Caring for a Patient with a Stoma 1
1/40
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
41 Terms
stoma
end of the ureter/small/large intestine that can be seen protruding through abdominal wall
ostomy
surgically created opening in the body for the discharge of body waste
describe a stoma
in tact blood supply
no nerve supply
red/pink colour
can be temp or permanent
name some conditions which predispose to stoma formation
IBD
carcinoma
familial adenoma polyposis
diverticulitis
trauma
incontinence
ulcerative colitis
inflammation of mucosa of colon
ulcerative colitis symptoms
bloody diarrhoea, urgency, mucus
anorexia
anaemia
abdominal discomfort
anal soreness and pain
fever
when is ostomy required in ulcerative colitis
medical treatment not adequate
risk of perforations or perforation has occured
risk of cancer
poor health
what does the ostomy procedure entail in ulcerative colitis
removal of full colon
sometimes rectum is left + ileum connected to it
crohns disease
inflammation and ulcerartion
can occur anywhere in GIT
Crohns symtoms
rectal bleeding
colicky pain after meals
chronic episodic diarrhoea
weight loss and anaemia
oral manifestation
crohns ostomy treatment
affected part is removed
bowel ends rejoined and protected by temporary ileostomy or colonostomy
risk of recurrence
familial polyposis coli
inherited condition
polyps form on large bowel - risk of malignancy
familial polyposis coli treatment
colon + rectum are removed
ileorectal anastomosis in some cases
ilerotectal anastomosis
ileum connected to rectum
diverticular disease
caused by lack of fibre in diet - high pressure in bowel
faeces become trapped in diverticula -> inflammation, pain and bleeding
diverticulitis symptoms
acute abdominal pain
fever
constipation or frequent defecation
abdominal mass
carcinoma - colorectal
cancer
insidious and symptoms are late
colorectal carcinoma symptoms
change in bowel habit
rectal bleeding
colorectal carcinoma treatment
surgery
chemo
biological therapy
radiotherapy
diseases predisposing to urostomy formation
spinal cord
malfunction
diabetic neuropathy
cancer
congenital defects
what is a temporary ostomy procedure
possibility of being reversed with another operation
minimum 6 weeks
what is a permanent ileostomy procedure
will not be reversed
can be due to not having enough bowel to create healthy pathway
3 most common ostomy procedures
