Week 9: Gestational complications
1/124
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
125 Terms
Gestational Hypertensive Disorders
Gestational HTN
Preeclampsia
Eclampsia
Gestational HTN
after 20 weeks gestation there is an increase in BP and there are no other changes
BP is > 140/90
Cause of gestational HTN
placenta not getting enough blood so mom’s BP increases to increase BF to placenta
Preeclampsia
A serous BP disorder developing after 20 weeks of pregnancy, characterized by high blood pressure (≥140/90) and signs of organ damage
Preeclampsia types
Kidney
CNS
Liver
Preeclampsia signs and symptoms
Kidney
Proteinuria (kidney issues)
Neuro
HA (can’t be treated with Tylenol)
Blurred vision
Liver issues
Epigastric pain
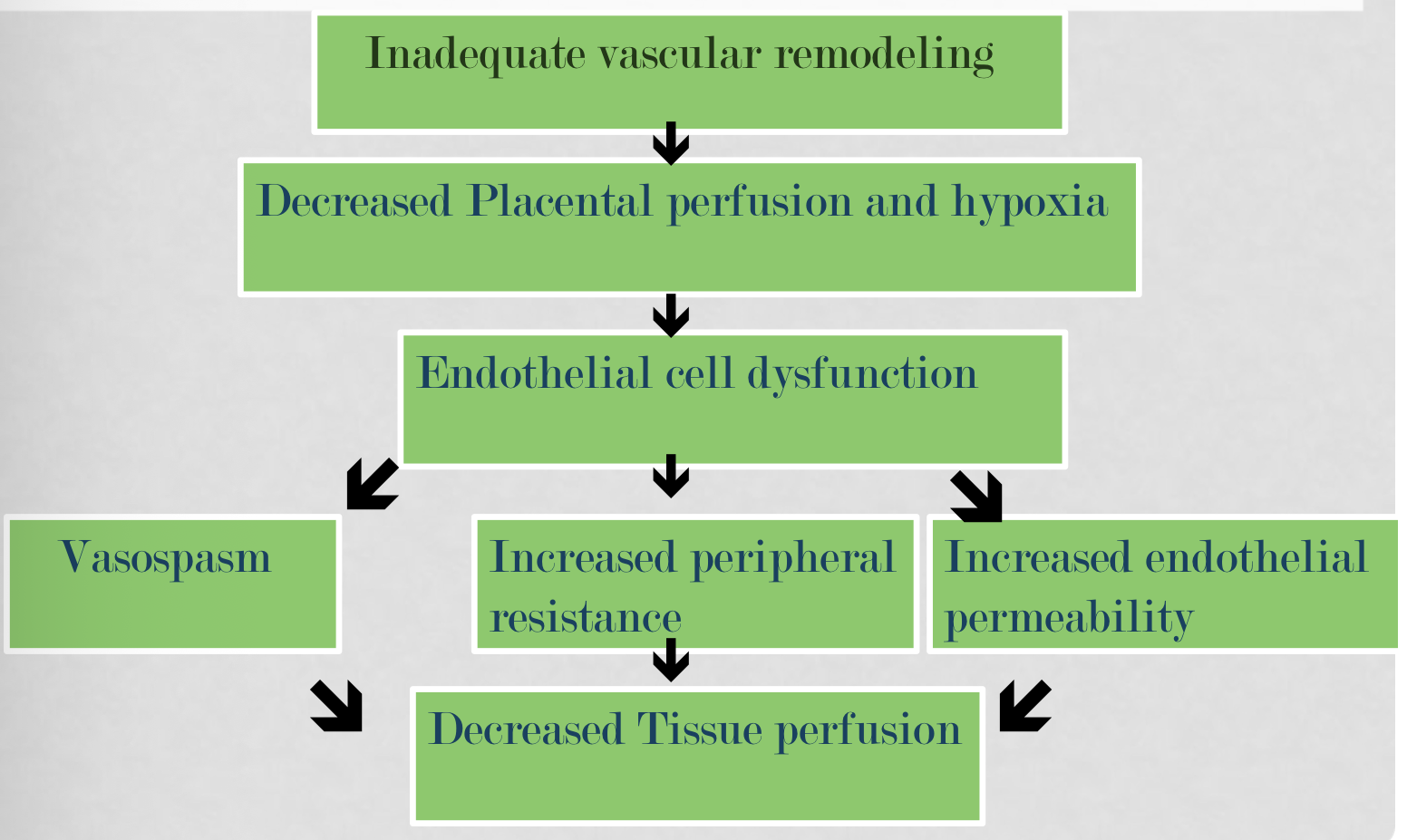
Preeclampsia vasospastic disease
widespread vasospasm and vascular dysfunction, leading to reduced blood flow (ischemia) in organs like the brain, kidneys, and liver
BP mild vs severe
Mild: >140/90
Severe: >160/110
Preeclampsia proteinuria methods to determine
30 mg/dl (1+ on dip) on at least 2 random connections 6 hrs apart
Protein/creatinine ratio >0.3
24 hour urine collection — >300 mg
Preeclampsia core pathophysiology
Poor perfusion
Not HTN
Pathophysiology of preeclampsia
Preeclampsia risk factors (12)
Nulliparity or new partner
Family or personal history of the disease
Obesity
Maternal age <20 or >35
Multiple gestation (larger placenta)
African decent
Smoking
Diabetes
Chronic HTN
Renal or collagen disease
Periodontal disease and infections (UTI hx)
Previous negative pregnancy outcome (IUGR, fetal death)
Mild preeclampsia diagnostics
BP
Protein
Urine output In ml/hr
HA
Visual changes
Epigastric pain/nausea
Liver function
Pulmonary edema
General edema
Placental perfusion
Always: BP >140/90
AND
Protein elevated
OR
Urine output 25-30 mL/hr
HA — absent/transient
Visual changes — absent
Epigastric pain/nausea — absent
Liver function — normal
Pulmonary edema — none
General edema — face or fingers
Placental perfusion — reduced
Severe preeclampsia diagnostics
BP
HA
Visual changes
Epigastric pain/nausea
Liver function
Pulmonary edema
General edema
Placental perfusion
Always: BP >160/110
AND
Protein/creatinine elevated
HA — persistent or severe
Visual changes — blurred, photophobia, scotoma
Epigastric pain/nausea — may be present
Liver function — may be impaired
Pulmonary edema — may be present
General edema — severe and sudden
Placental perfusion — decreased perfusion, IUGR, none General edema-reassuring fetal testing
