immune, hematologic, and neoplastic disorders
1/91
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
92 Terms
immune and allergic disorders:
conditions affecting body's defense mechanisms and hypersensitivity responses
- HIV
- allergy
-allergy anaphylaxis
The nurse is caring for a pt w/ HIV and is providing edu about antiretroviral meds. What should be included in the teaching plan?
the meds can be used for pre-exposure prophylaxis for HIV
3 multiple choice options
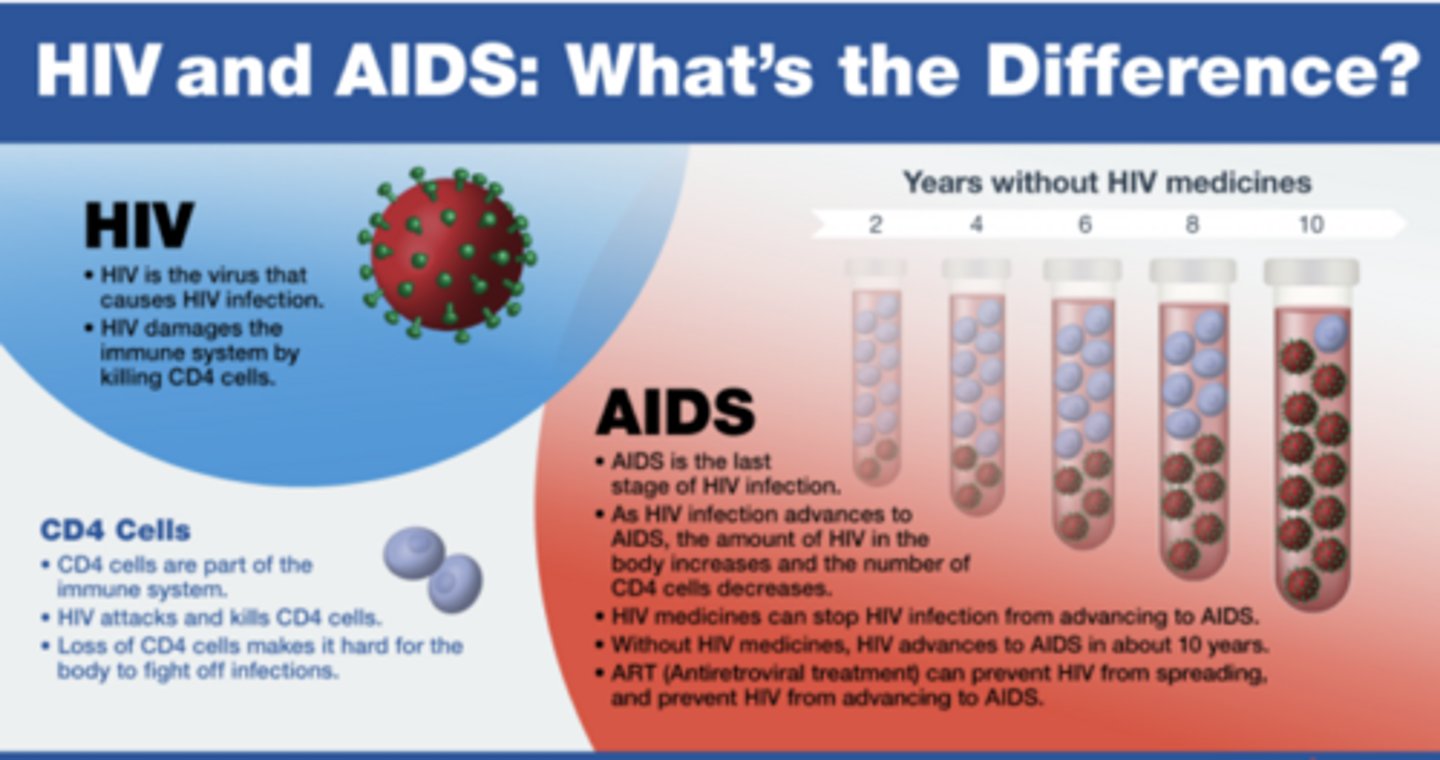
HIV vs. AID's
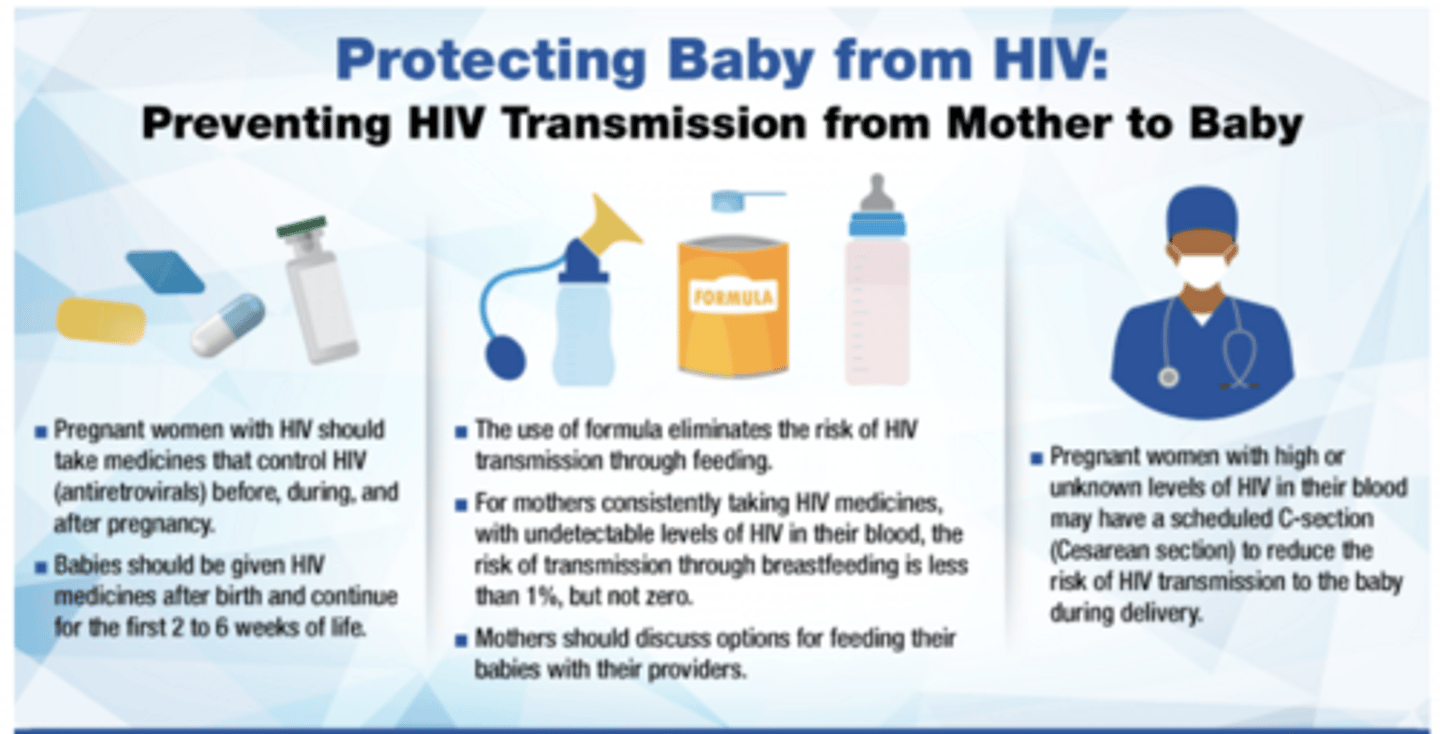
preventing HIV transmission from mother to baby
pediatric HIV/ AIDS
virus attacks CD4 and T lymphocytes = immunodeficiency
pediatric HIV/ AIDS: clinical symptoms
- retrovirus targeting CD4 & t cells, leading to immune suppression
- fail. to thrive, chronic diarrhea, opportunistic infections
pediatric HIV/ AIDS: nursing assessment
- hx of maternal HIV/ risk factors, growth and development (watch for delays/ stagnation)
- frequent/ severe infections
- nutritional status
pediatric HIV/ AIDS: testing
- PCR testing (infants)
- Elisa/ western blot (older children)
- CD4 count and viral load mo nonitoring
pediatric HIV/ AIDS: nursing interventions
- assess growth, dev. milestones, infection signs
- promote adherence to ART
- prevent infection: hand hygiene, immunizations, safe feeding
- support coping and confidentiality
meds:
- antiretroviral therapy (ART): combo of NRTI's, NNRTI's, and protease inhibitors
antiretroviral tx
- when teaching clients about ART, emphasize:
- adherence is critical to prevent viral resistance
