Multiple Sclerosis
1/59
Earn XP
Description and Tags
Wecht
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
What is MS?
+characteristics of Disease
Permanent, disabling, unpredictable autoimmune disorder
o Inflammation damages the myelin sheath which breaks down communication between the central nervous system (CNS) and the periphery
Two main characteristics of the disease
o Multiple neurologic symptoms accrue over time
o Plaques and lesions are seen in multiple areas of the brain and spinal cord
MS Pathophysiology
+hypotheses
Exact cause is unknown
Hypotheses include:
Inflammatory cause
Autoimmune cause
MS Inflammatory Hypothesis
T Cell Differentiation:
Th1: increase inflammation
bind inflammation cytokines → BBB breakdown → inflammatory mediators get into CNS → neurodegredation → strips myeline sheets → AND
Th2: decrease inflammation
Th17: increase inflammation
problem
Treg: regulatory
problem
can be pro or anti depending on environment (plascitiy)
in MS leads to inflammatory
MS Autoimmune Hypothesis
+offending vriuses
Molecular Mimicry
Viral infection occurs and immune response is generated to the antigen
then
Virus has a similar structure to the protein in the myelin
then
Immune system attacks both the antigen of the virus AND the myelin
Viruses
Epstein barr
CMV and herpes
MS Risk Factors
Having a first degree relative with MS
HLA DRB1*1501 gene
Vitamin D levels < 75 nmol/L
Smoking
High Epstein Barr (EBV) virus antibodies
Living in an environment farther from the equator
correlates to vitamin D levels?
Caucasian, northern European ancestry
Female
Obesity
Symptoms of MS
+primary, secondary, tertiary + ex for each
Primary: Direct consequence of conduction disturbances
Caused by the demyelination and axonal damage in the CNS
ex: Visual complaints, Cognitive changes, Gait instability, Pain
Secondary: Complications resulting from primary symptoms
ex: Recurrent UTIs, Depression, Bed sores
Tertiary: Symptoms that relate to the effect of the disease on the patient's life
ex: Financial burden, Emotional burden, Social issues
MS Initial Symptoms
+general, most common, others
Disease of exclusion - vague symptoms
Most common; optic neuritis
Others
Different types of pain
most specific to MS: “MS Hug”
squeezing or tightness
tingling
pins and needles
electric shock
Disgnosis of MS
+what to take into consideration → NEEDED?????
S/s
Dissemination in time
Dissemination in space
No other explanation for clinical findings
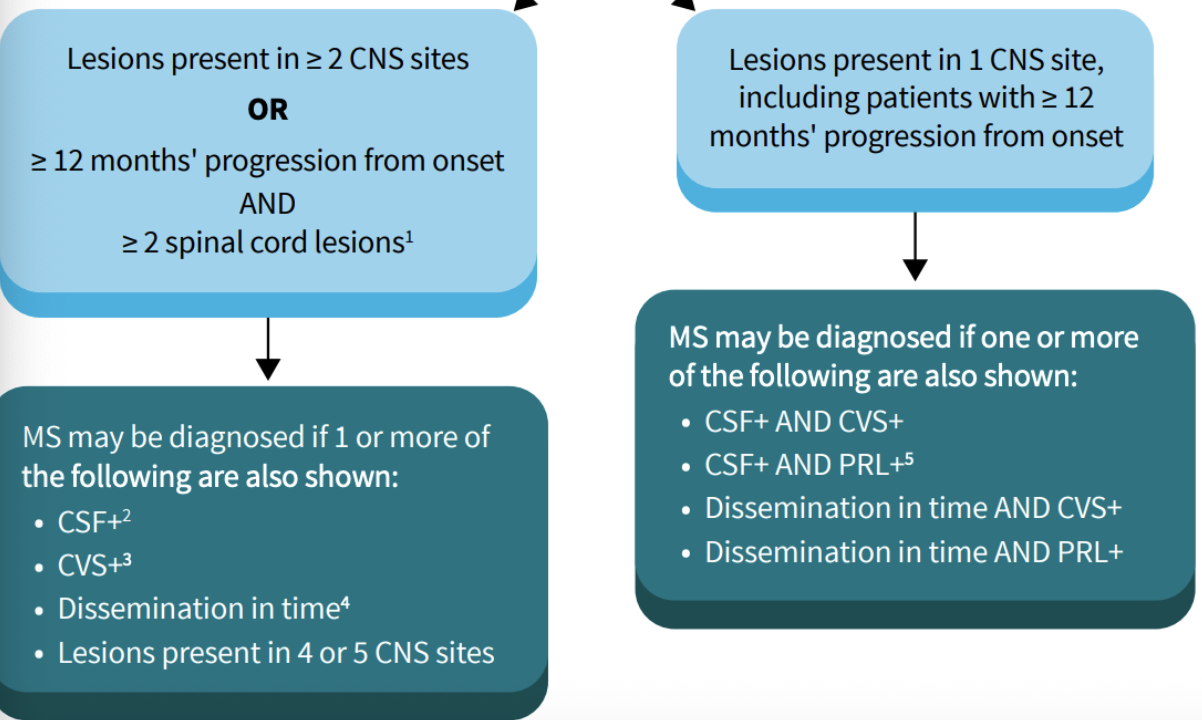
MS McDonald Criteria
+changes
Relation to dissemination in space and time
Changes
optic nerve can serve as fifth anatomical location
dissemination in time (NOT mandatory anymore)
paramagnetic rim lesions by MRI can be used to diagnose in specific situations
addition al recommendation should be considered for confirming diagnosis > 50 years with vascular comorbitiies
hyperlipidemia
diabetes?
MS Imaging and Labs
Imaging
o MRI
Lab
No specific lab tests
CSF evaluation
▪ Oligoclonal bands
▪ Increased IgG
▪ Kappa light chains
Expanded Disability Status Scale (EDSS)
determines disease prognosis for a patient
Disorders that can mimic MS
Lupus
Stroke
Vitamin B12 deficiency
Neoplasms
Syphilis
HIV
Sarcoidosis
Lyme's Disease
Common Phenotypes of MS
Relapse Remitting (RRMS)
most common
Symptom flare ups followed by recovery
However after each attack, recovery becomes less and less