Eclampsia
life-threatening emergency defined by seizures (convulsions) in a pregnant or postpartum person with preeclampsia
without history of seizures
Chronic HTN pregnancy
HTN occurs before pregnancy or before 20 weeks gestation that is diagnosed during pregnancy
Persists longer than 12 weeks postpartum
Antihypertensives for chronic HTN during pregnancy
Beta blockers during pregnancy
cannot be on ACE inhibitors
Chronic HTN makes a pregnant woman at a higher risk for developing _____
preeclampsia
Chronic HTN with Superimposed Preeclampsia
HTN before 20 weeks gestation with:
New onset proteinuria that is >500 mg in 24 hrs
Sudden uncontrolled HTN
Chronic HTN with Superimposed Preeclampsia — diagnosis if woman has proteinuria before pregnancy
new thrombocytopenia and increased LFT
HELLP syndrome
A severe form of liver preeclampsia, characterized by:
Hemolysis
Elevated Liver enzymes
Low Platelet count
**HELLP nursing assessment and physical examination
BP
Weight
Edema
Neurological changes
Severe epigastric pain
Pulmonary edema
Labs
HELLP syndrome: weight
retention of water leads to 3rd spacing and edema of the hands and feet
HELLP syndrome: Neurological changes
DTRs and clonus
HA
Blurry vision/spots
HELLP syndrome: DTRs
normal DTRs is +2
if HELLP is getting really bad, the woman may become hyperreflexic (+3 or +4)
HELLP syndrome: Hyperreflexic DTRs treatment ent
magnesium sulfate
HELLP syndrome: Clonus
When a pregnant woman’s food is flexed and rather than falling back into place (normal), the foot will “click” back into place
these are involuntary muscle contractions and relaxations
to be positive there must be 3 or more “clicks”
Preeclampsia: nursing assessments for mother and fetus
Mother:
patient education of cardiac, renal, and pulmonary system
provide a quiet environment
Fetus:
kick counts
EFW at diagnosis
NST
BPP
umbilical artery Doppler
Preeclampsia: bed rest position
side lying
Preeclampsia: diet
NO sodium restriction
limit excessively salty foods
No caffeine
No ETOH
Preeclampsia: medications (2)
MgSO4 — seizure prophylaxis
Anti-HTN meds (hydralazine and labetalol)
Preeclampsia: delivery indications
Always in the mom’s best interest when s/s are severe
Labor can be induced as early as 30 weeks if severe
Induction planned at 34 weeks for severe
Induction at 37 weeks for mild
Eclampsia
progression of preeclampsia to a more severe form, characterized by the same sx as preeclampsia but also seizures
this is a medical emergency!
