KINE 3465 Midterm #2
1/150
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
151 Terms
The Viscerocranium VS Neurocranium
Viscerocranium
facial skeleton and bone of the jaw…bones of the face
~14 bone
Neurocranium
protects the brain…they create the cranial cavity
8 bone

How Many Bones Does the Skull have?
22 Bones
The Neurocranium
Frontal bone = makes up our forehead and it articulate with parietal bones (one on either side)
In the back of the skull we have our occipital bone
we have 2 temporal bones and they are associated with where the ears are located
the ethmoid bone is difficult to see because it is situated behind the eyes and it is associated with the Neurocranium but it will contribute to the nasal cavities as well
sphenoid bone runs through the middle of the cranium and this is where we think the temple is

Sutures of the Neurocranium
Sutures: the way in which the Neurocranium is going to fuse
Coronal Suture: connects the frontal and 2 parietal bones
Sagittal Suture: in the sagittal plane… and it fuses the parietal bones together on top of the Neurocranium
Lambdoid Suture: fuses the occipital and parietal bones together
Pterion: is a specific region and it is a location of the weakest point of the skull due to the fact that so many bones articulate here
Calvaria = skull cap

The Cranial Fossae (All 3)
NOTE: in these images the calvaria is removed
the cranial cavity is divided into 3 cranial fossa
1. Anterior Cranial Fossa
Where we see the orbits (where the eyes sit)
mainly comprised of the frontal bone and we have contribution form the ethnic bone
a small portion of sphenoid bone continuities
2. Middle Cranial Fossa
Majority of this cranial fossa comes from sphenoid and temporal bones and on the sides is closed off with the parietal bones
3. Posterior Cranial Fossa
Mainly composed of our occipital bones but we have contributions form the temporal bone and parietal bone

The Brain - All Structures
in the cranial cavity is the brain
The cerebrum is going to be the top of the brain and we have right and left sides
gyru = bump
sulcus = fold
Lobes of the brain:
Frontal = anterior cranial fossa
Parietal = Not in a fossa
Occipital = posterior cranial fossa
Temporal = middle cranial fossa
Cerebellum = important for balance
Brain Stem: 3 Components
mid Brian = closest to the cerebrum
pons
medulla oblongata = leads into cervical segments of the spinal cord
Corpus Callosum = connection between right and left hemisphere and a way in which they can communicate

The brain and the Meninges - Mater layers
dura mater = outside layer
pia mater = hugs spinal cord or brain
arachnoid mater= between the dura mater and the pia mater
Between the arachnoid mater and the pia mater is our subarachnoid space where we find cerebrospinal fluid
the dura mater creates folds around the brian

The brain and the Meninges - The Falx Cerebri
The Falx Cerebri is creating a division between right and left hemispheres within the cranial cavity
The brain and the Meninges - The Tentorium
The Tentorium Cerebelli is fold of the dura mater and it creates a tent over the top of the cerebellum…separating the cerebellum right from left cerebral hemispheres
The brain and the Meninges - Dural Venous Sinuses
Dural Venous Sinuses = part of venous drainage for the brain. We have aspects of the cerebrospinal fluid where we want to regulate the cerebrospinal fluid that surround the brain that gives it it’s buoyancy and we want the Brian to be buoyant because the brain is heavy
parts of the subarachnoid space dumps cerebrospinal fluid in to these dural venous sinuses
The Brain and the Meninges - Summary

The Anterior Cranial Fossa
frontal bone is majority of the anterior cranial fossa and we see the orbits which is the bonney socket where our eyeballs sits
in between our eyes we have the ethmoid bone and it contributes to the medial orbit plate (contributes to the orbit) and it also contributes to the nasal cavity
part of the ethmoid bone is called the cribriform form plate which has pin like opening called the cribriform foramina

Sphenoid Bone - Anterior and Middle Fossa
the sphenoid bone looks like a bat or butler fly and it has 2 wings
lesser sphenoid wing: contributes to the anterior cranial fossa
greater sphenoid wing: contributes to middle cranial fossa
and in between on either side of the wings we have a central body where we have the hypophyseal fossa where the pituitary gland is going to sit (part of our endocrine system)
within the lesser sphenoid wings we have the optic canal (2 -right and left) which allows for nerves to get to our orbits and stretch towards the eye
we also have the superior orbital fissure which separates the lesser and greater sphenoid wings (lesser sits on top of the greater sphenoid wing) and it also is a hole that allows nerve to travel through to target the eye


anterior view we see the central body of the sphenoid bone
we have portions of the sphenoid bone contributing to the orbit
when we come down from the sphenoid wing we see the pterygoid processes and this splits and gives rise to lateral and medial pterygoid plates which brioche important for other attachments later on
Middle and Posterior Cranial Fossae
Temporal bone has 2/3 components
squamous portion: squamous means flat and thin and is there to protects the brain
petrous portion: petrous means rockey and is thicker and separates the middle and the posterior cranial fossa and houses part of our ear as well (holds middle and inner ear)
tympanic portion: where it opens up into part of the ear…its opening is called the external acoustic meatus (the external ear)
posterior cranial fossa
has a big opening in the occipital bone called the foramen magnum which is a opening for the spinal cord
cerebellar fossa on the inside of the occipital one are for the cerebellar aspects to sit in (sits on right and left sides)

The Cranial Foramina

in the anterior cranial foams we see the cribriform plate with the cribriform foramina and the nerves that pass through the cribriform foramina target the nasal cavity
in the middle cranial fossa
the optic canal can be considered part of the anterior and middle cranial fossa…but the optic canal is seen in the lesser sphenoid wing which moves into the orbit
part of the great sphenoid wing are additional holes
foramen rotundum = round hole
foramen ovale = ovale hole
foramen spinosum = tiny hole…holds the middle meningeal artery which is a artery that provides the primary blood supply to the meninges of the brain
Acronym: ROS with R starting more superior and medial and then they work their way down and laterally
SOF (superior orbital fissure) opening in the middle cranial fossa
we see the internal acoustic meatus which leads us into the internal ear and this opening is specific in the petrous portion of the bone…un death this we have a bigger opening called the jugular foramen and that is because the internal jugular vein passes through here which is the primary vein that brain venous blood from the brain…
***all the dural venous sinuses are all going to eventually dump the blood into the internal jugular vein and that goes down through the neck, then into the subclavian veins to the brachiocephalic vein
an open on either side of the foramen magnum is called the hypoglossal Canal (glossal = tongue) and this canal is specific for a cranial nerves to innervate the tongue