Patient remains stable between attacks
Secondary progressive MS (SPMS)
o Always begins as RRMS
o Experiences progressive deterioration in function unassociated with acute attacks
o Higher amounts of neurologic disability
Primary progressive MS (PPMS)
o ~males more often; diagnosed later on; more serious form
o Patient don’t experience attacks but show a steady decline in function from disease onset
o Usually occurs in patients diagnosed later in life (>40 years old)
Prognosis Factors: MS
+poor, positive
poor
male
older (>40 years) onset
motor, cerebellar, or splinter symptoms at initial presentation
more frequent attacks within first 5 years
postitive
female
younger onset
optic neuritis or sensory symptoms at onset
RRMS
FDA Approved Meds for MS
RRMS/SPMS
Self Injectives
Interferons
Glatiramer Acetate
Ofatumumab
Oral
Teriflunomide
Fumaric Acid Derivatives
PPMS
ocrelizumab
Interferons
+indication, moa, efficacy, agents - admin and pearls
Indications: RRMS, SPMS
Mechanism of Action: Unknown
• Thought to increase suppressor cell function, reduce and downregulate inflammatory markers
• Increase Treg cells
efficacy: moderate
Interferon-beta 1b
SubQ every other day
Interferon-beta 1a
SubQ three times weekly
pearls
prefilled syringe
longer stability in fridge
Pegylated interferon-beta 1a
admin: every 2 weeks (longer t1/2)
IM or SubQ
Bnenefits of interferons - 1a vs 1b
Benefits of Interferon-beta 1b
o Reduced annual relapse rate
o Decreases burden of disease
o No effect on clinical disability
Benefits of interferon-beta 1a
o Reduced annual relapse rates
o no increase in disability
o Reduction in lesions on MRI
Interferon Monitoring and ADEs
+frequency
Depression - all follow up visits
TFTs - q 6 months
CBS, Paltelets, LFTs - baseline, 1 month, q3 months x1 yr, then q 6 months
ADEs
Injection site reactions
Flu like symptoms
Leukopenia
Hepatotoxicity
Shortness of breath
Tachycardia
Anemia
Major Concern with Interferon use in MS
Antibodies that can reduce the effectiveness of the interferon beta therapies
Rates are variable
o close to half of people will develop neutralizing antibodies
o Depends on specific drug and dosing regimen
Glatiramer Acetate
+indication, moa, admin, pearls, benefits
Indications: RRMS, SPMS
Mechanism of Action: Unknown
• Thought to mimic the antigenic properties of myelin proteins --> inhibits binding of T cells
• Increases Th2 cells
Admin:
SubQ QD OR SubQ 3 times/week
Pearls
if using 3 times/week, doses must be separated by at least 48 hours
longer stability when refrigerated
Benefits:
Reductions in mean annual relapse rate
Delays the development of T1 holes on brain MRI
Slows progression of disability in RRMS
Glatiramer ADEs
+BBW
Injection site reactions
immediate post injection site reaction
One time transient reaction after the first dose of glatiramer is given
o Symptoms: chest tightness, flushing, shortness of breath
o Lasts ~20 minutes
o Usually no treatment is needed
Edema
Nausea
Flu like symptoms
Pruritis/skin rash
Infection
BBW: Anaphylactic reaction
Ofatumumab
+indicaitons, moa, admin, pearls, benefits
indications: RRMS, SPSMS
moa: Immunoglobulin antibody that binds to CD20 on B cells resulting in cellular cytolysis and complement mediated lysis
admin: SubQ once weekly x 3 doses THEN q1 month
pearls
should be administered into the abdomen, thigh, or upper arm