Eclampsia: seizure injury prevention
Seizure requires immediate treatment — may not have any warning
Side rails up
Side lying
Be ready to suction and administer O2
Eclampsia: assessment post-seizure (7)
Pulmonary edema
Circulatory and renal failure
Cerebral hemorrhage
Abruption
Contractions
Cervix
FETUS!
Eclampsia: delivery
delivery after stabilization and is most often a c/s
Eclampsia: delivery and Pitocin indications
Pitocin induction if >30 weeks gestation or if <30 weeks and favorable cervix
Eclampsia: c/s indications
if <30 weeks gestation and unfavorable cervix
reduces risk associated with delivery of very preterm infant
Eclampsia: MgSO4
used for seizure prophylaxis
NOT for HTN
Used through induction, labor, and 24 hours after delivery
*MgSO4 dosing for seizure prophylaxis
4-6 grams over 30-60 mins
Followed by 2 g/hr
Therapeutic serum levels is 4-7.5 mEq/dl
How long with MgSO4 used for eclampsia?
Used through induction, labor, and 24 hours after delivery
Symptoms of MgSO4 toxicity
During bolus she will feel very hot and horrible, but after bolus she should feel fine — if she doesn’t feel better after bolus this is a bad sign
Slowed speech
Decreased LOC
Solemness
Hyporeflexia
Slowed RR
*Eclampsia nursing assessment
BP
RR
UO
Neurological
DTRs
____ in protein in urine or edema
BP >160/110
RR <12 breaths/min
UO <30 cc/hr
Neuro: HA, visual changes
DTR: increase (worsening condition) or decrease (mag tox)
Increase in proteinuria or edema
Eclampsia: abnormal lab values — high or low
High
MgSO4
Platelets
Creatinine clearance
Uric acid levels
AST and ALT
PT and PTT
Down
Fibrinogen
Antidote for mag toxicity
calcium gluconate
Early Pregnancy Bleeding (EPB)
bleeding that occurs within first 12 weeks of pregnancy
EPB causes
Spontaneous abortion (miscarriage)
Incompetent cervix
Ectopic pregnancy
Hydatiform Mole
Hydatiform Mole
Non-cancerous tumor that develops in the uterus due to an abnormal fertilization, causing grape-like cysts instead of a healthy placenta
Spontaneous Abortion (SAB)
A pregnancy that ends before 20 weeks gestation
< 500 grams
Fetus cannot survive outside of uterus
Early SAB
pregnancy lost before 12 weeks gestation
Early SAB causes
Endocrine imbalance
Immunologic factors
Maternal infection
Systemic disorders
Genetic factors (chromosomal abnormalities are the most common cause)
Late SAB
pregnancy lost between 12-20 weeks gestation and is a result from maternal causes
Late SAB causes (7)
AMA
Increased parity
Chronic infections
Incompetent cervix (cervical insufficiency)
Reproductive tract anomalies
Inadequate nutrition
Recreational drug use
SABs 5 classifications
Threatened
Inevitable
Incomplete
Complete
Missed
SAB: Threatened abortion
occurs when vaginal bleeding occurs before the 20th week of pregnancy, potentially signaling early pregnancy loss, though the fetus is usually still alive and the cervix remains closed
SAB : Threatened abortion characteristics
Light bleeding
Mild uterine cramping
No passage of tissue
No cervical dilation
SAB: Inevitable abortion
occurs when vaginal bleeding and cramping are accompanied by the opening of the cervix, making the loss of pregnancy unavoidable, generally before 20 weeks
SAB: Inevitable abortion characteristics
Moderate to heavy bleeding with presence of tissue
Mild to severe cramping
Cervical dilation
ROM
Passage of products of conception (POC) inevitable
SAB: Incomplete abortion
Fetal expulsion with placental retention
SAB: Incomplete abortion characteristics (3)
Moderate to heavy bleeding with passage of tissue
Severe cramping
Dilated cervix with tissue in os
SAB: Complete abortion
Passage of all fetal tissue — fetus and placenta
SAB: Complete abortion characteristics
Closed cervix after all tissue has passed
Slight bleeding
Mild uterine cramping
SAB: Missed abortion
fetal death without expulsion
SAB: Missed abortion characteristics
Uterus decreases in size
Limited bleeding and cramping
No cervical change
Diagnosed by US
At risk for DIC!