The Base of the Skull

posterior view of the skull
In the temporal bone we have a opening for the carotid canal which is for the internal carotid artery to go from the neck into the cranial cavity and it is responsible for bringing blood to the brain..the carotid artery travels medially and anteriorly within this canal (come in bend 90 degrees travel in the canal and bends again to go up)…the foramen lacerum is for when the carotid artery bends the second time it gives it space to bend [internal carotid artery end 90 degrees twice]
Styloid process and mastoid process are places for attachment and in between we have a opening on the base of the skull that is NOT in a cranial cavity called the stylomastoid foramen
The Viscerocranium
viscerocranium are the bones of our face and it is made of approximately 14 bones and we say approximately because there is one controversial bone
our nasal bone (where our sunglasses sit) this is 2 bones (right and left sides)
on the medial side of the orbit the bone is called the lacrimal bones and it houses the tear ducts because tear are produced lacteal sacs
upper jaw is the maxilla and it is 2 bones fused together along the midline
the volmer is one bone associated with the nasal cavity specifically the nasal septum
***inferior nasal conchae is the controversial bone and they help while we breathe air into our nose career a turbulent flow in the nose to help heat up the air in term of moisture
we have 3 membranes inside the nasal cavity
superior and middle come from the ethmoid bone
The inferior is controversial because some say it's a extension off the maxilla others say it is its own bone
Zygomatic bones are our cheekbones and we have 2 right and left
on the base of the skull we have palatine bones and they are associated with the maxilla and they form the posterior bit of our hard palate
the mandible is one bone and it has to attach to the rest of the skull

The Zygomatic Arch
zygomatic bone is our check bone and if we pinch it on pour face there is a space below and a space above and that is our zygomatic arch and there is a opening that allows for passing of muscles and neurovascular structures along the side of the face and neck
the zygomatic arch is formed by the fusion of 2 bones the a process form the zygomatic bone and a process from the temporal bone

The Mandible
the rounded bit is called the head/condyle of the mandible and it has a coronoid process and in between we have the mandibular notch
the ramus of the mandible and that lead us into the 90 degree bend coming forward (also the angel of the mandible)..the portion that actually comes forward is the body
we have a mental protuberance which contributes to your chin (mental = chin) and on other side of the mental protuberance we have a mental foramen (right and left) and that is for particular arteries and nerves to exit the mandible and provide innervation to blood supply in the face
with respect to the jaw we have alveolar processes which are out bumps that the teeth sit within
the mandible has a unique attachment called the temporomandibular joint (located just in front of your ear, put your hands here and open and close your mouth)[TMJ joint]

The Cranial Nerves (CN) + Type of Innervations
12 pairs of cranial nerves (12 on the right, 12 on the left)
cranial nerves are located on the base of the brain or brainstem….the types of cranial nerves are general somatic, general visceral, special visceral, special somatic
touch is a special sense but it is more visceral somatic
General somatic: sensory innervation to skeletal muscle and skin
General Visceral: sensory information to internal organs or motor internal control to organs
Special Somatic: associated with motor pathways like vision, hearing, and balance, and touch
Special Visceral: associated with motor pathways like tase and smell

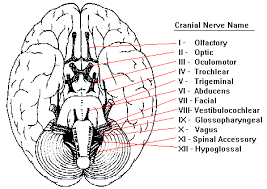
The 12 Cranial Nerves
Cranial Nerve l & ll - The False Cranial Nerves
cranial nerves 1(l) and 2 (ll) are considered false cranial nerves sand they are considered false because they are extension of tissues coming off the base of the brain
cranial nerve l is our olfactory nerve and it provides our special sense of smell
cranial nerve ll is our optic nerves and it provides our special sense of sight

Cranial Nerve lll to Xll are Associated with the Brain Stem
the other cranial nerves (3- 12) are true cranial nerves because they are directly associated with the brainstem
where the mid brian hits the pons is where cranial nerve 3 is
cranial nerve 4 and 5 are on either side wrapping around the pons
cranial nerve 6 is at the centre of the bottom of the pons at the pontomedullary junction
Cranial nerves 7,8 they are located more at the pontomedullary junction
alongside the medulla oblongata are cranial nerve 9,10 and 11
up towards the anterior center of the medulla oblongata we see cranial nerve 12

The Brainstem Cranial Nerve Orientation

cranial nerve 4 actually starts on the posterior side of the brain stem and it wraps around to the front (only peaks out on the anterior side)
cranial nerve 5 is big and it looks like there is 2 of them and that is because it has a big sensory component and a small motor component (big sensory root and small motor root)
cranial nerve 6 is along the midline at the pontomedullary junction
cranial; nerve 12 is along the midline of the medulla oblongata
parts of cranial nerve 11 come from the segments of the upper spinal cord and the medulla oblongata
nerves at the midline are 1,2,3,6,12
Cranial Nerve l - The Olfactory Nerve

What is truly cranial nerve 1 if all the nerve fibres travelling through the cribriform plate of the ethmoid bone and the cribriform foramina is for cranial nerve 1 to pass through and entered into the top of our nasal cavities
the olfactory bulb sits inside the cranial cavity on the cribriform plate and the nerve fibres extending from the olfactory bulb is going to the nasal cavity and provides us with our sense of smell
attached to the olfactory bulb is the olfactory tract which then leads signals to the brain that are responsible for sensing smell

in the nasal cavity we have a mucus membrane which has cilia for specific receptors that are responsible for sensing a specific odorant molecules…the cilia are attached to sensory receptors…the odorant molecules are going to bind to the olfactory receptors on the cilia of the neuron and the olfactory neurons are all going to the brain and travel through the cribriform plate and foramina and come up to the olfactory bulb where the nervous structure called glomeruli (glomerulus) and this is where we organise this information and then the information gets sent to regions of the brain associated with olfaction through the olfactory tract
The olfactory nerve is one of the only nerves associated with memory (e.g. ‘this smell reminds me of…”
Cranial Nerve ll - The Optic Nerve

the optic nerve goes to the eyeball and is going to detect vision and is our sense of sight and it travel to the centre back of the eyeball and gets there by travelling through the optic canal (in lesser wing of the sphenoid wing)..the optic chiasm we get the optic tract and the optic tract carries the nerve impulses back to the regions of the brain responsible for vision which is associated with the occipital lobe
the pituitary gland sits right where the optic chiasm is located….if we have any sporty of enlargement in the pituitary gland it can impinge on the optic chiasm and affect their vision
in one eye back it gets divided and sorted into right and left visual fields…and then the left visual field goes to the right side of the brain and the right visual field goes to the left side of the brain (contralateral association)
only some of the visual field cross at the chiasm sometimes it doesn't cross…if you take the right eye it has both right and left visual fields but only the right visual field would cross at the chiasm and the left visual field will stay and use the optic nerve to stay and go to the right side if the brain