- ART DOES NOT CURE HIV, but allows people to live longer healthier lives
- PrEP and PEP use similar meds for prevention in HIV-negative individuals
- PrEP
- prevents HIV infection before exposure
- taken daily on a long term basis for ongoing risk
- PEP
- prevents HIV infection after a possible exposure
- MUST BE started w/ in 72 hrs of exposure
PrEP
- prevents HIV infection before exposure
- taken daily on a long term basis for ongoing risk
PEP
- prevents HIV infection after a possible exposure
- MUST BE started w/ in 72 hrs of exposure
allergy and anaphylaxis: clinical symptoms
- rash
- sneezing
- watery eyes
- wheezing
- asthma exacerbations
- urticaria
-hypotn
- angioedema
allergy and anaphylaxis: nursing assessment
- exposure hx
- skin and respiratory symptoms
allergy and anaphylaxis: testing
- skin testing
- serum IgE level
- elimination diets
allergy and anaphylaxis: nursing interventions
- identify and avoid triggers
- rapid assessment of ABC's (presence of urticaria, angioedema, resp. distress, shock)
- emergency management of airway
- teach proper use of epi pens
- edu parents on allergen labels, emergency plans
meds:
- antihistamines, corticosteroids, leukotriene modifiers, epi auto injectors
allergy anaphylaxis: pathophysiology
severe, systemic hypersensitivity → massive histamine release → vasodilation, airway edema → bronchospasm
allergy anaphylaxis: clinical manifestations
- sudden hypotension
- urticaria
- wheezing
- laryngeal edema
allergy anaphylaxis: dx
clinical dx (no time for labs)
allergy anaphylaxis: meds
- IM epi (first-line)
- antihistamines, corticosteroids, bronchodilators