Why are people with a missed abortion at risk for DIC?
baby isn’t circulating blood back to mom anymore because it is dead
SAB: Missed abortion treatment
Providers suggest a D&C, but the mother could also go home and pass it on her own (unless she becomes septic)
SAB: Septic abortion
life-threatening uterine infection occurring before, during, or after a SAB
SAB: Septic abortion characteristics
Bleeding varies — foul odor
Uterine cramping varies
Passage of tissue varies
Cervix dilated
SAB: Septic abortion treatment
Immediate termination via D&C!!!
Antibiotics
Assess for shock
SAB management: Threatened
Will miscarry or carry to term
should have reduced activity, not bedrest because it can increase chances of a clot developing
SAB: Threatened subchorionic hematoma
a collection of blood between the placenta and uterine wall, often causing bleeding in early pregnancy and acting as a common cause of "threatened abortion"
SAB: repetitive
having previous miscarriage increases risk of another SAB
once you have 3 miscarriages, your body “resets” and your risk for another SAB decreases
SAB: Inevitable and incomplete management
D&C to remove all tissue
SAB: Complete management
no treatment bc no leftover tissue
must do u/s to make sure everything is out
SAB: Missed abortion management
Aborts spontaneously
May require uterine evacuation to prevent infection and DIC
If mom is ___, _____ must be administered after a SAB because…
If mom is Rh-, rhogam must be administered after a SAB because fetal blood could mix with mom’s after it dies
Symptoms associated with bleeding during pregnancy (3)
Cramping
Pain
N/V
Cause of a late abortion
incompetent cervix
results in the passive and painless dilation of the cervix during the second trimester
Incompetent cervix etiology
Hx of cervical laceration/trauma
Excessive cervical dilation during curettage/biopsy
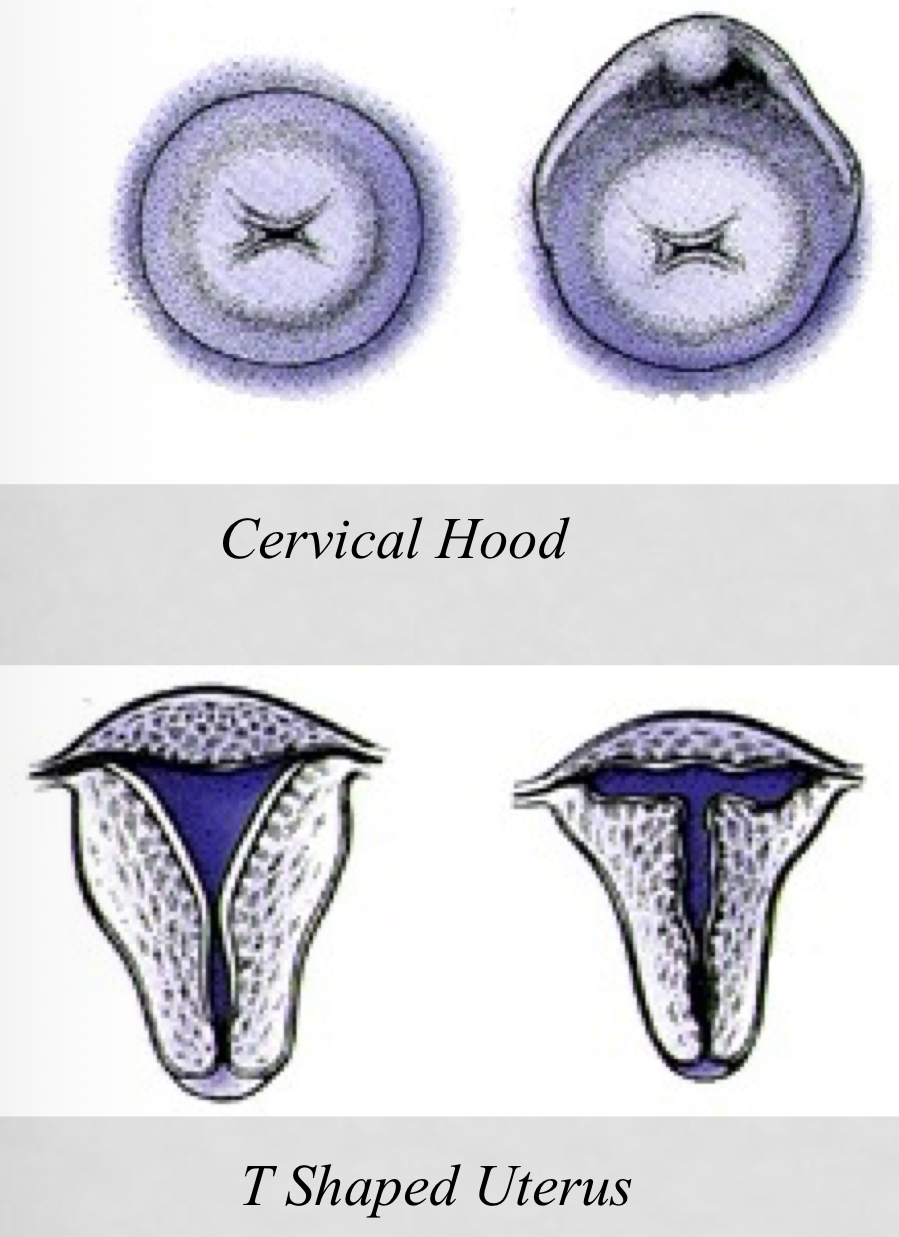
DES daughter (not used after 1971)
Reproductive tract anomolies
DES Daughter
DES was used prior to 1971 to prevent abortion, miscarriage, and premature labor by preventing full expansion of the uterus. Since the uterus wouldn’t fully expand, it would limit/prevent complete fetal development.
Incompetence cervix: signs and symptoms (5)
