Lecture 8: Substance Use Disorders
1/71
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
72 Terms
What are substance related & addictive disorders?
Substance related & addictive disorders: the problematic use of drugs & other substances that people take to alter the way they think feel and behave
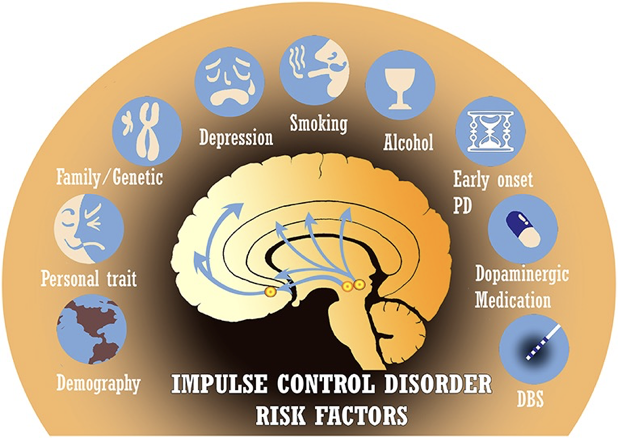
Impulse-control disorders: disorders in which a person acts on an irresistible but potentially harmful impulse
Involves the inability to resist acting on a drive or temptation
Included in this group are those who cannot resist aggressive impulses or the impulse to steal, for example or to set fires
Food vs. Drug Brain Mechanisms
There is overlap between food & drugs. Both affect cognitive control, over our behaviour.
People with ED have a lot of trouble dictating behaviours, they end up going into these cycles of high control, then breakdown, binging & then compensatory reactions (fasting, purgins, over-exercising)
With drugs, you have these areas where you try to exercise control, top-down from the front of the brain that executive network into the reward centers of the brain. This dopamine reactive system. Activation of system that supports craving
In ED & drug disorders it’s the wanting that is so problematic. It’s not bad that you feel pleasure, but this behavioural compulsion to overconsume, withhold food or go consume drug despite the fact its not in line with best interest
Major Takeaway:
Its this tension between our conscious intentions, this executive front of the brain, the prefrontal cortex network trying to exert control over behaviour & teach us whats right & wrong to do in terms of our regular habits
This dopamine reward learning network inside the brain & then there’s these core drives leading to the wanting, the compulsion to act, driven by core parts of the brain like the hypothalamus: which controls a lot of our most primitive urges, that are sending these signals that eventually when we’re not at our very best, we get worn down, stressed, override these top-down intentions & produce problematic behaviour

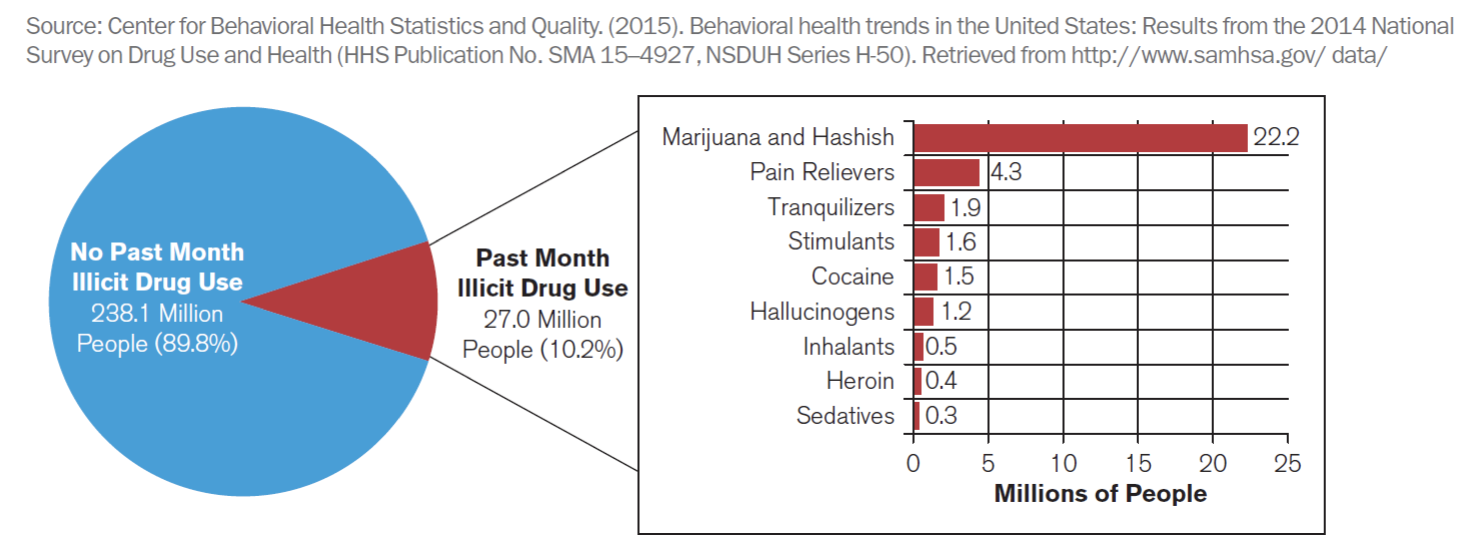
Drug Use Demographics
Drug use varies depending on the drug
Varies because its just whether the drug is illegal or not but also how profoundly, debilitating it is
Drugs like marijuana used to be illicit
Illegal drugs 1/10 people using them: a lot using painkillers, tranquilizers to regulate mood, cannabis products
At lower levels stimulants. Cocaine, hallucinogens, meth, heroin
Which drug do you think causes the most problems?
There are biological consequences
Some drugs are more physically harmful & physically addictive than others
Some drugs are addictive but not harmful in the short term
Ex. cigarettes: nicotine affects the reward system, the dopamine system in the brain. You have nicotinic receptors in the brain that hijack learning. In short-term not harmful to have one cigarette but highly addictive. Over long term extremely harmful
Not violent crime in short term
Alcohol is widely sanctioned, your brain can process it pretty well even at moderate does
In short term not super harmful, suppresses a lot of your higher cognitive function but in the short-term much more harmful because people in that disinhibited state crash cars, get into fight, make bad decisions
And even more so than cigarettes a lot of people are doing it
Heroin much more debilitating, cannot really do anything on heroin high.
Fewer people doing it so it is not affecting society at large as much but in areas where people are doing heroin, it leads to a lot of crime, people pursuing any sort of income so they can get more drugs
How you think about crime is how addictive is it? How many people are doing it? Is it addictive? Do they have choice around when they use it or not? Do they feel they have choices? Are they going to commit crimes to keep using it? Or get in trouble with the law? Are there long term and short term health consequences? Can balance all these things out to make different arguments about different drugs being the most harmful
Can make argument alcohol most harmful because so many people do it and one of the leading causes of car accidents. So its actually causing the most harm in society
Compared to heroin or meth- it’s so devastating to the individual that it's the most harmful because once you get addicted it really destroys your life in a way alcohol can but majority of people find ways of using alcohol responsibly
Cigarettes are worse because so many people do it and they do not see the harm. In the long-term it affects the healthcare system with these massively inflated rates of lung cancer and other cancers. Second hand smoke
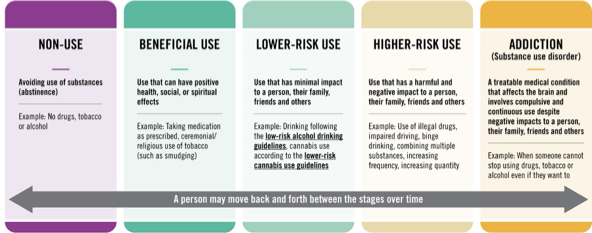
Levels of Involvement
Substance-related disorders involve problems associated with using & abusing drugs that alter patterns of thinking, feeling and behaving
Distinctive between substance use & abuse
Non use: Avoiding use of substances (abstinence)
No drugs, tobacco or alcohol
Beneficial use: Use that can have positive health, social or spiritual effects
Lots of people smoke a cigarette, smoke, consume marijuana in some way, have a drunk each night. It helps them in moderation to feel like they have some time for themselves, maybe there’s some stress fraction effects, and social facilitation effects
Alcohol social lubricant, smoke on work break-some benefits.
Marijuana for pain and appetite.
Lower risk use: It’s under control, not impairing function, not missing out on work events or social events. Has a minimal impact to a person, their family, friends and others.
Acts as a social facilitator
Higher-risk use: Use that has harmful & negative impact to a person, their family, friends & others
ex. use of illegal drugs, impaired driving, binge drinking, combining multiple substances
Starting to miss out on things, make mistakes, using money or other resources that you don’t have to spare to support your use
Addiction: Treatable medical condition that affects the brain & involves compulsive & continuous use despite negative impacts to a person, their family, friends & others
Higher risk activities, unsafe, putting self into unsafe environments
Do not have control, feel compelled to keep using the drug & it really starts to take out
Missing out on a lot of important events, not studying, not showing up, more isolated
Become persons whple life
What is a substance? What are psychoactive substances?