allergy anaphylaxis: nursing interventions
- immediate admin of epi
- airway management, O2, IV fluids
epinephrine auto injector: generic name
epinephrine (epi pens)
epinephrine: primary eff/ MOA
- stimulates a and b adrenergic receptors
- vasoconstriction, bronchodilation, ↑HR, ↓mucosal edema
hematologic disorders
conditions r/t the blood and blood forming tissues (excluding primary malignancies)
ex.
- iron deficiency anemia
- sickle cell anemia
- hemophilia
- lead poisoning
iron deficiency anemia (IDA)
decreased iron intake, absorption, or loss → reduce hemoglobin synthesis
iron deficiency anemia: clinical symptoms
- pallor
- fatigue
- tachycardia
- koilonychia "spoon nails"
- poor feeding
- pica
- developmental delay
iron deficiency anemia: nursing assessment
- dietary hx
- assess energy level
- growth and dev.
- signs of pallor or fatigue
- vital signs (tachycardia, SOB, breathlessness)
iron deficiency anemia: testing
- CBC: red cell indices- low hgb & hct, low mean corpuscular vol (mcv)(microcytic anemia)
- low serum ferritin (primary indicator of iron stores)
- screening @ 12m, repeat between ages 1-5yr for pt at risk
iron deficiency anemia: nursing interventions
medications
oral ferrous sulfate or other iron supplements
- give iron with vitamin C; avoid milk around dosing
- give through straws, brush after (stains teeth)
- edu parents on iron rich foods
- monitor for constipation or GI upset
s/s of iron deficiency anemia in children
- fatigue
- cold hands or feet
- slowed growth or development
- poor appetite
- usual craving for non nutritive substances (ex. dirt, starch, ice, etc.)