Extraocular Muscles - Movement of the Eye - Axis
we have 2 axis when we look a t muscles of the eye
axis of the orbit: the eyes sit on a angle (trace medially and posteriorly)[diagonal]
optical axis: from the front to the back of the eye
these 2 axis do not line up…IF they did then our pupils would face outwards
*when talking about the muscles that move the eye (Extraocular muscles) they line up with the orbital axis
the insertion of these eyeball ball muscles is ALWAY the eyeball itself because it is the movable structure while the origin should be stationary
most of our Extraocular muscle originate at the common tendinous ring and this is also called the Annulus of Zinn and all muscles of the eye originate here EXCEPT for one
the optic nerve passes through the Annulus of Zinn

Extraocular Muscles - Movement of the Eye - Levator Palpebrae
levator palpebrae starts in the annulus of Zinn BUT it doesn't connect to the eyeball it connects to the eyelid and it is responsible for elevation of the upper (superior) eyelid

Extraocular Muscles - Movement of the Eye - Rectus Muscles
Rectus = (in reference to the eye) means it pulls in a straight fashion (unlike the oblique muscles which we get into later)
When the Rectus eye muscles attach to the eyeball they always attach to the anterior half of the eyeball
medial Rectus and lateral Rectus muscles are responsible for adduction and abduction of the eye…
medial Rectus: adduction (brings eye to look toward midline)
lateral Rectus: abduction (brings eye to look laterally)
and they work in opposition when taking BOTH eyes and look to the right
the superior Rectus are elevating the eye AND pulling it medial and this rotation is called intorsion
elevation and intorsion
the inferior Rectus pulls the eye downward and pulls it posteromedial and it is a extortion
Depression and extortion



Extraocular Muscles - Movement of the Eye - Oblique Muscles

both the oblique eye muscles run in a diagonal fashion and they insert onto the posterior half of the eyeball
The superior oblique is on the top (superior) on the lateral side of the back half of the eyeball and it runs through a sling called the trochlea which is made of connective tissue which allows for a sling mechanism…and it pulls the eye down (pulls on the back of eye forward) and it pulls it medially (intorsion)
superior is always intorsion same as with superior rectus
The inferior oblique as its own separate origin in the orbit and it originates on the medial side of the orbit in the orbit socket and go to attach to the lateral side on the posterior side of the eyeball inferiorly…this causes elevation of the eye and extortion
inferior is always extortion same as with the inferior rectus
Anatomical Pull of the Extraocular Muscles

Cranial Nerves - lll, lV, Vl

cranial nerve that provide motor innervation to Extraocular muscles are cranial nerves 3(lll) ,4(lV) ,6(Vl)
oculomotor nerve is cranial nerve 3 and provide MOST if the innervation…to superior, medial, and inferior rectus, plus inferior oblique muscles and levator palpebrae
Cranial nerve 4 (trochlear nerve) supplies innervation to superior oblique
because the superior oblique goes through the trochlea
cranial nerve 6 (abducens nerve) innervates lateral rectus
Lateral rectus allows for Abduction
For the nerve to leave from the brainstem and exit the cranial cavity by traveling through the superior orbital fissure (slit between the lesser and greater wing)[cranial nerve 3,4,6]
the oculomotor nerve (cranial nerve 3) is assorted with the ciliary ganglion and that sits on the lateral side of the eyeball and this ganglion is a parasympathetic ganglion….this means that in addition to being a somatic motor nerve it is also a parasympathetic cranial nerve

Cranial Nerve lll - Oculomotor Carries Parasympathetic Innervation
when you look at the parasympathetic innervation we look at changing the shape and size of the pupil
we have 2 muscle in the iris
dilator pupillae: in a longitudinal axis and it take the iris and pull it out
during dim light to allow more light to come into the eye
sphincter pupillae: in the concentric ring and it contracts
during bright light to limit how much light comes into the eye
cranial nerve 3 parasympathetic contracts the pupil
Cranial nerve 3 sympathetic comes from T1 to T4 and allows dilation

Practice Question: Injury to which of the following cranial nerves below would result in the deficiency seen in the patient image below?

A. CN II – optic n.
optic nerve ONLY supply’s us with vision NOTHING motor
B. CN III – oculomotor n.
1. Cant look medially
2. Cant lift the eyelid
C. CN IV – trochlear n.
D. CN VI – abducens
How Do We Test for Muscle or Nerve Damage?

even when we have a neutral gaze all the muscles of the eye have some sort of natural tension on the eye
medial and lateral rectus are the only muscles the provide TRUE abduction and adduction and so by looking either right or left we are testing they muscles and cranial nerve associated
Breakdown of the H-Test - Superior Rectus and Inferior Oblique

we have 2 elevators (superior rectus and inferior oblique) and to test these since they have a shared function we need to align the optical axis with the vector pull of the muscle and once we do that it eliminates the other muscle
remember we have two axis of the eyes and the arrows on the muscles is the vector pull of that muscle (the way in which the muscle pulls on the eye)
Superior rectus:
to get the them in line you need to look laterally (abduct) and then after that you elevate the eye since the muscle os a elevator
Inferior Oblique:
To get them in line you need to look in (adduction)[medially] and since the muscle is a elevator you look up
Breakdown of the H-Test - Inferior Rectus and Superior Oblique

Inferior Rectus:
Abduction and looking down
Superior Oblique:
Has a pulley system with the trochlea but we still want to adduct (medially) and look down
Summary of the H-Test

Cranial Nerve V - Trigeminal Nerve

cranial nerve 5
Big nerve in the pons and has a small motor root and a big sensory root so it innervates both for sensory and motor but mainly sensory
Branches of Cranial Nerve 5
Since this nerve is so large it has 3 components to it
V1 = ophthalmic nerve
goes toward the orbit then up to the forehead
exits the cranial cavity through the superior orbital fissure and comes up through the superior portion of the orbit and come up along the forehead and provides general sensory information
V2 = maxillary nerve
Going to exit the cranial cavity through the foramen rotundum and then exits the infraorbital foramen (inferior to the orbit) and then come up and give general sensory to the face
V3 = Mandibular nerve
Exits the cranial cavity through the foramen ovale and comes down toward the mandible to provide sensory innervation to the face and the motor innervation to muscles of mastication (chewing)
Cranial Nerve V1 - Ophthalmic Nerve - 2 Branches
V1 goes through superior orbital fissure and it branches off into multiple branches and one is called the frontal nerve that nerve goes up to the frontal bone/forehead and it is going to exit through the supraorbital foramen and goes to the forehead and now these branches are now called supraorbital
We also have the lacrimal nerve going to the lacrimal gland on the lateral side of the eyeball responsible for tear production…provides sensory innervation to the lacrimal gland
*everything form the ear forward (in terms of the head) is cranial nerve innervation…everything behind is other spinal levels and periphery nerves

