Dermatology 6
1/12
Earn XP
Description and Tags
may 27th
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
13 Terms
Define MACULES and PATCHES and list the names of 10 diseases that appear with these lesions.
MACULE: flat lesion<1cm in diameter, differs in color from the surrounding skin
PATCH: flat lesion >1cm in diameter, like a larger macule
Neufibromatosis type 1 - café-au-lait spots
Junctional nevus
Blue nevus
Freckles
Melasma
Melanoma
Erythrasma
Erythrosis
Angioma piano
Solar lentigo
Define Sclerosis and list the names of 3 diseases that appear with this lesion
Sclerosis is an induration of the skin and/or underlying tissues due to increased collagen deposition and fibrosis causing it to become firm, less elastic, non-liftable and appear thickened.
Systemic sclerosis
Lichen sclerosus
Scleroderma of Buschke (scleroderma diabeticorum)
Pathognomonic lesions
Pathognomonic lesions are clinical findings that are an exclusive characteristic of only a single disease, thus their finding confirms the diagnosis. They are so distinctive that no other condition causes them.
Burrows —> SCABIES
Scutulum —> TINEA FAVOSA


State the most distinguishable clinical aspect of palmoplantar secondary syphilis
The most distinguishable clinical presentation of secondary syphylis is erythematous PAPULES folllowed by Biett’s collarette of scaling: a thin, whitish desquamating ring that sorrounds the syphylis papules.

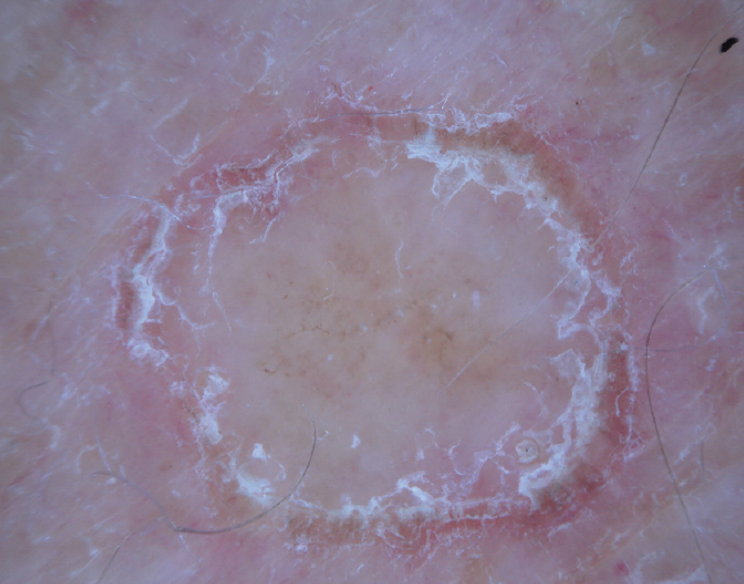
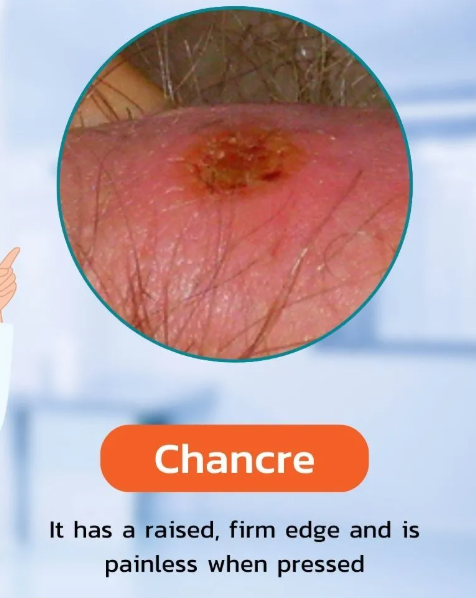
State the differences between chancre and chancroid
CHANCROID is a painful condition, and it is characterized by ulcers that are soft, with irregular edges and a gray base. Other findings are inguinal buboes and tender lymph nodes.