stored in refrigerator, first injection should be given in a provider’s office
pre medications can be given prior to injection
benefits
Decreased relapse rate
• Decreased active lesions
• Resulted in fewer new or enlarging lesions
• Slowed disability progression
Ofatumuab: Monitoring and ADEs
+frequency, risks
Hep B - baseline
serum iunoglobulins (IgG, IgM) , CBC, CMP - q 6 months
ADEs
infection s
Hep B reactivation
injection site reactions
Risks - PML
*All live vaccines should be given at least 4 weeks prior to the first dose
Progressive Multifocal Leukpencephalopathy (PML)
+description, symtpoms, treatment
RARE but serious side effect
• Fatal disease of the white matter of the brain caused by a viral infection (JC virus)
o Destroys the white matter of the brain and leads to irreversible axon demyelination
• Symptoms: clumsiness, progressive weakness, visual and speech changes
o In severe cases, personality changes
• Treatment: no treatment available
o Remove the offending agent
Comparison of Self-injected medications
Comparison of interferon beta to glatiramer
Similar clinical efficacy at 24 months
However, at 36 months, one study showed higher relapse rates in the group given interferon
page 51, 52
EDSS
Similar effect on new or enlarging lesions on MRI
Teriflunomide
+indications, moa, amdin, benefits
indications: RMSS, SPMS
Mechanism of Action:
• Inhibits dihydro-orotate dehydrogenase to prevent the proliferation of T and B cells
• Reduces CNS inflammation and demyelination
Admin: qd
Pearls
Inhibits CYP 2C8
Induces CYP 1A2
ADEs: embryofetal toxicity
Benefits:
reduction in relapses
reduction in total lesion volume
reduction in total lesion volume
Teriflunomide: Monitoring and ADEs
+frequency
CBC - baseline, then regular
LFTs - monthly for the first 6 months → every month
Pregnancy - baseline then regularly
ADEs
Alopecia
Headache
Paresthesias
GI Upset
Infection
Leukopenia
Hepatotoxicity
Fumaric Acid Derivatives
+indication, moa, pearls, agents- admin, pearls, benefits
indication: RRMS, SPMS
Mechanism of Action: unknown
Possible anti-inflammatory and cytoprotective properties via nuclear factor pathway
Dimethyl fumarate
maintenance : BID
Diroximel fumarate
maintenance : BID
lower rate of GI upset
Monomethyl fumarate
maintenance : BID
lower rate of GI upset
Benefit so fumaric Acid Derivatives
Reduced annual relapse rates
Reduced number of lesions
Slowed disability progression
Monitoring and ADES: Fumaric Acid Derivates
+risks
CBCs, LFTs → Baseline, then every 6 months for a year, then
annually
ADEs:
Flushing
Pruritus
GI upset
Leukopenia
Elevated LFTs
small risk of PML
Sphigosine 1 - Phosphate Receptor Agonists
+indications, moa, agents - admin, pearls, benefits
-imod
indications: RRMS, SPMS
Mechanism of Action:
• Blocks lymphocytes ability to emerge from lymph nodes, reducing the number of lymphocytes available to cross the blood brain barrier
Benefits - compared to placebo
Decreased relapse rates
New or enlarging lesions reduced over 2 year trial
reduction in 3 month disability progression
Sphigosine 1 - Phosphate Receptor Agonists - NOT DOEN
+agents - admin, pearls, benefits
Agnets
Fingolimod
admin: daily
new ODT formualtion
pearls
pediatrics
• Contraindicated to take with IA or III anti-
arrhythmic
• Good for highly active disease
Siponimod
Ozanimod
Ponesimod
Sphigosine-1-Phosphate Receptor Agonists
+monitoring-freqquecny, ADEs, risks,
