cardiovascular system
1/101
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
102 Terms
cardiac muscle characteristics and structure
- only found in the heart
-striations of repeating sarcomeres
-small w single nucleus
-arranged in layers and surround hollow cavities
-troponin and tropomyosin present
- T-tubules present
-SR present
-joined by intercalated discs
intercalated disks
link cardiac muscle cells together both mechanically and electrically
2 distinct features:
1. desmosomes: mechanically join cells with protein filaments
2. gap junctions: electrically join cells (allows ion flow)
functional syncytium
stimulation within a chamber results in a synchronous contraction of that chamber; each heart chamber functions as if it were one cell or a functional unit
L-type Ca2+ channels
(cardiac muscle excitation-contraction coupling)
specialized voltage-gated Ca2+ channels named for their long-lasting current
-located on sarcolemma and T-tubules (highly concentrated)
prolong cardiac muscle action potential and refractory period
Ryanodine Receptors
Ca2+ ch in cardiac SR
-opened by binding Ca2+ in cytosol rather tan by voltage as in skeletal muscle
-calcium-induced calcium release
Calcium-Induced Calcium Release
small initial influx of Ca2+ into the cell triggers the release of much larger quantity of Ca2+ from SR
tetanic contraction (tetanus)
sustained, maximum muscle contraction
-caused by high-frequency motor neuron stimulation, where muscles cannot relax between stimuli
can cardiac muscles exhibit tetanus? explain.
no because of L-type Ca2+ ch
-cardiac cells have a long refractory period of about 250ms
-cardiac cell contracts and relaces before it can be stimulated again which makes tetanic contraction impossible
cardiac muscle innervation (sympathetic and parasympathetic)
sympathetic:
-release NE
parasympathetic
-contained in vagus nerves (cranial nerve X)
-primarily release ACh
-muscarinic receptors
cardiovascular system overview and functions
heart + blood vessels
function: transports blood throughout the body
-delivery of O2, nutrients; removal of CO2, wastes
perfusion
delivery of blood per time per gram of tissue (mL/min/g)
adequate perfusion
sufficient delivery to maintain cells' health
-requires continual pumping of the heart and open, healthy vessels
what perfuses the heart?
heart is perfused by coronary arteries that supply muscle tissue
-blood inside the heart does not supply the heart w oxygen and nutrients
blood vessels
conduits of cardiovascular system that transport blood
three main types: arteries, veins, and capillaries
arteries (arterial trunks)
carry blood AWAY from heart
-most (not all) carry oxygenated blood
veins
carry blood back TOWARD the heart
-most (not all) carry deoxygenated blood
capillaries
sites of exchange (ex. of gases)
-b/w blood and air in lungs
-b/w blood and body cells
heart
hollow, four chambered muscular organ that pumps blood throughout the body
anatomic features vital to function:
-two sides
-great vessels
-valves
sides of heart and their functions
right side: receives deoxygenated blood from body and pumps it to lungs
left side: receives deoxygenated blood from lungs and pumps it to body
chambers of the heart
each side has two chambers
-atria (superior chamber)
-ventricles (inferior chamber)
interatrial septum
separates left atrium from right atrium
interventricular septum
separates left ventricle from right ventricle
pericardim
protective fibrous sac surrounding the heart
(a layer of the heart)
do the atria or ventricles have thicker walls?
ventricles (pumping chambers) have thicker walls then atria
is the left or right ventricle thicker?
left ventricle is thicker
-it must generate high pressure to to force blood through systemic circulation
-right just pumps to the nearby lungs
layers of the heart wall
epicardium, myocardium, endocardium (outside to inside)
epicardium
-outermost layer of the heart
-epi=upon
myocardium
-middle layer of heart wall (thickest)
-cardiac muscle cells that contract to pump blood
-myo=muscle
endocardium
-covers internal surface of heart and external surface of valves
-composed of endothelial cells
-continuous with lining of blood vessels
great vessels
transport blood directly to and from chambers of the heart
pulmonary trunk
transport blood away from heart to lungs (artery)
-branches into pulmonary arteries
aorta (descending and ascending)
transport blood away from heart to the rest of the body (artery)
-descending: to lower body
-ascending: to upper body
superior vena cava (SVC)
drain deoxygenated blood from superior body toward right atrium (vein)
inferior vena cava (IVC)
drain deoxygenated blood from inferior body toward right atrium (vein)
pulmonary veins
drain oxygenated blood into left atrium
what are the 2 sets of valves? Made of? function?