colostomy
ileostomy
urostomy
colostomy
surgical opening of the large bowel
output = semisolid/ solid
odour can be an issue
stoma usually flush, skin may protrude
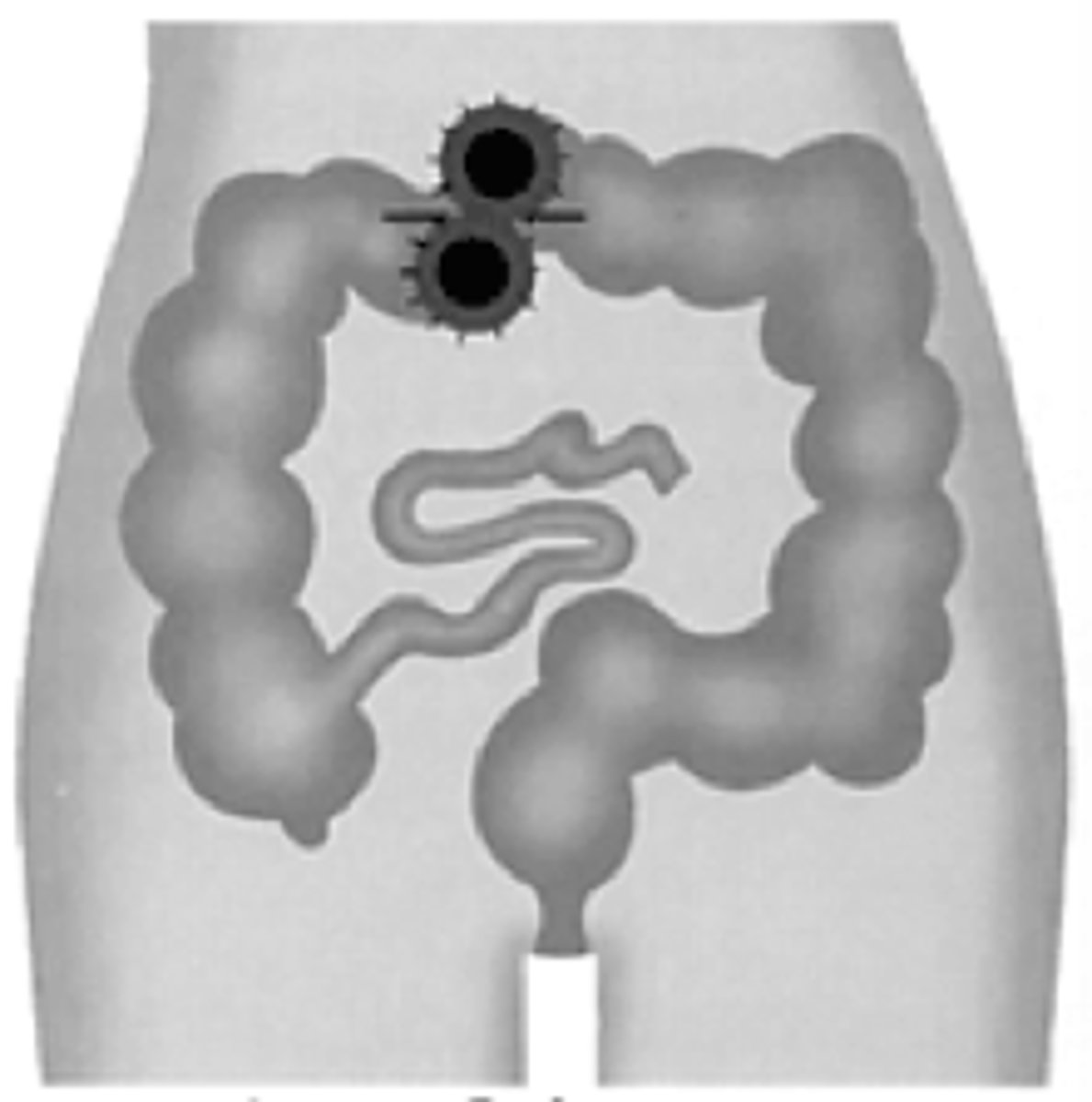
temporary loop colostomy
usually LHS
can be RHS above umbilicus
one stoma with two holes
can be reversed easily
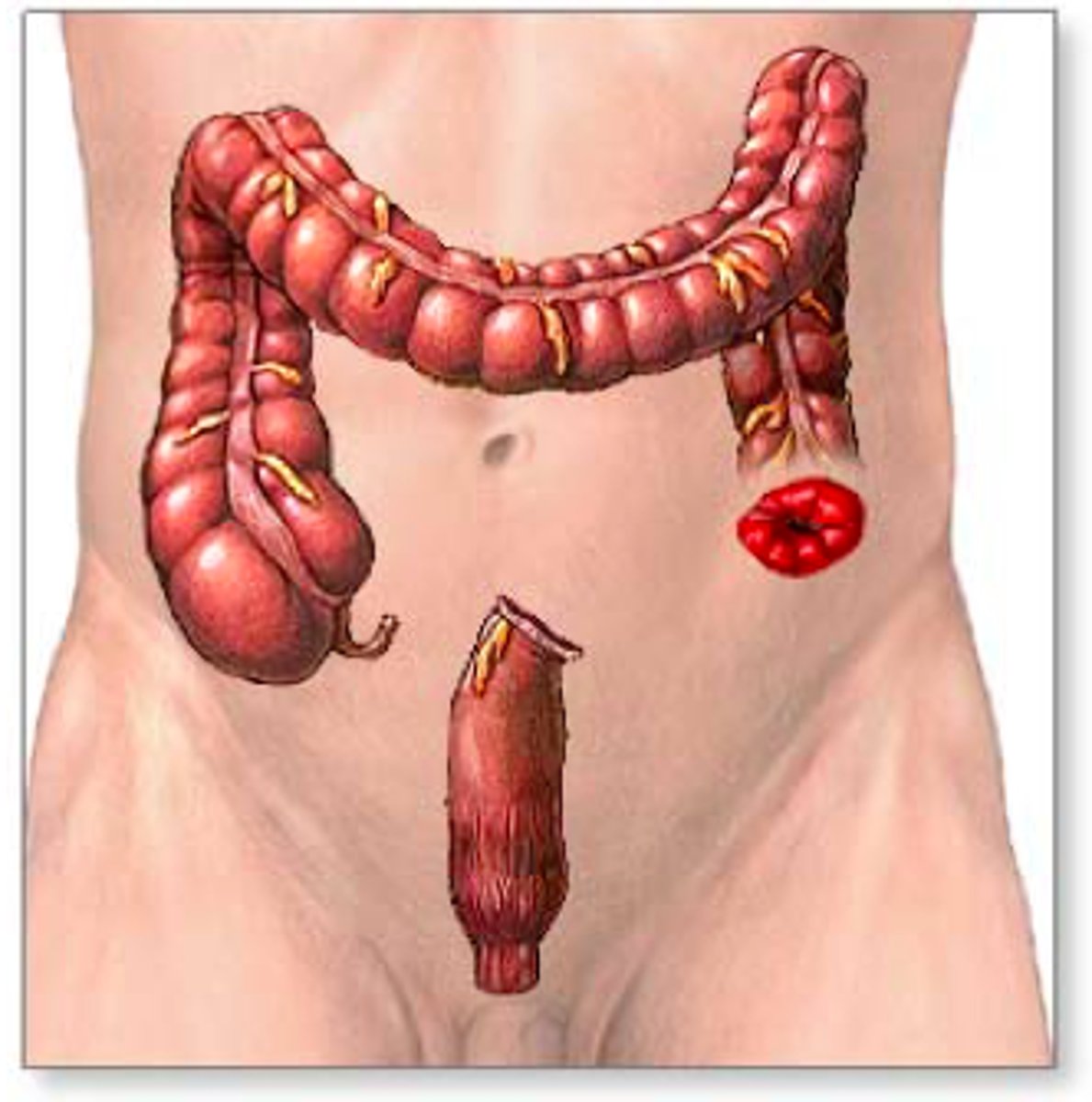
terminal colostomy
usually on LHS
one stoma on abdomen wall
sometimes will have second stoma called mucous fistula
more complex reversing
ileostomy
opening from small intestine/ ileum
output = liquid/ semisolid containing digestive enzyme which can irritate the skin
protrudes 2-3cm
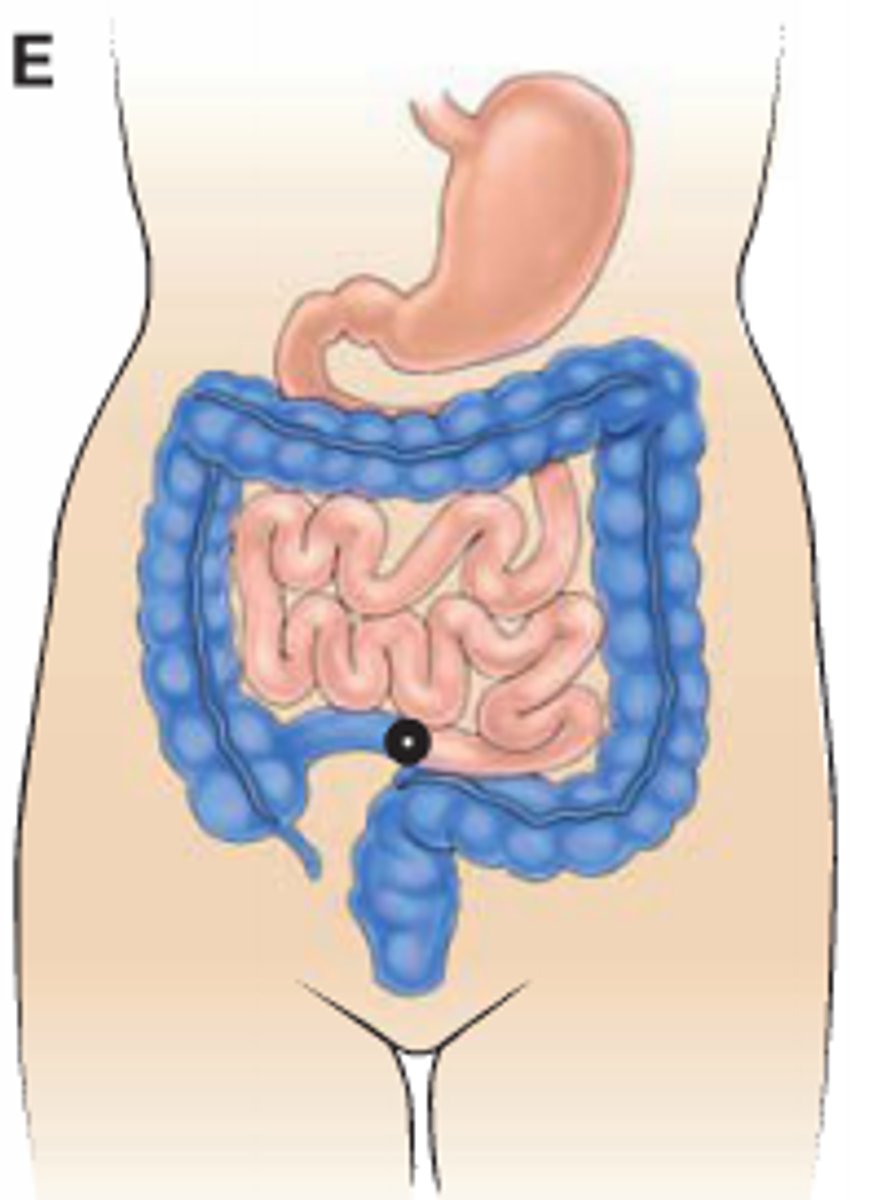
temporary loop ileostomy
usually RHS below umbilicus
first choice for temporary stoma
allows resting of whole colon
advantages of loop ileostomy over loop colostomy
less bulky
possible to site well to allow good management
effluent is more predicatble
terminal ileostomy
entire colon needs to be removed
ileum then brought out through a 2cm incision in rectum to a length of 6/7cm
sutured to abdominal wall - prevents from retracting
then turned inside out
urostomy
ileal conduit = most common
10-20cm isolated ileum with blood supply
ureters mobilised and attached into isolated ileum
other end used to form stoma
pre op patient prep
- 3 steps
early referral to stoma nurse
psychological prep
physical prep
psychological prep
improves recovery rate
prepare post op plan
counselling
physical prep
bowel evacuation
stoma siting
name some stoma sites to avoid
old scars, skin disorders
belly button
groin/ pubic areas
waistline
site which cannot be seen by patient
post op care
careful observation of stoma
monitor - size, swelling, temp, colour, quantity + consistency of material
pain
electrolyte balance
management
perianal wound care
3 types of bags
closed/ non drainable
drainable
urostomy
closed
no opening
used when faeces are well formed - colostomy
discard after use - 1/2x a day
fitted with integral flatus filter
drainable
open end
ileostomy pts always
colostomy - watery faeces
changed every 2-4 days
seal = clip or roll and click
urostomy bag
fitted with drainage table and anti reflux valve
change every 2-3 days
overnight drainage bags available
name some appliances
one piece
two piece - flange and bag
need to make sure appliances fit well to avoid complications