Substance: Chemical compound ingested to alter mood & behaviour
Nasally, orally, intravenously
Psychoactive substance: alter mood, behaviour or both
Include commonplace legal drugs, such as alcohol, nicotine, the caffeine in coffee & tea
Levels of Involvement- Use
Ingestion of psychoactive substances in moderate amounts
Does not significantly interfere with social, educational or occupational functioning
Use is using the drug
Cannabis legalized in Canada in 2018
Levels of involvement- Intoxication
Substance intoxication: Our physiological reaction to ingested substances-drunkenness or getting high is substance intoxication
Interaction of variables
Type of drug taken (relative to body weight, how it is metabolized) the amount ingested, and the person’s individual biological reaction (how it affects perception, thoughts, feelings & behavior)
Intoxication experienced as impaired judgment, mood changes, and lowered motor ability
Substance intoxication is when the drug actually affects you, you feel different and start acting differently
Substance intoxication: physiological reactions such as impaired judgment & motor changes as well as mood changes, resulting from the ingestion of psychoactive substances
What is substance use disorder?
Substance use disorder: Defined in terms of how significantly the use of any substance interferes with the user’s life, use disrupts education, job, relationships & puts them in physically dangerous situation
When a person starts to get into trouble. They start having problems with self-regulation, meeting commitments.
Loss of control around substance use
Usually described as an addiction
To meet the criteria for a disorder, a person much have at least 2 symptoms in the last year that interferes with their life or bothered the person a great deal
When the person has 4 or 5 symptoms they are considered to fall in the moderate range
A severe substance use disorder is someone who has 6 or more symptoms
Physiological & Psychological dependance
What is physiological dependence?
One definition considers addiction as physiological dependence on the drug or drugs, involving tolerance & withdrawal.
Tolerance: greater amounts of drugs needed to experience the same effect
People take more and more levels of the drug to feel like the ‘first high’
Not that the person wants to be higher than they ever have before, they might be trying to maintain the same level of intoxication but because the body learns how to break it down more quickly and psychologically, you learn how to compensate automatically. Take more and more to overwhelm this tolerance, leading to overdose.
Withdrawal: negative physical response when the substance is no longer ingested
Feeling you are much worse than normal when you don’t have drug in system.
You don't just go back to normal, you feel hungover from alcohol, you feel edgy when you don’t have heroin and other opiates in your system. You feel like everything is boring and pointless when withdrawing from cocaine or other types of stimulants.
Left worse than you were before and the way just to even get back to baseline is to take more of the substance.
Chills, fever, diarrhea, nausea & vomiting, aches & pains
Not all substances are physiologically addicting, however. For example, you do not go through severe physical withdrawal when you stop taking LSD. Cocaine withdrawal has a pattern that includes anxiety, sleep changes, lack of motivation, and boredom, and withdrawal from cannabis includes such symptoms as irritability, nervousness, appetite change, and sleep disturbance.
What is psychological dependance?
Behavioural reactions to substance dependance
Desire to seek & take the substance
Inability to avoid or limit taking the substance
Experience of negative emotional states when the substance isn’t available
Dependence can be present without misuse
A lot of people dependant on coffee but functional
Drink or smoke & dependant on it. Feel bad & dysregulated if they were to have to stop all of a sudden, headachy, irritable. But not spiraling out of control.
Pattern where used the substance because it produces pleasurable outcome but more likely over time as tolerance builds up, your just trying to avoid the negative outcomes of withdrawal is this idea of psychological dependence
Any kind of stressor or where you feel like you need help regulating or already feel on edge, perhaps because of withdrawal symptoms make it more and more likely that you will try to avoid that negative situation. Whether it’s being stressed, being in withdrawal and both happening together.
Although you can think of addiction as being overly focused on pleasure. The experience for most addicts is not really pleasure anymore but rather trying to get back to baseline because they’re so used to being in the intoxicated state
A lot of substance use is about experimental avoidance of the consequences of coming off the substance and also people are using it to get away from and avoid other negative things in their life. It distracts them.
Pleasure taking you away form unpleasant/unwanted circumstance
Substance dependence is usually described as addiction, though there is considerable disagreement about how to define addiction.
One definition considers addiction as physiological dependence on the drug or drugs, involving tolerance and withdrawal. Another view uses drug-seeking behaviours themselves as a measure of psychological dependence
Other symptoms that make up a substance use disorder include drug-seeking behaviours. The repeated use of a drug, a desperate need to ingest more of the substance (stealing money to buy drugs, standing outside in the cold to smoke), and the likelihood that use will resume after a period of abstinence are behaviours that define the extent of substance use disorders. Such behavioural reactions are different from the physiological responses to drugs we described before and are sometimes referred to in terms of psychological dependence
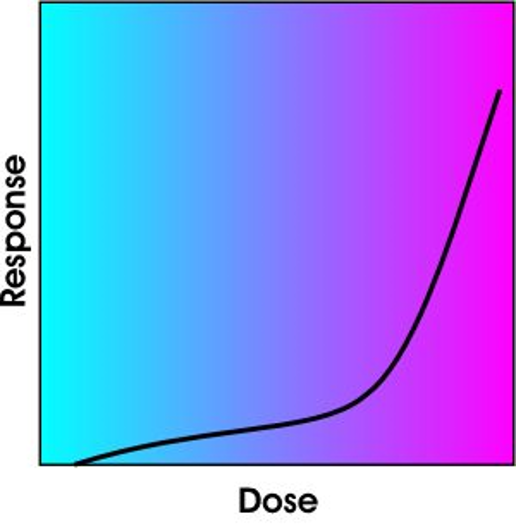
Tolerance
Tolerance: Decreased sensitivity to a drug as the consequence of long-term exposure to it.
Decreased in response
Increase in amount needed
Shift-dose response curve
Neuroadaptation
Tolerance: means that a person needs increased amounts of the substance to achieve the same effect. This occurs as use of a drug becomes more frequent.
The amount you need to take of any substance before you get that psychological response is known as this kind of dose-response curve & you might feel like a glimmer of something but once you get enough of the substance, now it produces the high.
Microdosing: earlier part of curve, not full-blown high. Little things are popping up differently for them but it hasn’t actually activated the full subjective experience so in theory safer like a slower kind of burn
Dose response curve shifts further to the right, the more you take a substance and that’s what tolerance is. You need to take a bigger and bigger dose to activate the actual high, so the whole curve is shifting further and further right this is known as neuroadaptation
Neuroadaptation: both at the biological level, you body’s getting better at clearing & regulating the effects of the drug & at a psychological level, you’re automatically learning to compensate & even expect the presence of those drug effects so that the overall net affect is lower.
Take larger dose to activate that quick rise & the side effects the consequences, toxicity of the drug accumulate as you take a larger and larger dose, hoping you’re going to get that bump.
Some other addiction terms
Abuse: use of a drug that causes culturally determined conflict
Reinforcement: the reward obtained by performing the addictive behaviour
Learning that if we take the drug it’ll be good for us, either because it produces pleasure, arousal or connection.
Also has a lot of negative reinforcement: it will help us stop feeling bad, stop feeling stressed, stop feeling withdrawal symptoms
Dependence: neuroadaptation to the addictive substance, promoting craving & withdrawal symptoms
That adaptation that just to get to a baseline state, the brain is now used to having the drug in its system, so it feels like something’s missing. It creates this behaviourally motivational wanting. It's wanting, that something is missing.
Marijuana not strong physical dependance but very strong psychological dependance: euphoric, not super agitated state of high. Feels like something wrong when not smoking.
Rebound: exaggerated addictive behaviour following an attempt to quit
Period of abstinence, when the person loses control again, they end up taking even more of the drug than they normally would
So exaggerated addictive behaviour following an attempt to quit.
DSM-5 & ICD-10 Definitions
Intoxication: typically impairment to psychological processes and behavioral abilities
Withdrawal: symptoms when the substance is reduced or no longer used
Disordered use: use of the substance causes the person to experience significant impairment or distress
Withdrawal
Feelings of restlessness or irrationality
Time will be spent obtaining & using the substance
Usually involves opposite effect of drug
E.g., extreme sensitivity following prolonged exposure to opioids
Opiate. Heroin takes away the ability to feel pain, then you’ll be super sensitive to any kind of sensory event as painful as you withdraw.
If it makes you feel really calm and not nauseous will do the opposite
Withdrawal refers to unpleasant and sometimes dangerous symptoms when the addictive substance is removed from the body.
Psychological dependence, or habituation, refers to being psychologically accustomed to a substance due to regular use.
When it comes to addiction, your brain works a bit like a spring. Drugs & alcohol push down that spring & suppress your brain production of neurotransmitters. And then, when you stop using drugs or alcohol its like taking the weight off the spring. And you rebound by producing a surge of adrenaline that causes withdrawal symptoms
Who becomes addicted?