Cranial V2 - Maxillary Nerve - 2 Branches
one of the branches of V2 is called the infraorbital nerve and travels through bones of the maxilla and it exits through infraorbital foramen and it provides sensation to the cheek (blue shading)
Another branch of V2 is the superior alveolar nerves (multiple) and alveolar refers to the teeth so therefore upper teeth…so the superior alveolar nerve travels through the maxilla to provide sensory innervation to the upper teeth
*V2 also provides sensation to the rest of the nasal cavity that does NOT get sensation from V1

Cranial Nerve V3 - Mandibular Nerve - 2 Nerves
exits the skull via foramen ovale and quickly branches a lot
the lingual nerve goes towards the tongue and provides general sensory information to the anterior ⅔ of the tongue
general sensation: pain, touch, heat/cold
inferior alveolar nerve travels through the mandible and provides general sensory information to the mandibular teeth (lower teeth)…after it goes from the teeth it exits the skull through the mental foramen (on either side of the chin) and it provides general sensory information to the lower lip

Summary of V1, V2, and V3 Branches
V1 = Ophthalmic nerve
Frontal nerve
lacrimal nerve
V2 = Maxillary Nerve
superior alveolar nerve
infraorbital nerve
V3 = Mandibular Nerve
inferior alveolar nereve
lingual nerve
Cranial Nerve Vll - Facial Nerve

cranial nerve 7 is the facial nerve and it comes from the ponsomedullary junction and it supplies motor to muscles of facial expression and it also gives off a branch called the chorda tympani that also targets the anterior ⅔ of the tongue but provides special sensory innervation (taste)….we also see the facial nerve also provides parasympathetic innervation specifically to salivary glands…we also get parasympathetic innervation to the lacrimal, nasal, palatal glands
the facial nerve leaves the cranial cavity through the internal acoustic meatus… within this middle ear there is a facial canal (in temporal bone) and it's called this because the facial nerve travels through this canal…because it travels through the ear and it needs to leave the skull it's going to leave the skull through stylomastoid foremen

Cranial Nerve Vlll - Vestibulocochlear Nerve

Cranial nerve has two names
we use vestibulocochlear nerve
some say auditory nerve
targets aspects of the inner ear
exits the cranial cavity through internal acoustic meatus and because it interact with the ear it never fully leaves the skull, just leaves the cranial cavity but stays within the temporal bone
2 component of the inner ear is called the vestibular apparatus which a responsible for balance and vestibular cochlear has 2 braches cochlea branch (goes to cochlea in the ear for hearing) and vestibular branch
vestibulocochlear nerve provides special sensory information for hearing and balance
Cranial Nerve lX - Glossopharyngeal Nerve

Gloso = tongue
cranial nerve 9 exits the skull through the jugular foramen and it give parasympathetic innervation to the parotid gland which sits right in front of the ear and the Otic ganglion sits next to the parotid gland
it also gives general and special sensory to the posterior ⅓ of the tongue
it also has sensory and muscles innervation to muscles of the pharynx
it also has sensory to the carotid body which is a small area where the common carotid artery splits into internal and external branches
Cranial Nerve X - Vagus Nerve

We already know the vagus know does 90% of our parasympathetic innervation to the heart, lung, and esophagus
When the vagus nerve wants to exit the cranial cavity in the skull it does so through the jugular foramen
***It also give gernal sensory information to the larynx and the branch of vagus nerve now called the recurrent laryngeal nerve innervates the muscles that move the vocal cords (supplies motor innervation)
Cranial Nerve Xl - Spinal Accessory Nerve

cranial nerve 11 exits the skull through the jugular foremen
This nerve is called spinal accessory because it has a cranial root which come directly off the brainstem and it has a spinal root that ascends up the through this foramen magnum join up with the cranial root and then merge with the spinal root to for form the spinal accessory nerve
it only provides motor innervation to muscles like the sternocleidomastoid and the trapezius
cranial nerves 9, 10 , and 11 and the internal jugular vein leave through the jugular foramen
Cranial nerve Xll - Hypoglossal Nerve

cranial nerve 12
it is a motor nerve that goes to the muscles that move the tongue for both intrinsic and extrinsic muscles
the right side of the tongue is controlled by the left side of our brain and vice versa
Summary of Cranial Nerves

the imagine on the right has the deramature tissue on it on the left side imagine it is removed
cranial nerve 1 = cribriform plate and cribriform foramina
cranial nerve 2 = optic canal
Cranial nerve 3,4, 6, V1 = superior orbital fissure
cranial nerve V2 = foramen rotundum
criminal nerve V3 = foramen ovale
cranial nerve 7 and 8 = internal acoustic meatus
cranial nerve exit the skull = stylomastoid foramen
cranial nerve 8 = doesn't leave the skull cause it goes to the ear
Cranial nerve 12 = hypoglossal canal
What Cranial Nerve makes Two 90 Degree Bends?
The nerve that makes two 90-degree bends is the abducens nerve (cranial nerve VI)
Cranial Nerve Acronym

this does NOT include parasympathetic
Summary of Parasympathetic Innervation

”Simplified” Overview of Some Cranial Nerve Testing

Olfactory = plug either side of nasal cavity and see if there's a difference in the strength of the smell
optic = letter and colour testing
Nerves that move the eye = H-Test
Trigeminal nerve = swabbing stuff on the forehead and check and have the patient close their eyes
Facial = asking people make faces

vestibulocochlear = rapid head movements, thinning forks to test different types of hearing
glossopharyngeal nerve = test gag reflex by using a tongue depressor
vagus = same assessment at nerve above
spinal accessory = resist shoulder shrug and cervical rotation
hypoglossal = can you stick your tongue out and move it in all directions (extrinsic), to test intricate muscle of the tongue you have them make shapes with their tongue
Muscles of Facial Expression - Brief Overview

Muscles of facial expression they are thin muscle in the face and they originate on the bone and insert into the skin to move the skin
Primary function of muscles of facial expression has a protection nature
E.g. something flying at your eyes you will have a reflex to close your eyes
Secondary function is to modify the expression of the face
Muscles of Facial Expression - Orbital Group
occipitofrontalis
orbicularis oculi (2 portions)
orbital portion
palpebral portion
Muscles of Facial Expression - Orbital Group - Occipitofrontalis

Muscles → Occipitofrontalis has 2 parts
Frontal belly portion is going to be muscles on the frontal bone and insert onto the skin of the forehead…associated with skin on the forehead and the top of the eyebrows
Occipital belly is on the occipital bone and it draws the scalp (skin of skull) posteriorly
They connect and work together through the epicranial aponeurosis which is a thick broad tendon that attaches the 2 bellies together
Muscles of Facial Expression - Orbital Group - Orbicularis Oculi