1. atrioventricular (AV) valves
2. semilunar valves
-made of endothelium-lined fibrous connective tissue cusps (flaps)
-ensure one-way flow of blood through heart
atrioventricular (AV) valves
sit b/w atrium and ventricle of each side
-right AV valve = tricuspid
-left AV valve = biscuspid or mitral valve
chordae tendineae (tendinous cords)
thin strands of collagen fibers attaching to AV valves
papillary muscles
cone-shaped projections extending from internal ventricle wall
-anchor chordae tendineae
semilunar valves
prevent backflow of blood into ventricles
each has 3 cusps
-pulmonary semilunar valve
-aortic semilunar valve
pulmonary semilunar valve
-located b/w right ventricle and pulmonary trunk
-prevent backflow of blood into ventricles
aortic semilunar valve
-located b/w left ventricle and aorta
-prevent backflow of blood into ventricles
heart sounds
S1 ("lubb") closing of AV valves
S2 ("dub") closing of semilunar valves
heart murmur
abnormal heart sound
-result of turbulence of blood passing through heart
-may be caused by valvular leakage, decreased valve flexibility, or a misshapen valve
basic pattern of circulation
right heart → lungs → left heart → systemic tissues → right heart
pulmonary circulation
the path of deoxygenated blood from the right side of the heart to the lungs
- right ventricle → lungs → left atrium
microcirculation
where exchange of gases, substrate, and waste products occurs b/w the blood and the extracellular fluid
- arterioles → capillaries → venules
-blood vessels return to left side of heart
systemic circulation
the path of oxygenated blood from the left side of the heart to systemic cells
-left ventricle → peripheral organs/tissues → right atrium
-at systemic cells (ex. skin, muscles), blood exchanges gases, nutrients, and wastes
-blood vessels return to right side of heart
1. heart contraction involves 2 events, what are they?
1. conduction system: initiates and propagates an action potential (excitation)
2. cardiac muscle cells: fire action potentials and contract (cross-bridge)
conduction system
initiates and conducts electrical events to ensure proper timing of contractions
-composed of specialized cardiac muscle cells that have action potentials but DO NOT contract
-activity influenced by autonomic NS
sinoatrial (SA) node
initiates heartbeat (pacemaker)
-located high in posterior wall of right atrium
atrioventricular (AV) node
located in floor of right atrium (near right AV valve)
atrioventricular (AV) bundle (bundle of his)
-extends from AV node through interventricular septum
-divides into left and right bundles
purkinje fibers
-extend from left and right bundles at heart's apex
-course through walls of ventricles
nodal cells
-nodal cells in the SA node initiate heartbeat
-exhibit autorhythmicity
-do not have a stable RMP
-common membrane proteins: Na+/K+ pumps, Ca2+ pumps, leak channels
-specific voltage-gated channels: slow ("funny") VG Na+ ch, fast VG Ca2+ ch, VG K+ ch
autorhythmmicity
spontaneously depolarize and generate an action potential
-aka spontaneous firing
resting membrane potential
about 60mV
pacemaker potential
ability to reach threshold without stimulation
cardiac muscle cells
- contain Na+/K+ pumps, Ca2+ pumps, Na+ and K+ leak channels
-resting membrane potential: -90mV
-contain specific VG Ca2+ ch
-fast VG Na+ ch
-L-type (slow) VG Ca2+ ch
-VG K+ ch
tetanic contraction (tetanus)
sustained, maximum muscle contraction
caused by high frequency motor neuron stimulation, where muscles cannot relax b/w stimuli
cardiac muscles and tetanus
cardiac muscle cannot exhibit tetanus
cardiac cells have a long refractory period = cell cant fire a new impulse
plateau phase leads to refractory period of about 250ms
cardiac cell contracts and relaxes before it can be stimulated again
electrocardiogram (ECG/EKG) recording
skin electrodes detect electrical signals of cardiac muscle cells
tool used to diagnose
measure summation fof many cardiac cell action potentials (APs) → not single AP
cardiac cycle
all events in the heart from the start of one heartbeat to the start of the next
includes systole and diastole
Contraction increases pressure; relaxation decreases it
blood moves down its pressure gradient (h → l)
Valves ensure that flow is forward / one-directional (closure prevents backflow)
ventricular activity
most important driving force
systole (ventricular contraction)