Those who start drinking before 15 are 4x as likely to become addicted
Earlier you start to earlier those patterns form
40-50% of variations of drug vulnerability can be tied to genetics
Epigenetics appears to play a rule in drug vulnerability, with parent addiction possibly affecting child vulnerability
Drug addiction ties to other pathologies, including gambling, sex addiction, bulimia, affective disorders, ADHD, anxiety disorders, personality disorder
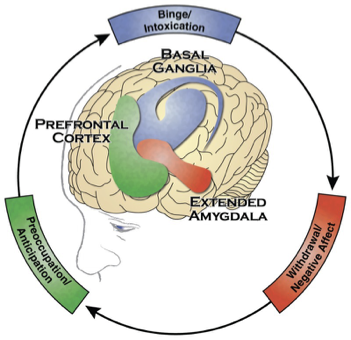
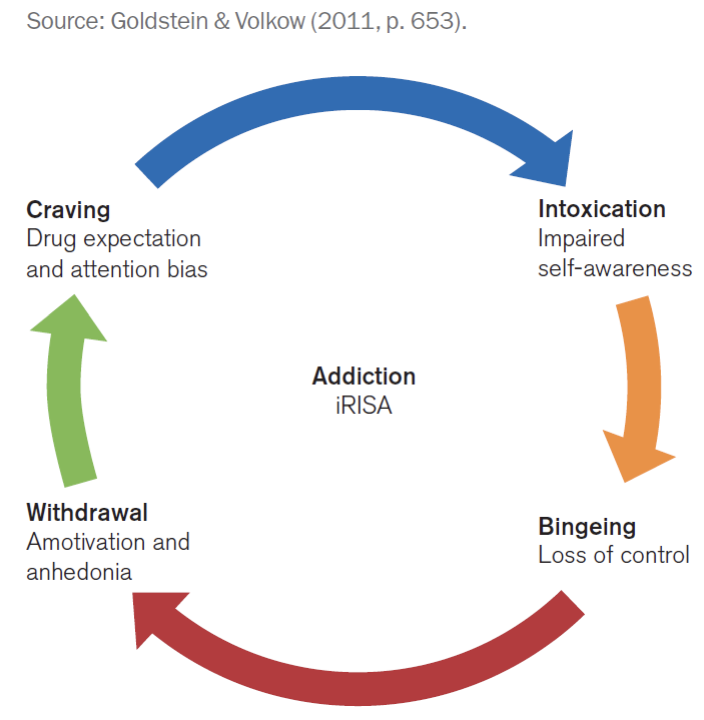
Patterns of Addiction
Patterns follow a typical, predictable pattern
Addiction follows this general cycle, where you have people binging & they have a kind of reward learning that something is good.
Withdrawal is triggering all this negative affect. The salience network is going crazy, saying something is wrong, you need to go find the thing that makes things better
Starting to think about how you’re going to get the substance again, starts to occupy your attention. So then the executive network, the prefrontal cortex, the cognitive system starts to become really engaged in drug-seeking behaviour
When get drug again, back into the reward circuitry, then the withdrawal back into the emotional circuitry & then that motivates you to start thinking about how you’re going to get more again
So that starts forming the cycle in terms of brain dynamics
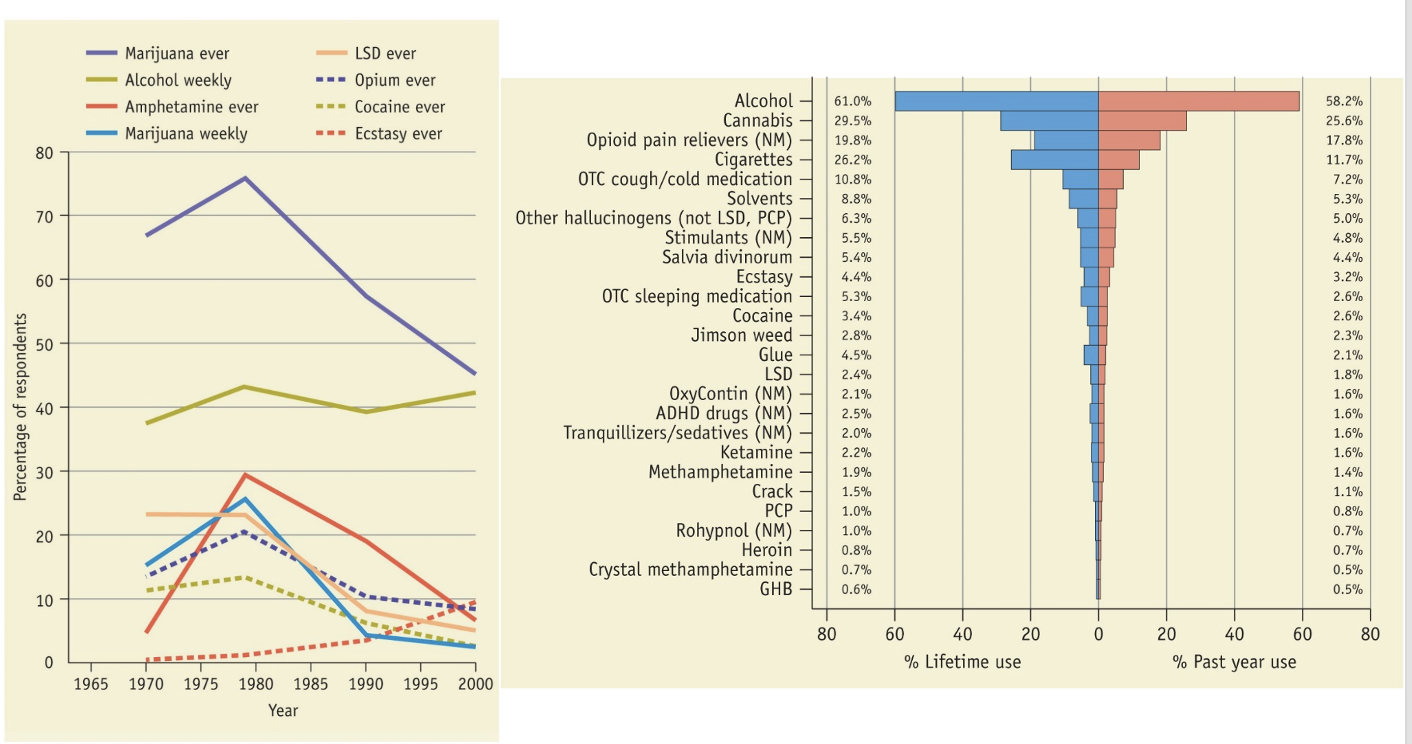
Here are some stats about popularity. As you can see, the 80s were a high time for drug use.
The only drug that is becoming more popular is ecstasy. And alcohol is remaining pretty steady over time.
Maijuana and alcohol most popular
Compared to 60s and 70s a lot of people are just choosing not to use substances which is interesting
People in last 20 years lowest levels of substance users.
Better education?
Molly, ecstasy more common- party drugs
Hallucinogens, psychedelics are becoming much more popular again
A continuum of risk
This is a really interesting diagram, because it compares the addictive level of a drug to how physically harmful it is to a user.
How addictive it is and how much physically it’s bad for you are 2 ways of doing it
So you see that the most addictive drugs are also the most harmful, like coke and heroin (most addictive, harmful to body, social harm, crime, people not working, taking care of family); whereas pot and ecstasy are slightly more on the safer and less addictive end of things.
Psychedelics least harmful, can mess up sanity and change worldview: difficult to physically harm yourself on most psychedelics such as LSD or mushrooms even though you can feel sick in the short-term. Don't form dependence easily.
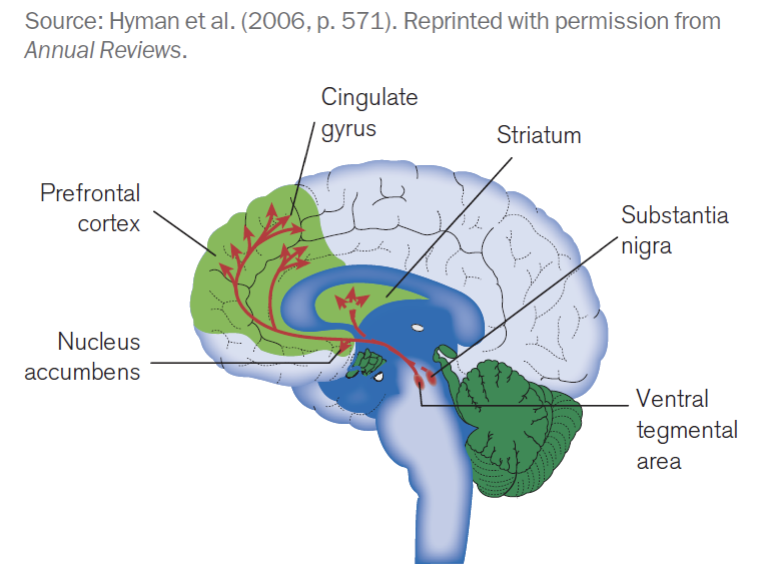
Drugs & the Brain
The reward of drugs comes from the release of dopamine in the mesolimbic dopamine system
Dopamine: midbrain reward or learning system & creates this craving cycle
How do drugs affect the brain?
The striatum is where we are doing a lot of our reward processing & learning & the prefrontal cortex is where we do our planning
So the things that are seen as really important learning influence what we pay attention to at the prefrontal cortex
Drugs & the Brain
Those with low dopamine levels show compulsive behaviours, hypersexuality & gambling when dopamine is raised
The ‘high’ from a drug affected by speed of entering the brain
Dysfunction is the prefrontal cortex is associated with drug addiction
The societal cost of substance abuse
In Canada, alcohol and illicit drugs costs 14 billion dollars a year
There are 86,000 admissions to Canadian hospitals each year for alcohol-related health reasons
Alcohol is associated with more than half of traffic deaths and homicides and 30% of all suicides.
In 2002, 19.3% of all deaths in Canada were attributed to alcohol, tobacco, or illicit drugs.
Drug use & abuse across cultures
Muslim cultures may impose strict sanctions for the use of any drugs; China did at the time of the cultural revolution
In the UK, drug abuse is viewed as a medical problem.
The Dutch make a clear distinction between soft and hard drugs.
Soft drugs are decriminalized
Psychedelics considered soft drugs
Whereas cocaine and heroin might still be prohibited
Many South Americans, Middle Easterners, and East Africans regularly chew khat and see nothing deviant in doing so.