Pressure and sensation in vagina
Leaking of fluid
Speculum exam shows membranes bulging through os
Fetal parts in vagina
Short cervix on US
Cerclage
surgical procedure to stitch cervix closed
Done at 10-28 weeks gestation for patients with have previous losses bc of an IC
Incompetent cervix: treatment
Prophylactic cerclage — placed at 10-28 weeks and removed at 37 weeks
Repeated with each successive pregnancy
Ectopic pregnancy
fertilized ovum is implanted outside of the uterus
most often in fallopian tube
leading cause of 1st sem abortion And infertility
Ectopic pregnancy danger
may cause maternal hemorrhage and death
The fertilized egg grows in the fallopian tubes and overwhelms it bc it can’t expands very much
Ectopic pregnancy: risk factors (10)
Previous bilateral tubal ligation (BTL) — after reversal or failure after cautery (tubes tied)
STIs/PID — chlamydia increases risk bc of pelvic inflammatory diseases
Abd or pelvic surgery
Previous ectopic pregnancy
Endometriosis
Previous uterine masses
IUD
Infertility meds/treatments
Progestin-only contraceptive use
Smoking
Adnexal
structures adjacent to the uterus
Ovaries
Fallopian tubes
Surrounding connective tissue
Ectopic pregnancy: signs and symptoms
Missed period
Sx of pregnancy
Adnexal (uterine adjacent) fullness
Unilateral, bilateral, or diffuse dull adnexal pain
Vaginal bleeding
Increased pain with rupture (6-12 weeks)
*Referred shoulder pain
Shock r/t rupture and hemorrhage
Ectopic pregnancy: pharmacological treatment
Methotrexate
stops cell growth and allows body to absorb cells
can be primary treatment if un-ruptured ectopic
Ectopic pregnancy: treatment
US for IUP
hCG discriminatory zone
Serial quantitative β-hCG levels — doubles daily
Laparoscopy
Progesterone levels
hCG discriminatory zone
threshold serum β-hCG level above which a normal intrauterine pregnancy should be visible. If hCG exceeds this level and no sac is seen, it suggests a potential ectopic pregnancy
typically 1,500-2000 mIU/mL for transvaginal US
6000-6500 mIU/mL for abdominal US
Hydatidform Mole
noncancerous tumor that develops in the uterus due to abnormal fertilization, resulting in an abnormal placenta, no viable fetus, and grape-like cyst formation
No fetus develops!