Muscles → Orbicularis Oculi has 2 portions
Orbital Portion which wants to orbit the eye..concentric rings around the eye that act as a sphincter that is involved in forceful closure of the eye
Palpebral portion is more so with respect to the eyelids… has muscle fibers that run transversely/horizontally across the upper and lower eyelid and this more so for blinking (involuntary closure of the eyelid, voluntary sleeping)
Muscles of Facial Expression - Orbital and Nasal Groups - Summary
Depressor Supercilii
Corrugator Supercilii
Procerus
Nasalis
Levator Labii Superioris Alaeque Nasi
Muscles of Facial Expression - Orbital and Nasal Groups - Depressor Supercilii
On The medial side of eyebrows and it wants to hold the eyebrows down…creates wrinkling between the 2 eyebrows

Muscles of Facial Expression - Orbital and Nasal Groups - Corrugator Supercilii
Deep to the frontal belly of occipitofrontalis and slightly deep to depressor supercilii
It wants to shorten the eyebrows (e.g. furrowing)...pulls eyebrows medially and slightly inferiorly
Works with depressor supercilii to get the full scrunching of the eyebrow
Muscles of Facial Expression - Orbital and Nasal Groups - Procerus
Right in the middle between the 2 eyebrows
Takes medial side of the eyebrows and pulls them medially and inferiorly and is responsible for scrunching the eyebrows together while scrunching the nose with it
Muscles of Facial Expression - Orbital and Nasal Groups - Nasalis
On the top of the nose on right and left that meet medially
Allows for flaring of nostrils and scrunching of the nose
Muscles of Facial Expression - Orbital and Nasal Groups - Levator Labii Superioris Alaeque Nasi
Elevates upper lip
Insert into skin just above upper lip
Is along the wings of the nose
Also involves in flaring of nostrils
Increase nasolabial furrow (smile line)
Muscles of Facial Expression - Oral Group - Summary
Orbicularis Oris
Levator Labii Superioris
Levator Anguli Oris
Zygomaticus Major
Zygomaticus Minor
Depressor Anguli Oris
Depressor Labii Inferioris
Mentalis
Risorius
Platysma
Buccinator
Muscles of Facial Expression - Oral Group - Orbicularis Oris
Orbicularis Oris
Concentric rings (right and left meet at midline of upper and lower lip → ‘C’ shaped)
Acts as oral sphincter -> compression of mouth and protrusion of the lips

Muscles of Facial Expression - Oral Group - Levator Labii Superioris
Levator Labii Superioris
Elevates the upper lip
Inserts onto skin of upper lip
Muscles of Facial Expression - Oral Group - Levator Anguli Oris
Levator Anguli Oris
Elevate the corner of the mouth
Inserts onto the corner/skin of the mouth
Assists in smiling
Muscles of Facial Expression - Oral Group - Zygomaticus Major & Minor
Zygomaticus Major
Inferior to minor
Inserts onto the angle of the mouth and wants to draw it up and lateral
Assists in smiling
Zygomaticus Minor
Superior to major
Inserts towards the midline of the upper lip
Elevation and lateral retraction of the upper lip

Muscles of Facial Expression - Oral Group - Depressor Anguli Oris
Depressor Anguli Oris
Pulls the corners of the lip down/inferiorly
Assists in frowning

Muscles of Facial Expression - Oral Group - Depressor Labii Inferioris
Depressor Labii Inferioris
Pulls lower lip inferior/downward
More medial than depressor anguli oris which makes sense because depressor anguli oris would insert at the corners of the mouth
Muscles of Facial Expression - Oral Group - Mentalis
Mentalis
Elevates and protrudes the lower lip
Draws skin up and over
E.g. think puppy dog face or pouting
Muscles of Facial Expression - Oral Group - Risorius
Risorius
Controversial muscles…some people think it is its own muscle others think its a extension of another bigger muscles
Attaches to the corners of the mouth and it creates our ‘fake smile’...take corners of the mouth and pulls them directly laterally

Muscles of Facial Expression - Oral Group - Platysma
Platysma
A muscle of facial expression that also comes down into the neck and it is very thin and superficial as it sits in the subcutaneous layer of the neck
Can get lost during dissection when the individual has lost subcutaneous fat
Take the sin along the lower face and draw it downward which also ultimately results is a lateral drawing of the corners of the mouth which is why it is closely associated with risorius which is also why some say risorius is part of platysma but we have individual control over each (e.g. think about make the 2 different faces)
Muscles of Facial Expression - Oral Group - Buccinator
Buccinator
Deep muscle directly in the cheek
Take the fleshly portions of the cheeks and tries to draw it toward the molar teeth
E.g. thinking of sucking
Works with orbicularis oris to perform resistion of distension of the cheeks (eg puffing your cheeks out, chipmunk face)
Good if you play a windpipe instrument
Over top of this muscle we have a buccinator fat pad and the size of the fat pad changes the size/shape of your face/cheek
Parotid (Stenson’s) Duct
The Parotid gland sits just in front of our ears and this gland produces saliva since it is a salivary gland therefore it has a opening/duct called the Parotid (Stenson’s) Duct to get saliva into the oral cavity since this gland sits outside of the oral cavity…and this gland has to pierce through the buccinator muscle and when it opens up inside the oral cavity ti opens opposite of the 2nd maxillary molar (on the top jaw, on labial side of molar 2)

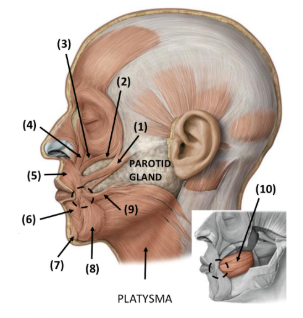
Label Image:

Motor Innervation to the Face - Cranial Nerve Vll

Facial nerve (cranial nerve 7) is responsible for innervation of muscle of the face for motor innervation and it exits the skull through the stylomastoid foramen and exits the cranial cavity through the internal acoustic medus…after it leaves the stylomastoid foramen is splits a lot and it pierces through the parotid gland and then branches to areas of the face and there is looping within these branches which shows us that the muscles of facial expression do not work in isolation they always work as groups
The branching of the facial nerve there are 5 branches
Note: to remember the branching take right hand bring it over to your left ear reaching posteriorly with thumb down

NOTE: we do NOT need to know all the muscles that each branch goes to we just need to know that some branches of the facial nerve innervate more than one muscle proving that muscles work in groups/pairs
Bell’s Palsy

Bell's Palsy is a partial or total paralysis and this is often temporary and that due to some form of paralysis to the facial nerve (CN Vll)
Symptoms
Dry eyes because we can’t voluntary causes our eyes
Dropping of the eye
Loss of muscle tone in the cheek (usually do to buccinator no longer pulling the cheeks inward to the molar teeth)
Dropping of corner of the mouth

