is less potent than neostigmine
B. 90% of neostigmine is metabolized by the liver
C. Edrophonium + neostigmine have additive effect
D. Renal failure necessitates larger dose
A. Pyridostigmine is less potent than neostigmine
C. Edrophonium + neostigmine have additive effect
Rank the following drugs acording to tendency to cause cycloplegia
Scop, glyco, atropine
Scop +++
Atropine ++
Glyco 0
The following are well absorbed from GIT EXCEPT
A. Scop
B. Glyco
C. Physostigmine
D. Atropine
B. Glyco
Atropine & scop are naturally occuring; Phys is lipid soluble; Glyco does not cross any membranes
Match ache-I to dose
Pyridostigmine
Neostigmine
Edrophonium
Pyridostigmine= 0.3 mg/kg
Neostigmine= 0.05 mg/kg
Edrophonium= 1 mg/kg
What ache-I prolong duration of succs 2
A. phys
B. Edrop
C. Pyridio
D. Neo
C. Pyridio
D. Neo
Match the drug to onset of action. Assume steady state of NDNMB in plasma
Neostigmine
Edrophonium
Pyridostigmine
Edrophonium= 1 min
Neostigmine= 10 min
Pyridostigmine= 15 min
Select the best statement regarding anticholinergic agent and edrophonium when used as NMB
A. Glyco should be mixed in the same syringe as edrophonium
B. Atropine pairs better than glyco
C. Atropine is given after edrophonium
D. Atropine should be avoided due to CNS SE
B. Atropine pairs better than glyco
In PACU, 85 female received scopolamine is now confused and agitated. What is the best intervention at this time.
A. Physostigmine
B. Pyridostigmine
C. Reduce environmental stimuli
D. Midazolam
A. Physostigmine
Phys crosses BBB
Sugammadex antagonized NDMR by encapsulating
A. Roc only
B. Benzyliquinoones and aminosteroids
C. Benzylisoquinolines
D. Aminosteroids
D. Aminosteroids
Select the best ACHe-I to antagonize 90% twitch suppression
A. Pyridostigmine
B. Physostigmine
C. Edrophonium
D. Neostigmine
D. Neostigmine
Phys has prolonged onset
Edro is effective in reversing mild to mod NMB but cannot reverse profound relaxation (90% twitch depression or one twitch)
Neostigmine antagonized Roc by
A. potentiating ache activity
B. reversibly binding to butyrylcholinesterase
C. Decreases ach hydrolysis
D. competing with roc at nicotinic receptor
C. Decreases ach hydrolysis
Click on the box that represents neostigmine
navy blue