CHANCRE instead is NOT a painful condition, and it is characterized by a single non-painful ulcer. It heals in 3-6 weeks, and it can give rise to a painless lymphadenopathy.
What do you think is the most important cell in the pathophysiology of psoriasis & explain why
MYELOID DENDRITIC CELL
Myeloid dendritic cells are key players in sustaining inflammation. They release pro-inflammatory cytokines that not only fuel the inflammatory response but also boost their own activity, creating a self-perpetuating and vicious cycle.
One of their main roles is to secrete IL-23, which is essential for the survival and expansion of Th17 cells.
In turn, Th17 cells release IL-17, which acts through the ACT1 adaptor protein-dependent pathway and the JAK-STAT pathway to trigger and maintain the expression of various pro-inflammatory genes.
Without myeloid dendritic cells, this entire cascade would be disrupted, meaning the inflammatory response would not be able to occur.
What are the classic signs of Psoriasis Vulgaris?
Psoriasis vulgaris is a type of chronic plaque psoriasis, the most common type (80% of cases). It usually presents as symmetrical, well-defined erythematous plaques covered by thick, silver scaling. It is common especially on extensor surfaces, scalp and back.
Classical signs include:
Auspitz sign: pinpoint bleeding occurring when the scales are removed from the plaque (e.g., due to scratching) due to hypervascularity of the lesion.
Koebner phenomenon: refers to the development of new psoriatic lesions at sites of skin trauma or injury. It may manifest as hyperkeratosis of the palms, especially if associated with repetitive trauma from manual labor. This sign is not specific for psoriasis, as it can also be assessed in other pathologies.
What are the treatments for type I/II/III/IV hypersensitivity reactions?
TYPE I: Remove allergen if possible, antihistamines, corticosteroids, anti-IgE antibody. Epinephrine in case of emergency laryngeal edema.
TYPE II: immunosuppressive therapy (corticosteroids as first line, steroid-sparing agents for long-term control, cyclosporin) AND biologic therapy (Rituximab)
TYPE III: corticosteroids, immunosuppressants, cyclosporine, hydroxychloroquine, topical steroids.
TYPE IV:
Topically: emollients, cleansers, topical steroids, bandages.
Systemically: steroids, cyclosporin, retinoids, anti-TNF, anti-IL17, anti-IL12, anti-IL23, anti-IL4/13, JAK-inhibitors
Illustrate treatment of herpes simplex
Mild labial herpes: topical acyclovir/penciclovir/idoxuridine cream.
Severe infections: oral acyclovir 200–400 mg five times daily for 5 days (1 tablet every 4 hours during waking hours, typically for a 5-day course. You skip the dose during the 8 hours of sleep (i.e., you don't take it during the night).
Why the 4-hour interval? It has been demonstrated that the Herpes virus replicates every 4 hours.
Secondary prophylaxis for frequent reactivation can be given as 400 mg once or twice daily. Higher doses are needed in immunocompromised patients. Caesarean section may be indicated in case of genital herpes in pregnancy (risk of ophthalmic infection of the infant).
What is the anatomical distribution of eczema according to age in atopic dermatitis?
Atopic dermatitis in infants and children (0-5 years) generally manifests at the levels of the cheeks (with sparing of the periorbital and perioral regions), extensor surfaces of the legs and the trunk.
In Children (6-11 Years), it has a flexural distribution with other characteristic manifestations such as atopic dirty neck and "dry" eczema, with exudative lesions becoming crusts.
In adolescents and adults, the areas most involved are the scalp, head, eyelids, neck, shoulders, upper trunk, folds, hands, wrists, feet.

List 5 differences between ICD (irritant contact dermatitis) and ACD (allergic contact dermatitis)
In ICD the major complaint is burning sensation, not itching as in ACD.
ICD evolves a few minutes/hours after exposure, while manifestations of ACD can take up to 24-72h.
In ACD the margins of the lesions are blurred, spreading to the periphery, while in ICD, the margins are sharp, strictly confined to the site of exposure.
In ICD pathogenesis is that of an inflammatory, localized skin response caused by chemical, physical and biological agents, while ACD is a delayed type IV hypersensitivity reaction
In ICD previous contact is not required. In ACD there is always a sensitization.
Which are the 3 main dermoscopic patterns of nevi?
GLOBULAR: globules of similar shape, size and color distributed throughout the lesion.
RETICULAR: diffuse network composed of pigmented lines and hypopigmented holes with minimal variation in their size and color.
HOMOGENEOUS: diffuse homogeneous structureless pattern.
A 35-year-old patient presents to our attention with a histopathological report of melanoma with a Breslow thickness of 0.9mm, non-ulcerated and without mitoses. What is the next surgical step?
Widening of the surgical scar to 1cm and simultaneously SNLB