Upper half of the face goes to the ipsilateral and contralateral side of the brain (goes to both sides of the brain)
Lower half of the face goes to the contralateral side of the brain (opposite side of the brain)
Left Image: Lesion in the cranial nerve once it leaves the brain stem
Affects all aspects that affect either the lower or upper half of the face
Right Image: Lesion in the brain stem
E.g. if the lesion was on the left side of the brain it would affect the ride side of the lower face
Sensory Innervation to the Face - Cranial Nerve V

Cranial Nerve 5 = Trigeminal Nerve (big sensory, small motor component)
V1 = Ophthalmic Nerve
V2 = Maxillary Nerve
V3 = Mandibular Nerve

V1= sensory innervation to the forehead, upper eyelids,and along the bridge of the nose
V2 = sensory innervation to the lower eyelids, cheek, and upper lip
V3 = sensory innervation to the lower lip, chin, and in front of the ear
Infraorbital nerve come out of the infraorbital foramen just below the orbit coming from V2
Inferior Alveolar Nerve is a branch of V3 going into the mandible itself and provides sensory innervation to the mandibular teeth and it comes out of the skull at the mental foramen and then becomes the mental nerve of V3
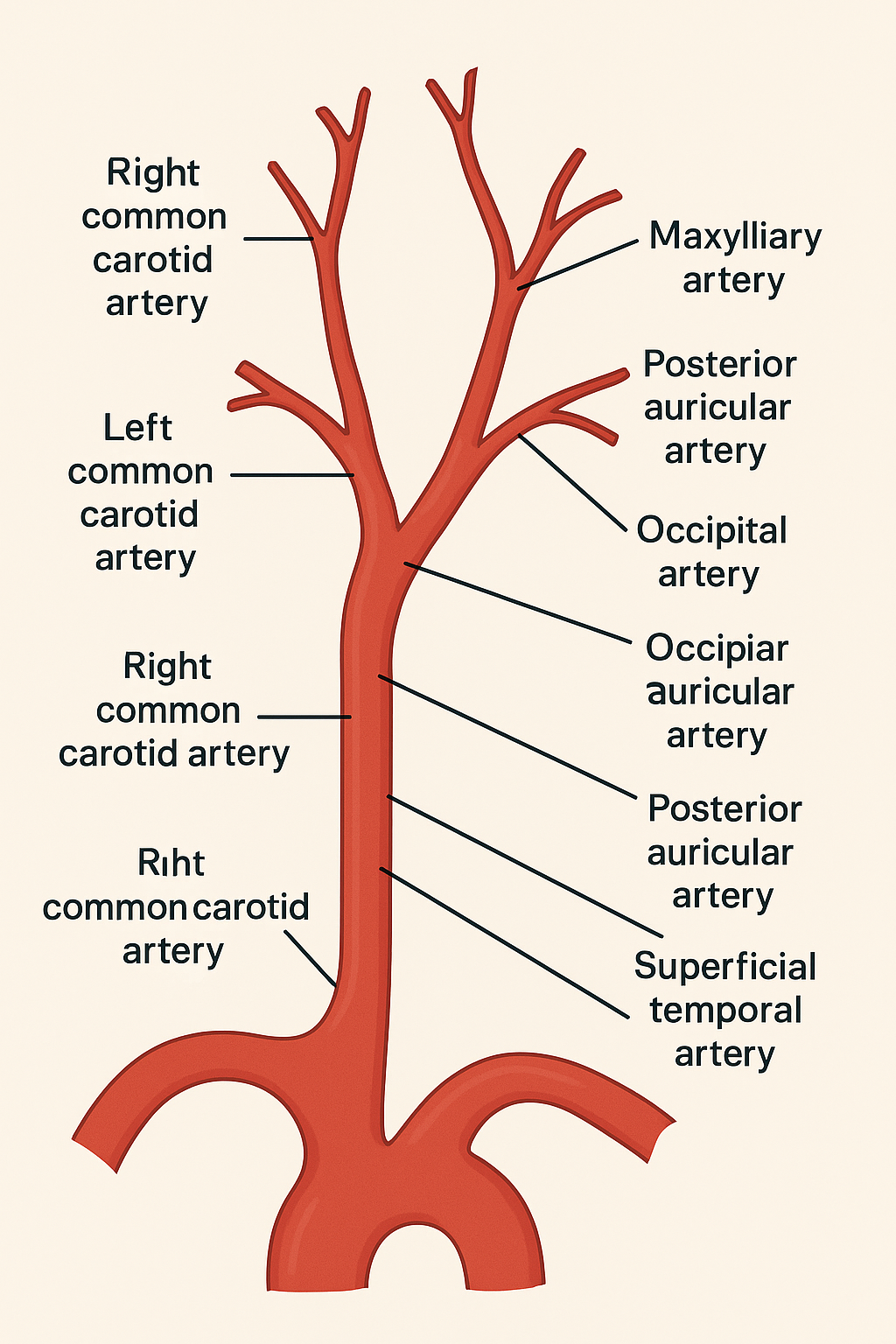
Branches of External Carotid Artery

The common carotid artery comes off the arch often aorta (R comes from brachiocephalic trunk, L is its own branch on the arch of the aorta)...he common carotid artery bifurcates around the 4th rib (occasionally the 5th defending on anatomical difference) and it splits into 2 arteries being the internal and external carotid arteries
The first branch off the external carotid artery is the superior thyroid artery and it goes into the neck to go to the top of the thyroid gland
Our external carotid artery ends as our superficial temporal artery
The second branch we get is the lingual artery (lingual - tongue) which provides blood supply to the tongue
The third branch we get is the facial artery and it targets the face and you can find a facial pulse there (clench your draw. Place fingers on the edge of the mandible to feel the pulse)
The fourth branch is the occipital artery which goes posteriorly to the occipital bone
The fifth branch is the posterior auricular artery which goes behind the ear (behind the external acoustic meatus)
The sixth branch is the maxillary artery
The superficial temporal artery has tonnes of branches along the lateral side of the head
Summary of Branching for External Carotid Artery
1. Origin of Common Carotid Arteries:
Right common carotid artery branches from the brachiocephalic trunk.
Left common carotid artery branches directly from the arch of the aorta.
2. Bifurcation of the Common Carotid Artery:
Occurs around the level of the 4th cervical vertebra (C4) (near the upper border of the thyroid cartilage or around the 4th rib depending on anatomical variation).
Splits into:
Internal carotid artery (goes to the brain, no branches in the neck).
External carotid artery (supplies face, neck, scalp).
3. Branches of the External Carotid Artery (in order):
Superior thyroid artery – goes to the top of the thyroid gland.
Lingual artery – supplies the tongue.
Facial artery – supplies the face; palpable at the mandibular edge.
Occipital artery – goes posteriorly to the occipital bone.
Posterior auricular artery – goes behind the ear (posterior to the external acoustic meatus).
Maxillary artery – large terminal branch that supplies deep facial structures.
Superficial temporal artery – final branch; continues upward and gives many branches along the lateral side of the head.
Blood Supply to the Face - Facial Artery