Abnormal fertilization of egg whose nucleus has been lost — sperm duplicates itself very fast
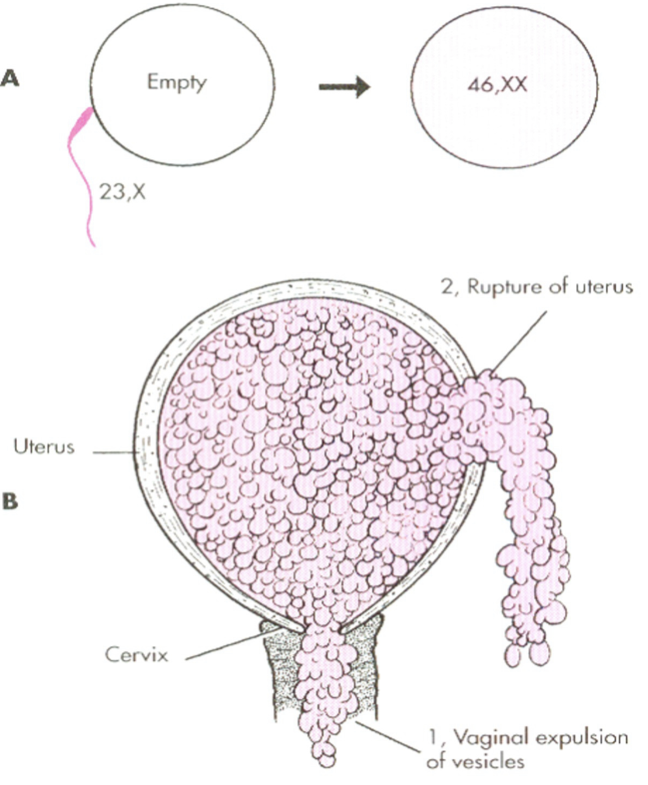
Complete vs Partial Mole
Complete moles: arise from an empty egg fertilized by one or two sperm (diploid, 46,XX/XY), resulting in no fetus and high-risk cancer potential, characterized by "grape-like" chorionic villi.
Partial moles: occur when a normal egg is fertilized by two sperm (triploid, 69,XXX/XXY/XYY), often including fetal tissue and having lower malignant potential
Hydatidform Mole: signs and symptoms (8)
Vaginal bleeding (dark brown to bright red)
Size of fetus is > than expected based on date of conception
No signs of IUP (no FHR, movement, or parts on US)