Something like cocaine response but not as intense
Many First Nations groups across the Americas use psychoactive agents in religious ceremonies
The set and setting, the mindset of a person and both the social and physical environment around them determine whether drug use can be something spiritual or meaningful or a source of bonding
Drinking in alleyway versus in bar with friends
The appropriateness and healthiness from a social perspective of the drugs really varies based on why you’re using it, who you’re using it with and what context
Diagnostic issues
Substance use might occur concurrently with other disorders; hard to know which to address first
Are they depressed because of how much time they’re on drugs? Or are they using drugs to deal with the fact they’re depressed all the time? And which one are we going to pick first?
Drug intoxication and withdrawal cause increased risk taking
Mental health disorders cause substance use disorder
What are the 5 general categories of substances?
Depressants
These substances result in behavioural sedation & can induce relaxation.
They include alcohol, sedative & hypnotic drugs in the families of barbiturates, benzodiazepines (e.g, valium, Halcion, Xanax)
Bring down arousal in the brain & body
Stimulants
These substances cause us to be more active & alert & can elevate mood
Amphetamines, cocaine, nicotine & caffeine
Raise arousal
Opiates
Temporality reduce pain & euphora
Heroin, opium, codeine, morphine & oxycodone are included in this group
Bind with pain receptors in the brain & prevent you from processing pain information among other types of sensory information from the body
Hallucinogens
These substances alter sensory perception and can produce delusions, paranoia, and hallucinations. Cannabis and LSD are included in this category.
Other drugs
Other substances that are misused but do not fit neatly into one of the categories here include inhalants (e.g., airplane glue), anabolic steroids, and other over-the-counter and prescription medications (e.g., nitrous oxide). These substances produce a variety of psychoactive effects that are characteristic of the substances described in the previous categories.
Short-term highs, euphoric, pleasurable or dissociative effects
Sniffing glue
What are depressants?
Depressants decrease CNS activity, reduce arousal & help people relax
Included in this group are alcohol and the sedative, hypnotic, and anxiolytic drugs and those prescribed for insomnia. These substances are most likely to produce symptoms of physical dependence, tolerance, and withdrawal.
Alcohol
Barbiturates
Benzodiazepines
Alcohol- Related Disorders
Sedative, hypnotic & anxiolytic-related disorders
Most people drink moderate amounts but ¼ people would be described as frequent drinkers
Canadian Consumption Patterns
Drinking extremely popular in Canada
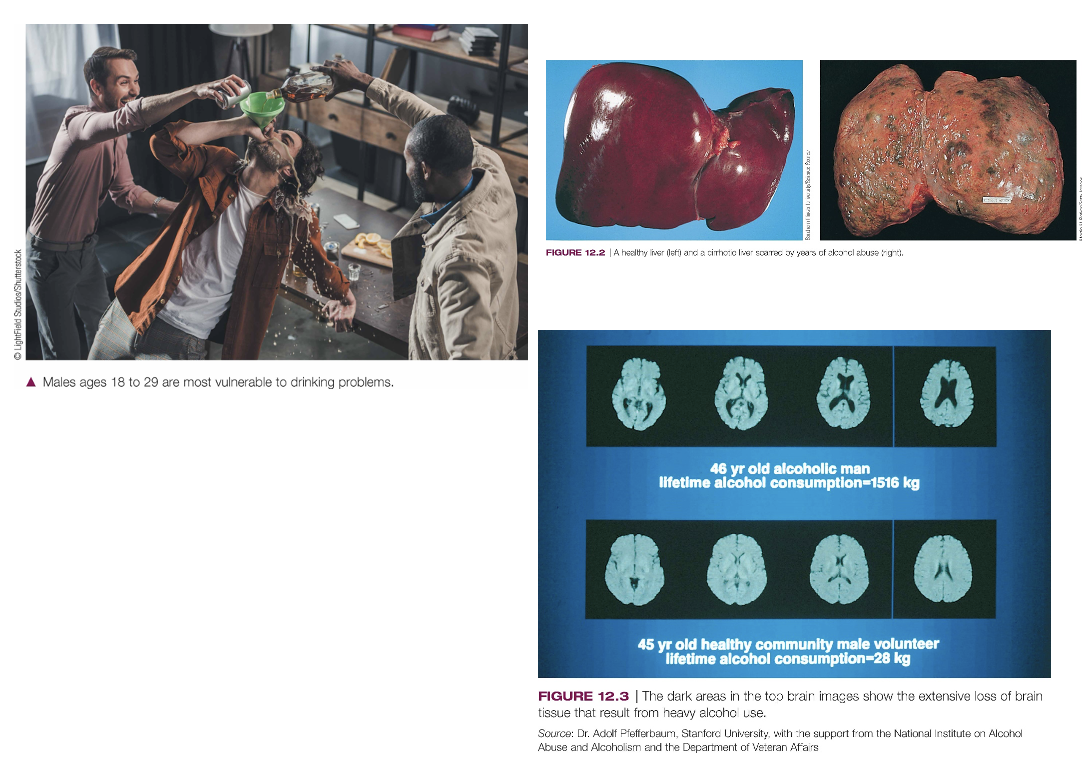
The rate of drinking is higher for males (82%) than females (77%), and highest for young adults and single people.
The largest groups of drinkers are light, infrequent (39%) and light frequent (28%) drinkers.
About 6% are heavy infrequent and 7% are heavy frequent drinkers.
Alcohol use is extremely prevalent across Western countries.
Prevalent in countries where it’s illegal
What is the clinical description of alcohol-related disorders?
Depressant, inhibitory centers in the brain are depressed or slowed
Continued drinking depresses more areas of the brain
Impaired motor coordination
Slower reaction times
Confused, poor judgments
Vision & hearing affected
What are the effects of Alcohol?
Influences several neuroreceptor systems
GABA, inhibitory neurotransmitter, blackouts
Alcohol causes higher levels of GABA release so if enough of it gets released, it knocks out other systems. It can knock out the hippocampal memory system & that’s why have blackouts
Release natural analgesics
Which tie into the pain perception system, so you become numb to pain
The serotonin system also appears to be sensitive to alcohol. This neurotransmitter system affects mood, sleep & eating behaviour & is thought to be responsible for alcohol craving
Alcohol also exerts effects on dopamine reward system & these effects may be responsible for the pleasurable feelings people experience when drinking alcohol
We generally experience a feeling of well being, inhibitions reduced and we become more outgoing
These reactions occur partly because the inhibitory centres in the brain are initially depressed (in the sense of slowed)
With continued drinking, however, alcohol depresses more areas of the brain, which impedes the ability to function properly.
Motor coordination is impaired (staggering, slurred speech), reaction time is slowed, we become confused, our ability to make judgments is reduced, and even vision and hearing can be negatively affected, all of which help to explain why driving while intoxicated is very dangerous.
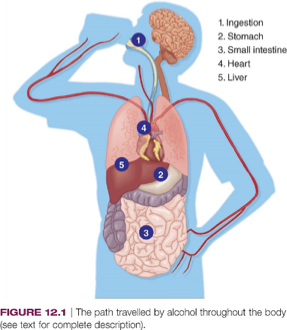
Alcohol
Alcohol goes back to prehistory
Widely used for celebrations due to mild euphoria & increased social interactions
Wide cultural variations in use
Moves directly into blood
Food in stomach shows alcohol absorption, CO2 increases it
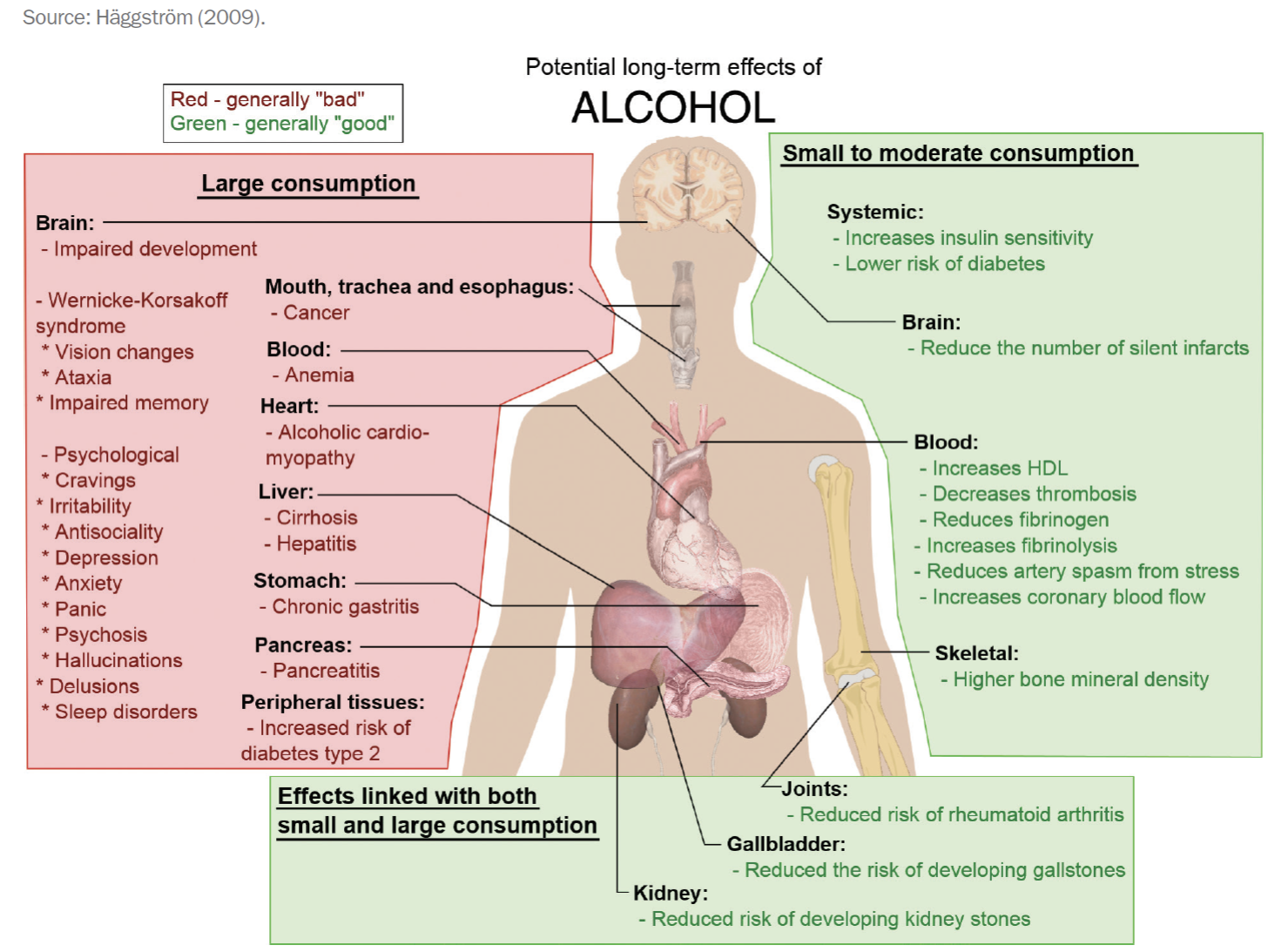
Alcohol Effects on the Body
Small to moderate consumption can be beneficial, it can reduce swelling response
Chronic inflammation is really bad. So it can reduce a lot of risk of things like arthritis or some digestive issues, blood flow issues, small amounts
Larger amounts very mad
Mess up DNA transcription, physically are toxic, erode base of brain
If they arose the mammillary bodies, they lead to Korsakov syndrome: where a person completely loses the ability to assess the memory system. They have no idea who they are, where they are, what they are doing
Long-term drinkers have these issues
Vitamin deficiencies
With brain impairments can get all kinds of disorders like panic, hallucinations, memory loss, antisociality, depression
Liver & kidneys hit
Liver cirrhosis: death of liver common sign of chronic alcoholism
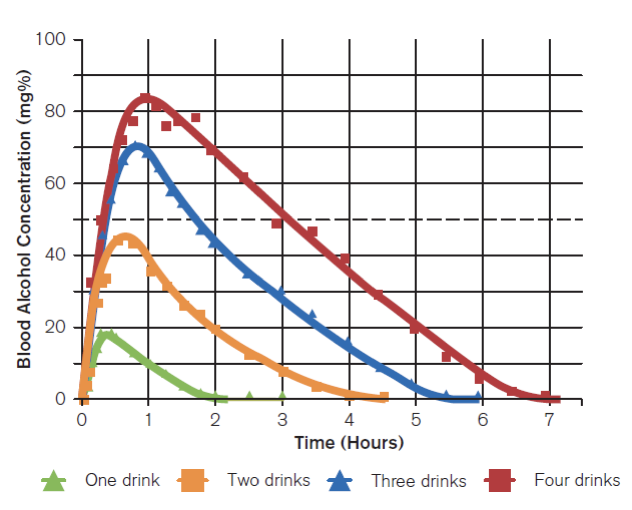
Blood Alcohol Levels
Blood alcohol levels in males as a function of number of drinks within an hour
We measure blood alcohol levels by how much its concentrated in your blood
On average people can clear about 1-2 drinks per hour. So if you have 1 drink by the time you’re 2 hours out, you should be back to baseline
If add more drinks longer and longer to clear those drinks
What are some alcohol disorder effects?
Delirium Tremens (DTs): frightening hallucinations & body tremors
Can have tremors as it erodes some of the basal ganglia that controls motor movement
Fetal alcohol syndrome (FAS): affects child whose mother drank during pregnancy
Fetal growth retardation, cognitive deficits, behaviour problems & learning difficulties
Effects of Long-term Alcoholism
Consequences of long-term excessive drinking include liver disease, pancreatitis, cardiovascular disorders & brain damage