- abnorm. rapid breathing
- behavioral problems
sickle cell anemia
autosomal recessive; HbS (hemoglobin S) → sickling → vaso- occlusion, ischemia, hemolysis
sickle cell anemia: clinical symptoms
- pain crisis
- anemia
- acute chest syndrome (ACS)
- splenic sequestration dactylitis (rapid blood trapping in spleen → causing severe anemia and hand and feet are swollen due to vaso occlusion
- splenomegaly
- stroke risk
- delayed growth
sickle cell anemia: nursing assessment
- pain episodes
- family hx
- growth delays
- physical exam
sickle cell anemia: testing
- hemoglobin electrophoresis
- sickledex
- CBC (low hgb/ hct), high reticulocyte count
sickle cell anemia: nursing interventions
- pain controls
- hydration
- respiratory status (watch for ACS)
- spleen precautions
- educate on avoiding triggers (cold, dehydration, stress)
- infection prevention
- psychosocial support
- blood transfusion management
H: hydrate
O: oxygen
P: pain meds
S: support
meds
- hydroxyurea
- pain management
- flic acid
hemophilia
X linked recessive deficiency of factor VIII (A) or IX (B)
hemophilia: clinical symptoms
- spontaneous bleeding/ prolonged bleeding
- hemarthrosis (bleeding into joints)
- bruising/ hematomas
hemophilia: nursing assessment
- hx of bleeding
- hemarthrosis
- neurological assessment (for intracranial hemorrhage)
hemophilia: testing
- coagulation studies
- factor assays
hemophilia: nursing interventions
- bleeding prevention
- RICE for hemarthrosis
- avoid aspirin/ NSAID's
- safe environment/ activity promotion
- educate on factor administration
meds
- replacement therapy
- DDAVP (desmopressin)
- aminocaproic acid (amicar)
- cryoprecipitate
8 steps of blood transfusion
1. verification
2. inspection of unit
3. pt identification
4. baseline vitals
5. administration
6. monitoring
7. duration
8. post transfusion
blood transfusion: verification
two nurses verify → correct pt, blood type, Rh factor, expiration date, unit #, consent
prevents fatal transfusion errors
blood transfusion: inspection of unit
check for discoloration, clots, bubbles, or leaks
ensures product integrity
blood transfusion: pt identification
confirm name, DOB, MRN w/ wristband and unit label
correct pt verification per protocol
blood transfusion: baseline vitals
record immediately before transfusions
detects changes indicating a reaction
blood transfusion: administration
start infusion SLOWLY (≤2mL/min) for first 15 min, remain w/ pt
early detection for a reaction
blood transfusion: monitoring
reassess vitals every 15 minutes, then every 30, then at completion
tracks for fluid retention or fluid overload
blood transfusion: duration
complete transfusion w/ in 4 hrs MAX
prevents bacterial growth
blood transfusion: post transfusion
flush line with Ns; document total volume and patient response
ensure complete delivery and accurate record keeping
lead poisoning (plumbism)
toxic accumulations of lead in the body, particularly in bones, teeth, and soft tissues affecting multiple organ systems
lead poisoning (plumbism): clinical symptoms
- neuro status, seizures, encephalopathy, coma
- vomiting, weight loss
- anemia
- bone pain, delayed growth, skeletal deformities
- developmental delay, poor attention,, learning deficits
lead poisoning (plumbism): nursing assessment
- health hx
- physical assessment
- environmental assessment
lead poisoning (plumbism): testing
- blood lead level (BLL): primary screening test\
- serum iron ferritin
- abdominal x ray
- neuro developmental screening
lead poisoning (plumbism): nursing interventions
- assessment and monitoring
- regular BLL screening for at-risk children
- monitor growth, neuro status, and learning milestones
- environmental control
- nutrition support
- encourage food high in iron, calcium, vit C
- medication administration
- chelating agents
- family edu
- teaching parents about lead sources and prevention
early signs of lead poisoning: neuro
- irritability
- lethargy
- headache
- learning difficulties
- behavior changes
early signs of lead poisoning: GI
- anorexia
- nausea
- vomiting
- abdominal pain
- constipation
early signs of lead poisoning: hematologic
mild anemia (inhibited heme synthesis)
early signs of lead poisoning: renal
- proteinuria
- impaired renal function
early signs of lead poisoning: musculoskeletal
- bone pain
- delayed growth
early signs of lead poisoning: developmental
- speech delay
- poor attention
- learning deficits
late/severe signs of lead poisoning: neuro
- seizures
- encephalopathy
- coma
late/severe signs of lead poisoning: GI
- weight loss
- colic
late/severe signs of lead poisoning: hematologic
severe anemia
late/severe signs of lead poisoning: renal
chronic nephropathy
late/severe signs of lead poisoning: musculoskeletal
skeletal deformities
late/severe signs of lead poisoning: developmental
- cognitive impairment, decreased IQ
chelation therapy
MOA
- binds to lead to enhance urinary excretion
indications
- if BLL is ≥45
nursing consideration
- monitor renal and hepatic function; ensure hydration
succimer (DMSA)
MOA
- oral chelating agent
indications
- mild-moderate poisoning (BLL 45- 69)
nursing considerations
- oral; monitor for neutropenia, GI upset
chelation therapy: supportive therapies
indications
- iron, calcium, and vitamin C supplements
nursing considerations
- reduce lead absorption and enhance secretion
neoplastic/ oncology disorders: pathophysiology
uncontrolled cell growth in various tissues
neoplastic/ oncology disorders: assessment
- fatigue
- weight loss
- unexplained bruising
neoplastic/ oncology disorders: clinical man.