The facial artery comes up alongside/margin of the mandible and ascend along the side of our face and it first gives off a submental artery that goes underneath the chin…then we have other branches that come off the facial artery that go to the lips like the inferior labial artery (lower lip) and the superior labial artery (goes to upper lip)...then the facial artery continues to go up and once it get to the side of the nose it changes names to angular artery and then some of these branches off the angular artery will go to the orbit and cheek
The lateral nasal artery goes off the lateral side of the nose and target the cheek
Blood Supply to the Face - 2 Main Anastomoses

1. Infraorbital
Infraorbital nerve (branch of V2) and the infraorbital artery (coming off of maxillary artery)
2. Orbital
Mental nerve (branch of V3) ad our mental artery (comes of maxillary artery) comes out deep in the skull, deep to depressor anguli oris muscles and deep to depressor labii inferioris muscles
Venous Drainage: Parallels Arterial Supply

Facial arteries and facial veins travel together…and we can see that the arteries are very turbulent and has a curly nature and is more round and tubular as the facial vein usually sits superior to the artery and more flat and straight
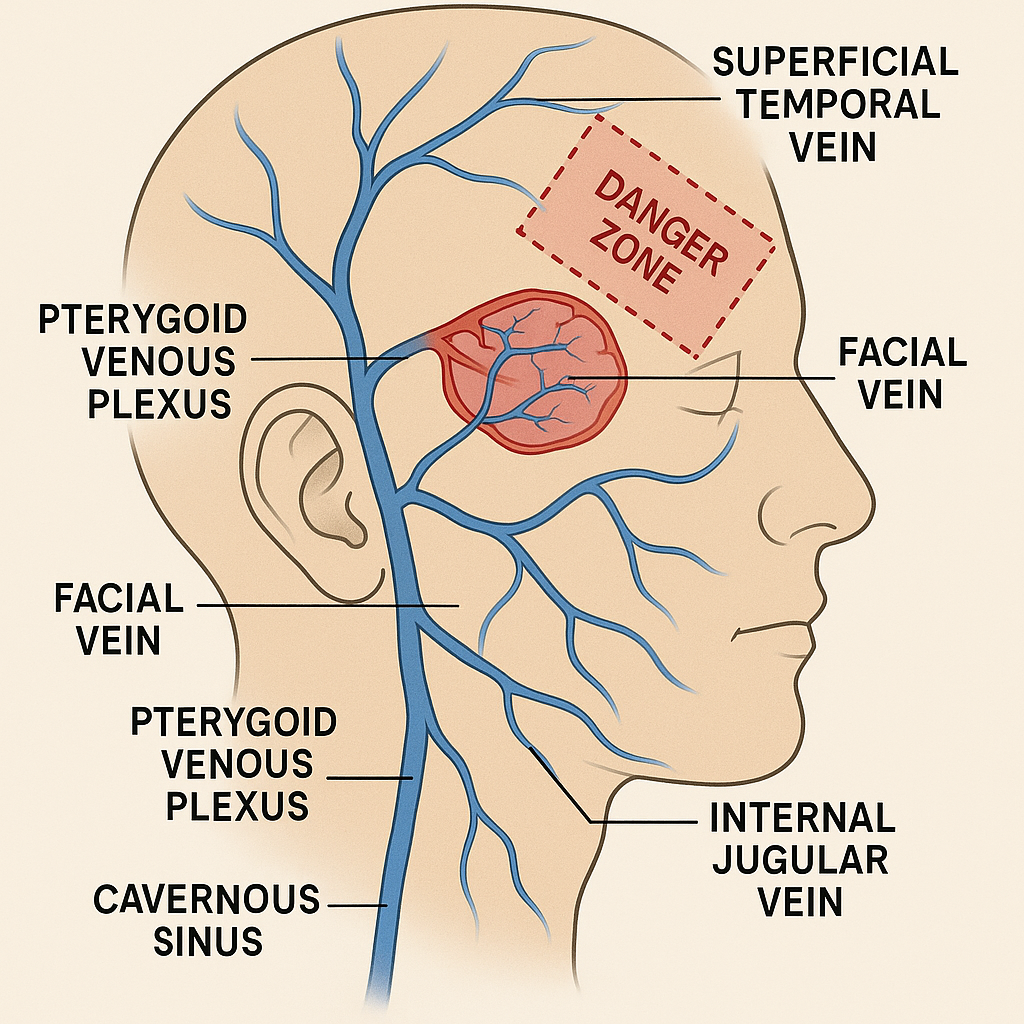
Venous Drainage in the Face

Superficial temporal vein is going to be its own branch that descend downs the side of the head where it is going to travel behind the ramus of the mandible and once that happens it is called the retromandibular vein and that is what meets up with the facial vein and together the facial vein and the retromandibular vein drain into the internal jugular vein
Deep within the cheeks we see a pterygoid venous plexus which drain venous blood from deep within the cheeks/ ear and drain into the superficial temporal vein and the facial vein
We have a venous plexus called the cavernous sinus up within that cranial cavity associated with the brian… it is involved in draining blood from the brain…there is small venous connection between the cavernous sinus (drains the brain) and the pterygoid venous plexus (drain the head)///and this connection is called the danger zone because all the veins in the region are relatively valveless meaning that there is possibility of bidirectional venous blood flow…also if you get any sort of infection is this area of the face you have a high risk of dissemination of bacteria to the brain and that can affect the brain
Where the pterygoid plexus is we have inferior alveolar nerve that comes next to it and when we are applying any anaesthetic to the face and you are targeting the inferior alveolar nerve that last thing you want to do it place the needle to far that it reaches the venous plexus which could travel up to the brain…when you but the needle in you want aspirate first make sure your not hitting any blood before you administer anesthetic
Summary of Branching for Superficial temporal vein
1. Superficial Temporal Vein
Drains blood from the side of the scalp.
Travels down the side of the head, behind the ramus of the mandible.
2. Retromandibular Vein
Formed when the superficial temporal vein passes behind the mandible.
This vein then joins the facial vein.
3. Facial Vein
Drains the face.
Joins the retromandibular vein.
Together, they drain into the internal jugular vein, which continues venous return to the heart.
4. Pterygoid Venous Plexus
Located deep in the cheeks.
A network of interconnected veins that drains deep facial structures.
Drains into both the superficial temporal vein and the facial vein.
5. Cavernous Sinus
A venous plexus within the cranial cavity.
Drains blood from the brain.
Connected to the pterygoid venous plexus via small venous channels.
⚠ “Danger Zone”
The connection between the cavernous sinus and pterygoid plexus is valveless.
Bidirectional blood flow is possible.
Facial infections (especially around the nose and mouth) can spread to the brain, risking cavernous sinus thrombosis.
6. Clinical Note – Inferior Alveolar Nerve & Anesthesia
The pterygoid venous plexus lies near the inferior alveolar nerve.
During dental anesthesia targeting this nerve:
Incorrect needle placement into the venous plexus can risk intravenous injection and potentially brain infection.
Always aspirate before injecting to avoid accidental venous access.
The Temporal VS Infratemporal Fossa