The dark areas in the top brain images show the extensive loss of brain tissue that result from heavy alcohol use.
Ventricles enlarged
Healthy liver (left) and a cirrhotic liver scarred by years of alcohol misuse (right)
What are the stats on use & abuse?
23% Canadians exceed low-risk guidelines for alcohol consumption; 17% high-risk drinkers
Binge consumption frequent among college students
Men drink more than women
Single males most likely to be heavy drinkers
Cultural differences exist
Particularly prevalent in Indigenous groups in Canada and other parts of the world.
Heavy drinking was studied in the 2018 Canadian Community Health Survey. Heavy drinking in the past year was defined as five or more drinks on one occasion for men, four or more drinks for women, at least once a month for the past year.
A study of health inequalities in Canada revealed that, compared to non-Indigenous peoples, heavy drinking was more prevalent among Inuit, Métis, and First Nations people living both on and off reserve (Public Health Agency of Canada [PHAC], 2018).
Progression of alcohol related disorders
Fluctuations between heavy drinking and abstinence (like ED)
Gets worse if untreated/unchecked
Early consumption can predict dependence/abuse in later years
The way people act & get used to act is how they tend to act tends to get worse if it's not treated
Early use of alcohol predicts later misuse
Linked with violent behaviour; may reduce the fear of punishment
People inhibited cannot conceive or properly calibrate consequences of actions
Depressants: Sedative, Hypnotic & Anxiolytic Related disorders
The general group of depressants also includes…
Sedative (calming)
Sedatives are to immediately calm someone down, lower arousal and pump GABA into the brain
Hypnotic (sleep-inducing)
Help people sleep
Anxiolytic (anxiety-reducing)
Barbiturates: synthesized sedatives (sleep-aids)
Benzodiazepines: anxiety-reducing
Most of them have this common pathway for reducing anxiety but most of them have this common pathway of increasing the inhibitory signalling in the brain
Some more addictive than others
Older classes of anxiolytic sedative drugs like barbiturates and benzodiazepines are powerful calming agents but they can also evoke dependency because get used to them for keeping themselves
What are barbiturates and benzodiazepines?
Barbiturates relax muscles
Low doses produce mild feeling of well-being
Larger doses can have results similar to those of heavy drinking: slurred speech and problems walking, concentrating, and working. At extremely high doses the diaphragm muscles can relax so much as to cause death by suffocation
Overdosing is common means of suicide
Very easy to overdose on because you can relax tone in muscle regions like the heart and lungs that you ought not to be relaxing
Top-down psychological level & leave the person to feel kind of numbed out, dissociated a little bit, easier to sleep & relax, everything seems dreamlike
Benzodiazepines: calming, induce sleep
Tolerance and dependence with repeated use
People who use them for nonmedical reasons report first feeling a pleasant high and a reduction of inhibition, similar to the effects of drinking alcohol. With continued use, however, tolerance and dependence can develop. Users who try to stop taking the drug experience symptoms like those of alcohol withdrawal (anxiety, insomnia, tremors, and delirium
Sedative, hypnotic, and anxiolytic drugs affect the brain by acting on the GABA neurotransmitter system, although by mechanisms slightly different from those involving alcohol. As a result, when people combine alcohol with any of these drugs, there can be synergistic effects (Fils-Aime, 1993). In other words, if you drink alcohol after taking a benzodiazepine or barbiturate, the total effects can reach dangerous levels.
What are the statistics of Sedative-, Hypnotic-, and Anxiolytic-Related Disorders?
Benzodiazepine use declined by 6% between 2016–2017 (CIHI, 2018)
CTADS, 2019: 12% of Canadians reported using sedatives in the past year
9% of men and 14% of women
What are stimulants?
Stimulants are the most widely consumed drug in Canada, and include caffeine, nicotine, amphetamines & cocaine
“Uppers”-such drugs increase alertness and increase energy
Most commonly abused stimulants are things like cocaine, crack, ectasy
Stimulants are prescribed for ADHD- the inattention is often due to things not seeming rewarding or interesting enough & then the wrong things seeming interesting- stimulate the brain
Ritalin or Adderal
Variations of cocaine, not quite as strong but the same general principle. So they lead to kind of high
Stimulant related disorders- Amphetamines
“Uppers” leading to a “down” and crash
Reduce appetite, weight
Reduce fatigue
Induce feelings of elation & vigour
You feel “up.” After a period of elevation, however, you come back down and crash, feeling depressed or tired.
Amphetamines are prescribed for people with narcolepsy: a sleep disorder characterized by excessive sleepiness
Some of these drugs (Ritalin) are even given to children with attention-deficit/hyperactivity disorder
DSM-5 Diagnostic Criteria for Intoxication in amphetamine use disorders
Behavioural symptoms: euphoria, changes in sociability, interpersonal sensitivity, anxiety, tension, anger, stereotyped behaviours, impaired judgment, and impaired social or occupational functioning
Physiological symptoms: heart rate or blood pressure changes, perspiration or chills, nausea or vomiting, weight loss, muscular weakness, respiratory depression, chest pain, seizures, or coma
MDMA, “ecstasy”: recreational drug
Stimulate central nervous system
Enhance activity of norepinephrine and dopamine
Lead to hallucinations and delusions
Severe intoxication or overdose can cause hallucinations, panic, agitation, and paranoid delusions
However enjoyable these new amphetamines may be in the short term, the potential for users to become dependent on them is extremely high, with great risk for long-term difficulties
Amphetamines stimulate the CNS by enhancing the activity of norepinephrine & dopamine
Stimulant-Related Disorders- Cocaine
Derived from leaves of coca plant
Increases alertness, blood pressure, causes insomnia
Statistics: Use increased in Canada from 1% to 2%
Stimulants- Tobacco Related Disorders
Nicotine in tobacco is a psychoactive substance
Produces dependence, tolerance, withdrawal
15% of Canadians smoke
Inhaled nicotine enters blood in 7–19 seconds (very quickly enters bloodstream)
Stimulates pleasure pathways
Nicotine and depression interrelated
Genetic vulnerability and life stresses combine to lead to vulnerability to nicotine use and depression
Nicotine in small doses stimulates the central nervous system; it can also relieve stress and improve mood. However, it can also cause high blood pressure and increase the risk of heart disease and cancer and is the leading cause of preventable disease and death worldwide
High doses can blur vision, cause confusion, lead to convulsions, and sometimes even cause death.