CBC, LFTs, EKG - baseline, then regular
Opthaminc exams - anually
ADEs:
First dose bradycardia, AV block
Hypertension
Increased risk of malignancies
Elevated liver enzymes
Macular edema
Infections
small risk of PML
*All live vaccines should be given prior to the first dose of S1P Receptor Agonists
Monitoring: First Dose Bradycardia
+offending agents, parameters
Fingolimod:
Monitored for 6 hours after the first dose is given
Pulse check and blood pressure check every hour
Continuous EKG monitoring
For high risk patients, monitoring can be required overnight
High risk: QTC prolongation, concomitant medications that slow HR, history of MI or heart failure, risk factor for torsade's
Ponesimod
Monitored for 4 hours
Siponimod, ozanimod
Monitoring only required for high risk group
Cladribine
+indications, moa, admin, pearls
indications: RRMs, SPMS
moa: Impairs DNA synthesis --> leading to depletion of B and T lymphocytes
Admin:
2 treatment courses
Initiate first dose anytime, initiate the
2nd dose 23-27 days after
The 2nd course is started 1 year after the first dose is initiated
Pearls
• Maximum lifetime dose is 3.5 mg/kg
• Teratogenic
• Usually saved for patient who have failed other DMTs
Benefits of Cladribine
reduction in relapse rate
remained relapse free after 96 weeks
reduction in new or enlarging T2 lesions
Cladribine: Monitoring and ADEs
+frequency, risk
CBC, LFTs → baseline, ten 3-7 months into tx course
Infection and cancer screening → prior to start of treatment
Pregnancy → baseline, then regularly
ADEs:
Headache
GI upset
Joint pain
Infection
Elevated liver enzymes
Leukopenia
Risk of PML
Alemtuzumab
+indicaiton, moa, admin, pearls
indications: RRMS, SPMS
moa: Humanized monoclonal antibody that targets CD52 which is expressed on T and B lymphocyte
admin: IV infusion
daily x5 days
Then 12 months later, 12 mg IV daily x3
days
pearls:
REMS program -- high monitoring burden
Requires premedication prior to giving infusion
Good for highly active disease
Benfits of Alemtuzumab
reduction in annual relapses
reduction in 6 month disability progression
omitted not stisitclaly significantt
Alemtuzumab: Monitoring and ADEs
+frequency, risk
CBC, LFTs, CMP, UA, TFTs → baseline every 3 months
Infection and cancer screening → prior to start of tx, then regularly
ADEs
Headache
Rash
GI upset
Infusion reactions
Infections (URIs, UTIs)
Immune thrombocytopenia (ITP)
Risk of PML
Ocrelizumab
+indication, moa, admin, pearls
indication: RRMS, SPMS, PPMS
moa:
• Humanized monoclonal antibody that targets CD20 and kills B cells in the immune system
• Prevents B cells from penetrating the blood brain barrier
Admin: IV infusion
day 1 → 2 weeks later →q6months
Pearls
• Humanized monoclonal antibody –-> lower autoantibody formation, infusion reactions
• Requires pre medication prior to infusion
Benefits of Ocrelizumab
reduced relapses
• Compared to interferon-beta 1a
• Reduced new or enlarging lesions
• Compared to interferon-beta 1a
• When studied specifically for PPMS, patient taking ocrelizumab were less likely to have disability progression
compared to placebo
Ocrelizumab: Monitoring and ADEs
+frequency
CBC, LFTs, Serum Immunoglobulins (IgG, IgM) → Baseline, then regularly
Hepatitis B → baseline
ADEs
Infusion reactions
Inections (URIs, skin infections)
Risk of PML
All live vaccines should be given at least 4 weeks prior to the first dose of
ocrelizumab