Anemia from blood loss
Abnormally high levels of hCG (>100,000)
Preeclampsia btwn 9-12 weeks gestation (bc mole is accelerating everything)
Passage of grape-like vesicles
“Snowstorm” appearance on US
Hydatidform Mole: Treatment (5)
Most vesicles pass spontaneously around 16 week
Will have D&C
Follow-ups with frequent US and labs
Pregnancy contraindicated for 1 year
Rhogam (bc sperm blood type is likely different than mom’s
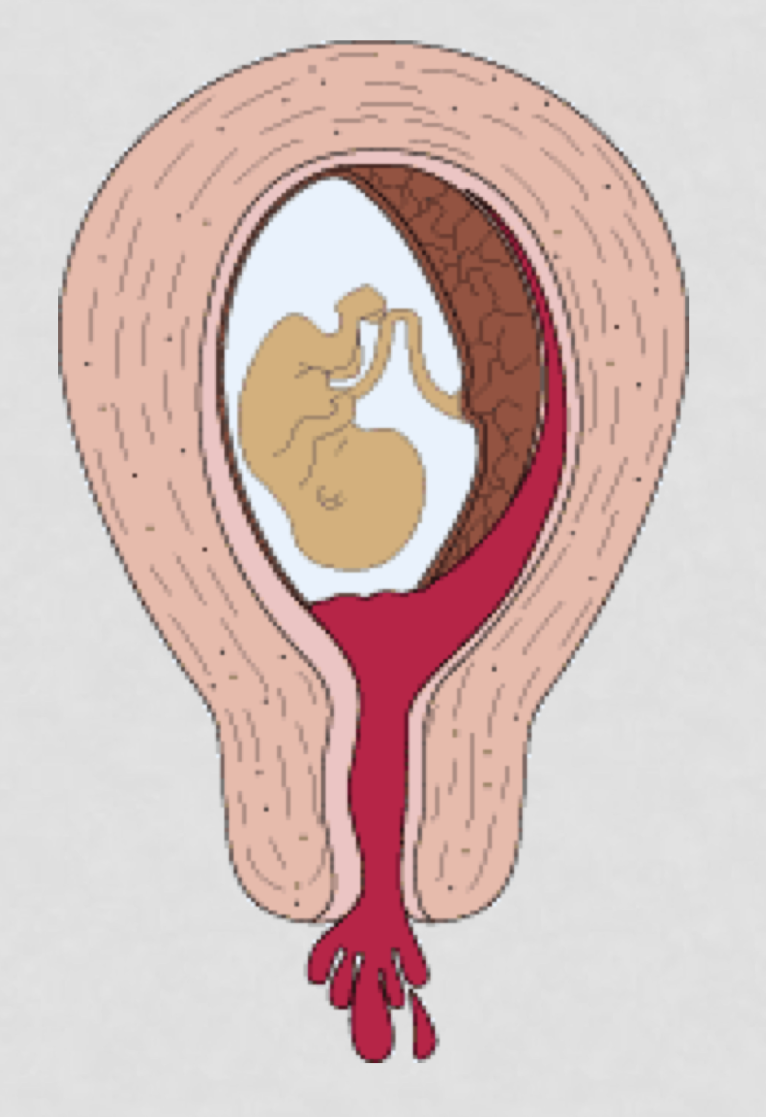
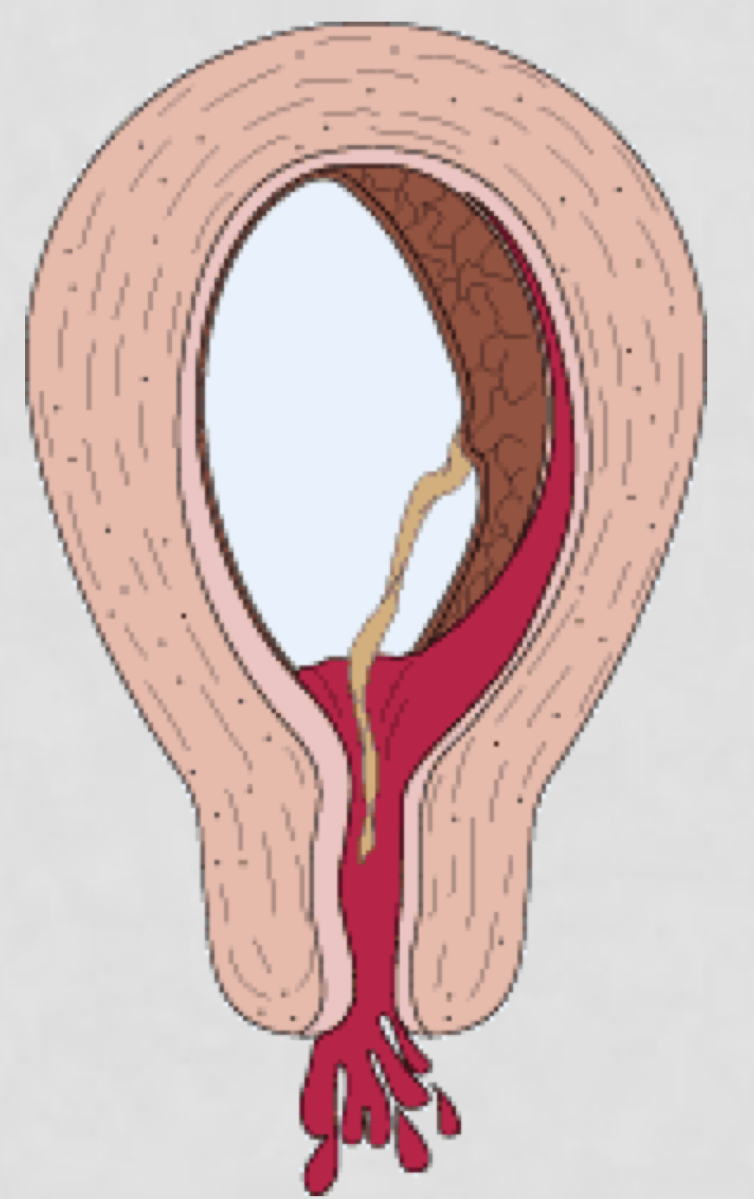
3 types of late placental bleeding
Placenta Previa
Abruptio Placenta
Cord Insertion
Placenta Previa
Placenta covers part or all of the cervix
Partial placenta previa

Complete placenta previa

Marginal placenta previa