varies by cancer type
neoplastic/ oncology disorders: meds
- chemotherapy
- targeted therapy
neoplastic/ oncology disorders: nursing interventions
- supportive care
- monitor for side effects
- family edu
childhood cancers
often arise from embryonal or blood forming tissues; tend to be rapidly proliferating
childhood cancers: symptoms
varies by cancer type
- fatigue
- weight loss
- unexplained bruising
- unexplained lumps/ swelling
- persistent pain
- unexplained fever
- pallor (anemia)
childhood cancers: testing
- CBC w/ differential
- lumbar puncture (checks CNS involvement)
- biopsy-definitive diagnosis
- CT, MRI, PET scans
childhood cancers: nursing interventions
- supportive care
- pain management
- monitor for side effects
- family edu
meds
- chemo (multi-phase), corticosteroids, antibiotics, antiemetics
- radiation
- surgery
acute lymphoblastic leukemia
malignant proliferation of lymphoblasts
acute lymphoblastic leukemia: clinical symptoms
- fever, pallor, bleeding
- bone pain
- anemia, thrombocytopenia, hepatosplenomegaly
acute lymphoblastic leukemia: nursing assessment
- pale skin
- petechiae
- ecchymosis
- lethargy
- signs of malnutrition
- s/s of infection
- enlarged lymph nodes
- hepatosplenomegaly
- bone tenderness/ joint swelling or pain
- headaches
- CNS involvement
acute lymphoblastic leukemia: testing
- CBC, bone marrow biopsy
acute lymphoblastic leukemia: nursing interventions
- meds
- chemo (multi-phase), corticosteroids, antibiotics, antiemetics
- monitor for infection, bleeding, mucostitis
- manage chemo side effects
- support nutritional and emotional needs
neuroblastoma
patho/ clinical manifestations
- tumor of SNS; often adrenal origin
- S/S: firm, irregular abdominal mass, crosses midline
dx
- urinary catecholamines
- imaging
- biopsy
nursing focus
- support surgery/ chemo
- monitor for mets
- poor prognosis → family support is crucial
Wilms tumor (nephroblastoma)
patho/ clinical manifestations
- renal tumor; peak 2-5 yrs
- S/S: painless abdominal mass, hematuria
dx
- ultrasound, CT, biopsy (AFTER SURGERY)
nursing focus
- DO NOT PALPATE ABDOMEN
- prep for nephrectomy
- monitor renal function
- protect remaining kidney post op
ewings sarcoma
patho/ clinical manifestations
- bone tumor (pelvis, long bones)
- S/S: pain, swelling, fever
dx
- bone biopsy, MRI
nursing focus
- pain management
- limb protection
- support during chemo/ radiation
- physical therapy!!
rhabdomyosarcoma
patho/ clinical manifestations
- soft tissue sarcoma (head, neck, GI tract)
dx
- biopsy, imaging
nursing focus
- post op care
- airway support (if head and neck)
- fam teaching
child receiving chemo
pathophysiology
- cytotoxic effects on rapidly dividing cells
clinical manifestations
- nausea, fatigue, neutropenia
nursing assessment
- side effects
- nutritional status
- infection signs
dx
- CBC, liver/ kidney, function tests
meds
- antiemetics, growth factors
nursing interventions
- infection prevention
- manage side effects
- emotional support
radiation therapy in children
pathophysiology
- ionizing radiation changes DNA of cancer cells
clinical manifestations
- skin changes
- fatigue
- site specific effects
nursing assessment
- skin integrity, fatigue, localized symptoms
dx
- imaging for planning
meds
- symptom management
nursing interventions
- skin care
- fatigue management
- emotional support
pediatric cancer strategies: preoperative
- assess baseline VS, labs (CBC, coagulation, electrolytes), nutrition
- screen for infection or neutropenia (delay surgery if febrile)
- age-appropriate edu and emotional support
- verify informed consent and child assent
- maintain NPO as ordered
pediatric cancer strategies: intraoperative
- verify correct sit/ procedure ("timeout")
- maintain strict asepsis
- monitor VS, oxygenation, and fluid balance
- assist anesthesia and maintain airway
pediatric cancer strategies: postoperative
- monitor VS, pain, incisions, drains, and output
- maintain IV fluids, nutrition, and sterile wound care
- watch for infection, bleeding, poor healing
- provide pt management and family support
- educate on home care and follow up