Stimulants- Caffeine Related Disorders
“Gentle stimulant” found in tea, coffee, many soda drinks, cocoa products
Called gentle stimulant because it is thought to be the least harmful of all addictive drugs, caffeine can still lead to problems like those caused by other drugs (e.g., interfering with social and work obligations
In small doses elevates mood, decreases fatigue
Causes insomnia
Because caffeine takes a relatively long time to leave our bodies (it has a blood half-life of about six hours), sleep can be disturbed if the caffeine is ingested close to bedtime.
Tolerance and dependence with overuse
DSM-5 includes caffeine use disorder:
Problematic caffeine use that causes significant impairment and distress
Caffeine’s effect on the brain seems to involve the neuromodulator adenosine and, to a lesser extent, the neurotransmitter dopamine (Juliano et al., 2015). Adenosine plays an important role in the release of dopamine and glutamate in the striatum, which may explain the elation and increased energy that come with caffeine use
What are Opiods?
Knock our or the compete with pain receptors and stop pain signals from reaching the brain
Opiate: natural chemicals in opium poppy having a narcotic effect
The opioid receptor is a natural receptor in the brain that’s used to control pain signalling and out body does produce endogenous opiates- means it comes from inside our body to help us deal with pain after we get that initial signal
Sleep-inducing, pain-relieving (analgesic)
Canada in grip of opioid crisis: prescription and illegal; high in First Nations adults
Withdrawal is unpleasant
Intravenously taken: risks of HIV
Because such drugs are usually injected intravenously, users are at increased risk for HIV infection and therefore AIDS
High mortality rates
The term opioids refers to a family of substances that include natural opiates, synthetic variations (i.e., methadone, pethidine), and comparable substances that occur naturally in the brain (e.g., enkephalins, beta-endorphins, and dynorphins). Heroin, opium, codeine, and morphine are included in this group.
What are Hallucinogens?
Most popular these days
Ketamine: horse tranquilizer that has hallucinogenic properties.
Create distortions in perception and cognition, mostly by weakening the inhibitory links.
LSD (acid; d-lysergic acid diethylamide)
Commonly known
Psilocybin (mushrooms), lysergic acid amide, dimethyltryptamine (DMT), mescaline (peyote), phencyclidine (PCP)
Create differences in time perception, cause perceptual distortion, they can make you hear or see things that aren’t there so perceptual hallucinations
As the drug clears your system, you come back down to Earth, and stability reinstated
Acid trip takes 6-12 hours, mushroom trip is 3-6 hours, DMT 15 min long but might be subjectively hours, days or lifetime of subjective experience when people recount the intensity of information processing that occurred during those times
Tolerance develops quickly to many of the hallucinogens, including LSD, psilocybin, and mescaline (hallucinogen use disorders); taken repeatedly over several days, these drugs completely lose their effectiveness. Sensitivity returns after about a week of abstinence, however.
For most hallucinogens, no withdrawal symptoms are reported.
Stories in the press about people jumping out of windows because they believed they could fly or stepping into moving traffic with the mistaken idea that they couldn’t be hurt make for sensational reading, but little evidence suggests that using hallucinogens produces a greater risk than being drunk or under the influence of any other drug.
Stories in the press about people jumping out of windows because they believed they could fly or stepping into moving traffic with the mistaken idea that they couldn’t be hurt make for sensational reading, but little evidence suggests that using hallucinogens produces a greater risk than being drunk or under the influence of any other drug.
What are the DSM-5 Diagnostic Criteria for Hallucinogens?
Perceptual changes: subjective intensification of perceptions, depersonalization, and hallucinations
Physical symptoms: pupillary dilation, rapid heartbeat, sweating, blurred vision (American Psychiatric Association, 2013).
Most of these drugs bear some resemblance to neurotransmitters
Hallucinogen- Cannabis
Cannabis (marijuana) most routinely used drug in Canada; 2019 cannabis use was 15%
People who smoke marijuana experience altered perceptions of the word; mood swings
Users often report heightened sensory experiences, seeing vivid colours or appreciating the subtleties of music
The feelings of well-being produced by small doses can change to paranoia, hallucinations, and dizziness when larger doses are taken
Impairment of memory, concentration, motivation, self-esteem, relationship with others and employment are common negative outcomes of long-term use (possibly leading to cannabis use disorder)
“Reverse tolerance” with repeated use: when regular users experience more pleasure from the drug after repeated use
Tetrahydrocannabinols (THC): a variety of marijuana
The brain makes its own, too!
Chronic users who stop taking the drug report a period of irritability, restlessness, appetite loss, nausea, and difficulty sleeping (Bahji et al., 2020), but no evidence suggests they go through the craving and psychological dependence characteristic of other substances.
Hallucinogens is much lower than the harms of other drugs because it’s very hard to overdose. They’re not physically dependent
Less likely to have compulsive seeking of the drug in the future kind of thing
What are other drugs?
This class does not fit neatly into the previous categories and includes inhalants, steroids, and designer drugs.
Inhalants include several substances found in volatile solvents and breathed into the lungs directly.
Spray pain, paint thinner, amyl nitrate, glue, gasoline, laughing gas, nail polish remove, felt-tipped markers
Steroids are derived or synthesized from testosterone.
People use to rapidly increase muscle growth for either performance or aesthetic
Designer drugs refers to a growing group of drugs produced by pharmaceutical companies to target specific diseases or disorders.
What are the Biological Causes?
Familial & Genetic Influences
Genetic vulnerability to drug abuse, alcoholism
A gene of chromosome 4 may prevent alcohol depence
Some people experience more of an intense high. There are different genes that help us break down different substances more quickly
Alcohol dehydrogenase (ADH) may be absent in some people
Enzyme that helps people metabolize alcohol
The result is a physiological response, known as the skin-flushing response, characterized by reddening and warmth of the face, dizziness, and nausea. This response is thought to contribute to the relatively low rates of alcohol-related disorders in people of Asian descent
Gene DRD2 may be related to alcoholism
Twin, family, and adoption studies indicate that certain people may be genetically vulnerable to drug abuse.
What are the Neurobiological Causes?
Psychoactive drugs activate reward center of the brain. People are positively reinforced for using drugs & negatively reinforced when the drug remove unpleasant experiences such as pain, feeling ill or anxiety or result in withdrawal symptoms
Dopaminergic system and its opioid-releasing neurons known as MOP-r receptors implicated
Sensitization: repeated exposure to stimulant drugs leads to increased dopamine release when taking the drug
Negative reinforcement
Over time, the amount of receptors that can activate any part of the brain will change depending on the concentration or availability of the binding agents
So if you never have dopamine in the midbrain, eventually your brain will grow more to receptors to make sure it catches the bits of dopamine that are available so it doesn’t miss a signalling opportunity.
Binding sites will disappear. They’ll be broken back down if there’s too much of the substance available because the brain doesn’t want to overload. With long-term exposure this explains tolerance that the binding sites start to disappear because of how intensely you’re presenting the binding sites in the neurons with these neurotransmitters
All drugs seem to affect the reward or pleasure centres of the brain. People are positively reinforced for using drugs and negatively reinforced when the drugs remove unpleasant experiences such as pain, feeling ill, or anxiety, or result in withdrawal symptoms.
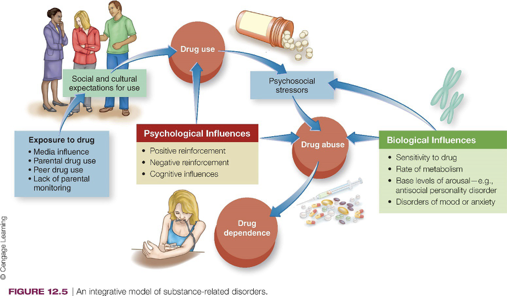
A comprehensive view of substance-related disorder includes both psychological and biological influences.
What are some psychological dimensions
Positive Reinforcement
Psychoactive drugs provide a pleasurable experience
Pleasure, excitement, euphoria
Use increase leads to tolerance increase
As tolerance increases & dependence forms, the long-term impact is not so much through positive reinforcement, it moves from initial positive reinforcement to negative reinforcement
Sometimes drugs are combined to enhance pleasurable experience
For example, individuals who are dependent on heroin sometimes combine it with benzodiazepines (such as Valium) to intensify their pleasure
Negative Reinforcement
Psychoactive drugs provide escape from physical pain (opioids), from stress (alcohol), or from panic and anxiety (benzodiazepines)
Opponent-process theory
Experience an unpleasant crash after being high
So why don’t they just stop taking drugs? One explanation involves an interesting integration of both the positive and negative reinforcement processes
This opponent-process theory holds that an increase in positive feelings will be followed by an increase in negative feelings a short time later. Similarly, an increase in negative feelings will be followed by a period of positive feelings
So a person who has been using a drug for some time will need more of it to achieve the same results (tolerance). At the same time, the negative feelings that follow drug use tend to intensify.