raises ventricular pressure
diastole (ventricular relaxation)
lowers ventricular pressure
4 main events of cardiac cycle
ventricular filling
isovolumetric ventricular contraction
ventricular ejection
isovolumetric ventricular relaxation
ventricular filling
1st event
both AV valves open → blood floes into ventricles
semilunar valves closed
ventricles filled to end-diastolic volume (EDV)
amount of blood just before systole
isovolumetric ventricular contraction
2nd event
beginning of systole
isovolumetric
all 4 valves are closed
no blood can be ejected
ventricular pressure increases
isovolumetric
associated with no volume change
all 4 valves are closed
ventricular ejection
pressure in the ventricles exceeds pressure in aorta
and pulmonary trunk
→ semilunar valves open → blood ejected
from ventricles
• AV valves closed (chordae tendineae and
papillary muscles) to ensure one-directional
flow of blood
• Stroke volume (SV)
Volume of blood ejected per cardiac
cycle
Isovolumetric ventricular relaxation
4th event
beginning of diastole
isovolumetric
all 4 valves are closed
end systolic volume
end systolic volume
amount of blood remaining in ventricle after contraction finishes
ESV=EDV-SV
cardiac output
amount of blood pumped by a single ventricle in one minute (e.g., L/min)
measure of effectiveness of cardiovascular system
determined by heart rate and stroke volume
HR x SV = CO
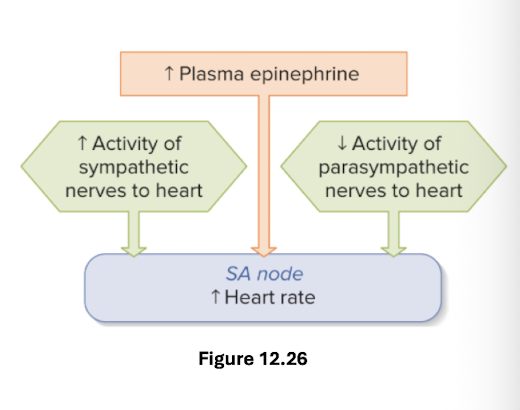
what influences HR
chronotropic agents
autonomic NS
hormones
what influences SV?
preload
inotropic agents
afterload
chronotropic agents
external agents that change HR
alter activity of nodal cells
autonomic NS
parasympathetic : dec HR
sympathetic: inc HR
hormones
epi: inc HR
preload
pressure stretching heart wall before shortening
inc by filling heart w more blood (venus return)
inc EDV
frank starling mechanism
force of ventricular contraction directly proportional to the initial length (stretch) of myocardial fibers
greater stretch (EVD/preload) → actin and myosin overlap in more optimal pattern → stronger contraction → higher SV
ionotropic agents
external agents that affect stroke volume by alterign contractility
inc or dec avaliable Ca2+
sympathetic nerve stimulation : inc SV
epi : inc SV
contractility
force of contraction independent of stretch (EDV)
afterload
how hard the heart must work to eject blood from ventricles
greater the “load” (pressure of blood in arteries) → inc work of cardiac muscle to eject blood → dec stroke volume
atherosclerosis
(plaque in vessel linings) increases afterload
plaque dec artery diameter → inc resistance to blood flow
general structure of vessels
vessel walls are composed of 3 layers called tunics
lumen : space inside of vessel where blood resides
tunica externa
outermost layer of vessel wall
helps anchor vessel to other structures
tunica media
middle layer of vessel wall
circularly arranged layers of smooth muscle cells w elastic fibers
contraction causes vasoconstriction
relaxation causes vasodilation
vasoconstriction
narrows lumen → inc pressure
vasodilation
widens lumen → dec pressure
tunica intima
innermost layer of vessel wall
endothelium of simple squalamous epithelium
provides smooth surface for blood flow
arteries
heart ventricles → arteries → arterioles
contain smooth muscle
thick walled
large quantity of elastic tissues → elasticity
large diameter → low resistance
arteriole blood pressure depends on
volume of blood
how easily vessels can stretch → compliance
compliance
change in (Δ) volume/change in (Δ) pressure
systolic pressure
maximum arterial pressure just before ventricular ejection
diastolic pressure
min arterial pressure just before ventricular ejection
what is arterial pressure recorded as?
systolic/diastolic
capillaries
small vessels connecting arterioles to venules
thin wall of endothelial cells and basement membrane (no surrounding smooth muscle or elastic tissue)
small diameter : optimal for exchange between blood and tissue fluid
3 types of capillaries
continuous
fenestrated
sinusoid
capillary beds
groups of capillaries functioning together
precapillary sphincter
precapillary sphincter
smooth muscle ring that helps determine volume of blood each capillary receives
veins
venules → veins → heart atria
thinner, less eslatic fibers, and less muscle then arteries
venous valves
prevent blood from pooling in the limbs; ensure blood flow toward heart