Temporal Fossa is the space above the zygomatic arch and were we find the region where multiple bones of the Neurocranium fuse together
Infratemporal Fossa is the space below the zygomatic arch but is deep to the ramus of the mandible…laterally is the ramus of the mandible, medial border is the lateral pterygoid plate, anteriorly is the posterior border of the maxilla and the posterior border is the styloid and mastoid process, superior is part of the greater wing of the sphenoid bone and parts of the temporal bone
The Temporomandibular Joint (TMJ)

The mandible attaché to the skull through the temporomandibular joint (TMJ) and this is a synovial hinge joint
typically with hinge joints is that they move along one axis in the mandibles cause in suppression and elevation but we call it a modified synovial hinge joint because the mandible can move side to side and forward and backward
the head of the mandible sits in the mandibular fossa of the temporal bone
the articular tubercle is anterior to the mandibular fossa and within the mandibular fossa we have a articular disc
Articular Disc is to add additional cushioning and reduce friction
When we move of mandible we take the head of the condyle and push it out of the fossa and back into the fossa
when our mouths our close the head of the condyle is located in the mandibular fossa
When we depress/open our mouths fully the head of the mandible comes out of the mandibular fossa and sits open the articular tubercle
e.g. put your rings in front of your ear and open your mouth fully
reinforcing ligaments are ligaments that sit outside the joint capsule that helps strengthen and support the joint
lateral ligament = extends from the Inferior part of the condyle of the mandible and goes up to the zygomatic arch
Movement of the Mandible

protrusion = forward movement of the mandible
retraction = backward movement of the mandible
elevation = closure of the mouth
depression = opening of the mouth
Muscles of Mastication - Summary
Temporalis
Masseter
Medial Pterygoid
Lateral Pterygoid
Muscles of Mastication - Temporalis
Temporalis is a muscle that originates in the temporal fossa and inserts on the coronoid process of the mandible…the muscles fibers run up and back and therefore the muscle is responsible for elevation and retraction of the mandible…It is innervated by deep temporal branch of V3 (mandibular nerve and uses the deep branches of V3)
e.g. put your fingers slightly in front of your ears and clench your jaw you will feel the muscle bulge out, also involved in chewing gum

Muscle of Mastication - Masseter
Masseter is a muscle originates at the zygomatic bone/arch and inserts at the angle of the mandible (where the ramus of the mandible comes down and curls to the front) and because of this the muscle fibers run up and anteriorly therefore it elevates the mandible and protrusion of the mandible and it is innervated by the masseteric branch of V3
masseter you can also feel bulge out the same way as the muscle above
Masseter muscles has a association with the parotid gland (salivary gland that sits in front of the ear) and the parotid duct needs to pierce through the buccinator muscle but FIRST it must travel over the Masseter muscles dive through the buccal fat pad pierces buccinator and opens up opposite to the 2nd maxillary molar
remember buccinator sits deep
Muscles of Mastication - Medial Pterygoid
The 2 Pterygoid muscle together create a number 7 on the side of the face
Medial Pterygoid origin is because it originates on the medial surface of the lateral pterygoid plate (LPP) and it inserts towards the internal (inside) surface of the angle of the mandible and it functions to elevate the mandible and it is innervated by medial pterygoid nerve (which is a branch of V3)
the medial pterygoid has 2 components one that sits superficial and another that sits deep [she doesn't care too much on this]

Muscles of Mastication - Lateral Pterygoid
Lateral Pterygoid muscle has a superior and inferior head and it originates along the sphenoid bone (superior) and the lateral side of the pterygoid plate (inferior)…it inserts into the articular disc of the TMJ (superior) and the condyle of the mandible (inferior) and this is where we the protrusion of the jaw which initiates the full depression of the jaw (bilateral function - right and left sides working together)…the unilateral function is an elevation of the mandible to the opposite side and this is during chewing (the right lateral pterygoid muscle allows you to swing the mandible to the left - contralateral)
innervated by the branch of V3 called the lateral pterygoid nerve

Summary: Innervation of Muscles of Mastication (V3)

masseteric nerve is on the inside and sits between the mandible and the masseter muscle itself
we also have the branch called the buccal nerve of V3 and this is NOT to be mistake for the buccal branch of the FACIAL nerve because this one gives sensory innervation to the inside of your cheek
buccinator closes off the lateral sides of the oral cavity if we removed it there would be the oral mucosal next and that whys the buccal branch of V3 comes in and provides sensory information to the oral mucosa
The Oral Cavity and the Palates

the nose has right and left nasal cavities that are separated by a nasal septum
the oral cavity sits inferior to the nasal cavity
the hard palate separates the oral and nasal cavities
the pharynx is a muscular tube and it is composed of 3 regions:
Nasopharynx
Oropharynx
Laryngopharynx
in order to breathe air in we need the nasal cavities internally and externally to be open
in the back we have openings called the kwana and air comes through the nasal cavity to the nasopharynx and brought down all the way to the larynx for food it travels the same path BUT it goes to the esophagus NOT the larynx
Hard palate is the roof of our oral cavity…our soft palate is muscular… at the back of our oral cavity we have our uvula which is our soft palate and that is what moves
Overview of the Oral Cavity

the floor of our oral cavity is made of muscle (mylohyoid and geniohyoid)
the lateral wall of the oral cavity is the buccinator muscle
everything in the oral cavity is covered in a mucosal membrane
at the back of our oral cavity things start to open into the oropharynx and where it starts to narrow is the oropharyngeal isthmus
Parts of the Tongue
our tongue has 2 parts
Root = sits more Inferior and posterior
Body = sits more anterior and superior
we have both general and special sensory of the tongue
special sensory = taste
general sensory = temperature, pian, touch
The posterior ⅓ of the tongue is at the back of the tongue and is more associated with the root of the tongue
the ‘V’ is called the terminal sulcus and that separates the poster ⅓ form the anterior ⅔
the tongue is right and left muscles fixed together along the midline and this is called the lingual septum
The Tongue and it’s Innervation

hypoglossal nerves (CN 12) provides motor innervation to majority of the tongue along with the Vagus nerve
posterior ⅓ of the tongue receive both sensory and special sensory innervation from CN 9 - lX (glossopharyngeal nerve)
the anterior ⅔ of the tongue general sensory comes from the lingual nerve (branch of V3) and the chorda tympani branch (branch of facial nerve) which provides special sensory to the anterior ⅔
The vagus nerve gives off general and special sensory innervation to the tongue