Feels bad to be at your baseline state because the brain has changed and a lot of times you’re also getting negative reinforcement by avoiding problems that are still there, often worsening because you’re getting into trouble by spending too much time & effort & attention, energy money, etc. on the drug
Internally needing more help just to have a regular level of neurotransmitter function and externally getting dependent on this being your coping strategy. You get double pronged negative reinforcement leading to more and more compulsive drug seeking
Cognitive Factors
Expectancy effect: what people expect to experience when they use drugs influences their reaction
How arousal interpreted and channelled
People's experiences when they get intoxicated depend a lot on what they expect. This is that sudden setting thing
If it's supposed to be a holy, spiritual, peaceful experience, the same drug could create wild, uncontrolled, feelings of hallucinations & risk taking if that’s what was expected instead like in a party situation
Expectancies
develop before people actually use drugs
change as people have more experience with drugs
Conditioning; drug cues
Alcohol myopia
As higher cognitive function which is like long-term planning & inhibition and things like that are breaking down. You have something called alcohol myopia
It doesn't just have to be alcohol where things that are immediate seem so important because you can’t conceive counterbalancing by thinking about long-term consequences
That can lead you to focus on immediate rewards & actions that you wouldn’t maybe not do when you think about the longer term effects
Picture someone who is drunk, carefully and methodically placing one foot in front of the other as he or she walks so as not to fall, walking straight into the path of an oncoming truck. Although alcohol myopia may not explain why people drink in the first place, it may help us understand why they continue to drink when they know excessive drinking can have severe negative consequences.
People under the influence of alcohol may not be able to evaluate properly the risks involved in their continued drinking.
What are some social dimensions?
People are exposed to these substances through friends, media
Drug-addicted parents monitor their children less
Because of fixation on drugs affects how present & avaliable for other people.
Less monitoring from parents for kids, leads kids to grow up with perhaps less scaffolding & structure & that makes them perhaps more likely to perpetuate risk-taking behaviours
Moral weakness view
Depending on culture, that getting addicted is a moral weakness and if you are more spiritually strong or pure it wouldn’t happen
Disease model of physiological dependence
People can experience higher or lower levels of intoxication depending on the people around them
Could be calming, inciting or exaggerated presences
According to the moral weakness view, drug use is seen as a failure of self-control in the face of temptation; this is a psychosocial perspective.
The disease model of physiological dependence, in contrast, assumes that drug use disorders are caused by an underlying physiological cause; this is a biological perspective.
What are cultural causes/dimensions?
Cultural norms affect rates of substance use /abuse
Drinking heavily on certain social occasions
May facilitate their misuse
Social pressure for heavy and frequent use
Biological factors may interact with cultural norms
The 4 Types of Triggers
Triggers both internally and externally are going to push us towards substance use
Being around people or in situations where we’re used to using substances makes that more commonly come to mind
Being around peer groups so if you’re trying to get over a substance use disorder & you try to avoid the people and places you associated with substance use
Social triggers are the specific people who either just implicitly because what you do when you are together or explicitly because they push you to drink or smoke or whatever
Emotional triggers is feeling things that you associate with either feeling really good or getting away
Withdrawal triggers: physical dependence. I feel bad inside my body because my body’s used to a certain level of this substance and it’s telling me now im out of balance.

An Integrative Model
Multiple influences interact to account for substance use disorders
These all some together to have this biopsychosocial model
Where cultural and social expectations interact with our own sensitivity and reward learning & then our own ways of coping or reinforcement at the psychological level
Equifinality refers to the fact that a disorder may arise from multiple and different paths, and seems particularly relevant to substance-related problems. Repeated drug use may lead to biological and cognitive reactions that contribute to dependence.
What is the treatment?
With substance use disorders they’re hijacking our motivation system
So treatment begins with motivation.
Substance abusers arrive at treatment at different stages to change substance use behaviour
There's often this idea that someone has to hit rock bottom. They have to come face to face with what it’s costing them to be addicted to the substance in order for them to start to make any sort of upward progress
Focusing first on motivation and what you could have is called motivation interviewing: where you really try to ask people, what is it costing you to be in this disordered state? Is there any reason why you would want to improve things? Do you have dreams or aspirations? What are things you could get if you got out of this state?
Motivational enhancement therapy (MET): increase motivation to change behaviour
MET has been developed to help individuals with substance use disorders increase their motivation to change and move toward a stage where they are ready to work on modifying their problematic substance use.
Need to try different treatments to find the things that fits with that person’s understanding, their capacity, their motivational level is the biggest predictor of success
Treatment plan has to constantly be modified depending on how stressed the person is, what else is happening in their life, have they had recent setbacks
Goal not always abstinence but more controlled use
A specific psychological technique called motivational enhancement therapy (MET) has been developed to help individuals with substance use disorders increase their motivation to change and move toward a stage where they are ready to work on modifying their problematic substance use
Treatment
Substance abusers arrive at treatment at different stages to change substance use behaviour
Motivational enhancement therapy (MET): increase motivation to change behaviour
What are some biological treatments?
Agonist Substitution
Involves providing the person with a safe drug that has a chemical composition similar to the abused drug
Chemical makeup of drug similar to addictive drug
Methadone: opioid agonist; may lead to dependence
Successful when combined with psychotherapy
Buprenorphine: less risk of dependence
Nicotine substitution: gum, patch, inhaler, nasal spray, bupropion
Antagonist Treatment
Involves drugs that block or counteract the positive effects of psychoactive drugs
Naltrexone: opioid antagonist drug
Aversive treatments involve the use of drugs to make the ingestion of abused substances extremely unpleasant
Also given for alcohol dependance
Aversive treatments
Prescribed drugs that make ingesting substances extremely unpleasant
Dissulfiram (Antabuse) used for alcohol disorder
Problem of noncompliance
For smoking aversion: silver nitrate in lozenges or gum
Other Biological treatments
To deal with withdrawal symptoms
Sedatives to minimize discomfort
Desipramine: decreases abstinence rates for cocaine
Other drugs being tested
What are some Psychosocial Treatments?
Impatient Facilities
For initial withdrawal period
Provide support therapy
Expensive
Impatient hospital treatment is expensive & is often used to assist people through the withdrawal stages of substance abuse & to provide supportive therapy so they can return to the community
Alcoholics Anonymous & Its variation
A popular 12 step program that views alcoholism as a disease that people are powerless to overcome without help. Social support key element
Independent from established medical community
Is in more than 170 countries
12-step philosophy Effective with motivated individuals
Cocaine Anonymous and Narcotics Anonymous
Admit you will always be an addict and there is neuroscientific evidence that reward circuitry once it forms into addiction can easily be retriggered but internalize that & identity that I am an addict.
Abstinence focused not just controlled consumption because even a little re-triggers the full cascade of addictive potential
Making amends, apologizing or trying to reach out to people to acknowledge the harms you’ve done, regardless of whether or not they forgive you
Has this religious component to it
What are the factors that led me to get addictive, how can I see those triggers and be aware of them and responsible in the future for my use.
Mentorship program
Controlled Use
Controlled use of a substance instead of abstinence
May be alternative, not a cure
Not every effective over the long-term
Teaching people how to be responsible with their use
We know from this kind of biopsychosocial model that a person who develops a full blown substance use disorder is going to have a lot of trouble finding that happy balance point.
Component Treatment
Covert sensitization: imagining unpleasant scenes
Get person to imagine all the horrible things that are associated with it so don’t have a bunch of positive associations
Same thing used in chronic sex offenses
Individual might be offered a drink of alcohol and receive a painful shock when the glass reaches their lips. The goal is to counteract the positive associations of substance use with negative associations.
The negative associations can also be made by imagining unpleasant scenes in a technique called covert sensitization
Contingency management
Try to get people to change what they use to get pleasure or avoid pain. You try to think of what those triggers are & how to replace some of the things that are more constructive
Here, the clinician and client together select the behaviours that the client needs to change and decide on the reinforcers that will reward reaching certain goals, perhaps money or small retail items like music downloads
Community reinforcement approach
Getting people around you to understand your situation & avoid presenting you with or protect you from triggering situations and offer support
Matching treatment to needs of client
There isn't one evidence base that says one treatment is better than all others. The best research suggests that if you can find out what makes sense to the person, what’s going to work with them and try to use those as your first guesses you have better chance of success

Relapse Prevention
Relapse seen as failure of cognitive and behavioural coping skills
Helping people remove any ambivalence about stopping their drug
Examining their beliefs about the positive aspects of the drug
Harm Reduction & Prevention
Harm Reduction
The harm reduction approach recognizes that substance use occurs in society and seeks to minimize the harm associated with substance use as its primary goal.
Controlled drinking
Legally required bartenders are not allowed to serve you if they think you are too intoxicated
Not going to deal with long-term addiction but stop you from harm
Safe injection sites (SISs)
Prevent downstream effects like disease transmission, violence, unsafe needles
Make as safe as possible
Prevention
Education-based programs
Community-based interventions
Cooperation of governmental, educational, and other social institutions determines success
Prevention efforts have increasingly shifted from education-based approaches to more wide-ranging approaches including changes in the laws regarding drug possession and use, and community-based interventions.
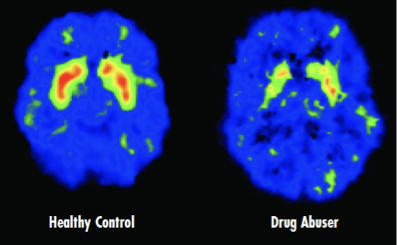
Tolerance for Life’s Pleasures?
Problem that when someone starts using drugs for a long period of time, they’re no longer experiencing pleasure
You can see this is a top down view of the stratum and brain in a PET scan, which measures metabolic activity
The metabolic activity in the striatum is breaking down. You no longer have very many of these red peaks in the long-term meth abuser
Striatum - critical for coding how valuable / rewarding something is…
Dopamine - primary neurotransmitter involved…
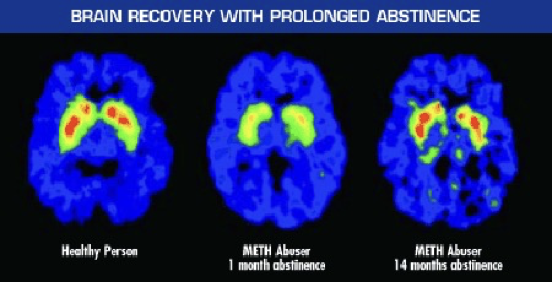
Recovery is Possible
When they become abstinent for a month, they still don’t show any of those red peaks. Their brain reward center not firing like a normal person’s would
It can take up to over a year you can see in right panel. Long time before brain can perceive other types of event inside the body or external events being around other people to have that sense of meaning and pleasure
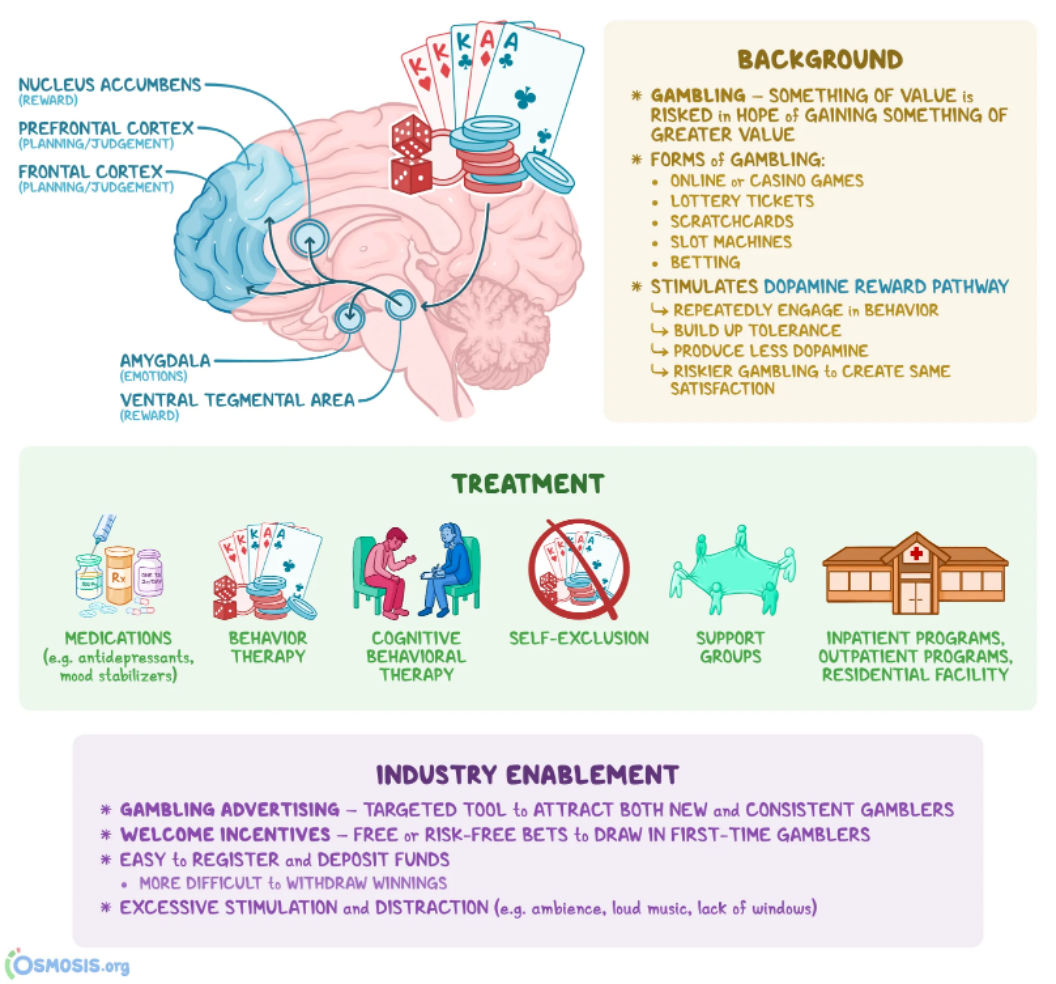
What is Gambling Disorder?
Essentially substance use where a symbol replaces the drug directly getting into your system
Symbol of reward, money becomes addictive substance
Lifetime estimate of approximately 2% Americans
Job loss, bankruptcy, arrests
Similar to substance use disorders
Tolerance and withdrawal
Same patterns of tolerance, get used to certain level of betting. If you really are doing it for excitement you need to bet more and more to have that same level of excitement and feel like nothing else is as exciting as betting
DSM-5: addictive disorders; see DSM-5 Table 12.6
People with gambling disorder: in denial, impulsive, continually optimistic
Internet gambling disorder
High levels of impulsivity
Problem gamblers display the same types of cravings and dependence as individuals who have substance-related disorders.
Similar brain systems appear to be involved with those addicted to gambling as seen in individuals with substance-related disorders.
Gambling Disorder
Same brain system
Its this medial learning reward network pushing us to pay more attention to how we can secure more of those rewards
The way we try to treat people who are stuck in these cycles is in the exact kind of same ways we try to limit the experience of reward, increasing feelings of control maybe with antidepressants, behaviour therapy, talk therapy, avoid triggers, find support groups, maybe even physically removed from situations where you can gamble for periods of time
What are Impulse-Control Disorders?
Intermittent Explosive Disorder: Aggressive impulses resulting in serious assaults, destruction of property
People with intermittent explosive disorder have episodes in which they act on aggressive impulses that result in serious assaults or destruction of property
Lifetime prevalence is 7%
People who have trouble regulating their emotions and end up doing things like punching holes in wall, hitting other people: impulse to have an externalizing behaviour for a strong emotion not controlled
Although it is unfortunately common among the general population to observe aggressive outbursts, when you rule out the influence of other disorders (e.g., antisocial personality disorder, borderline personality disorder, a psychotic disorder, and Alzheimer’s disease) or substance use, this disorder is not often diagnosed.
One concern, among others, is that by validating a general category that covers aggressive behaviour, it may be used as a legal defence for violent crimes.
Cognitive-behavioural interventions (e.g., helping the person identify and avoid triggers for aggressive outbursts) and approaches modelled after drug treatments appear the most effective for these individuals, although few controlled studies yet exist.
Kleptomania: recurrent failure to resist urges to steal things; stigma associated; illegal
More common in women then men, typically starts in adolescence
A person feels a sense of tension just before stealing which is followed by feelings of pleasure or relief when the theft is committed.
People with kleptomania score high on measures of impulsivity, reflecting their inability to judge the immediate gratification of stealing compared with the long-term negative consequences (e.g., arrest, embarrassment
Patients with kleptomania sometimes report having no memory (amnesia) about the act of shoplifting
There appears to be high comorbidity between kleptomania and mood disorders, and to a lesser extent with problematic substance use
Some refer to kleptomania as an “antidepressant” behaviour, or a reaction on the part of some to relieve unpleasant feelings through stealing
Pyromania: having an irresistible urge to set fires
The person feels a tension or arousal before setting a fire and a sense of gratification or relief while the fire burns. These individuals will also be preoccupied with fires and the associated equipment involved in setting and putting out these fires
Pyromania is diagnosed in only about 3 percent of arsonists (Lindberg et al., 2005), because arsonists can include people who set fires for monetary gain or revenge rather than to satisfy a physical or psychological urge
Treatment: Cognitive-behavioural, third wave
They all have this hypersensitivity to reward both socially and genetically endowed
Which leads to uncontrollable, repetitive behaviour which eventually causes distress and dysfunction
Trying to find ways of breaking these cycles
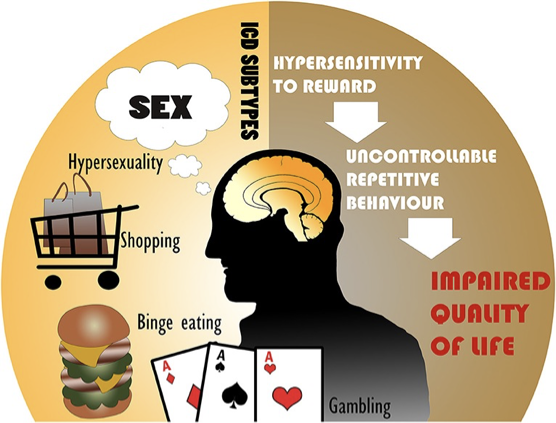
There's all these different risk factors at the biological and social,early development level
Its specifically lack of scaffolding around dealing with reward, dealing with disappointment, turning towards disappointment gratification or pacification or inhibition of negative experiences or stress without being able to sit with negative emotions & try to think constructively about how to move through them or just letting them pass naturally all feed into these kind of impulsivity disorders