Hematologic and Hemostatic Disorders
1/24
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
25 Terms
Mention macrocytic anemias, and normocytic normochromic anemia.
Non megaloblastic anemia
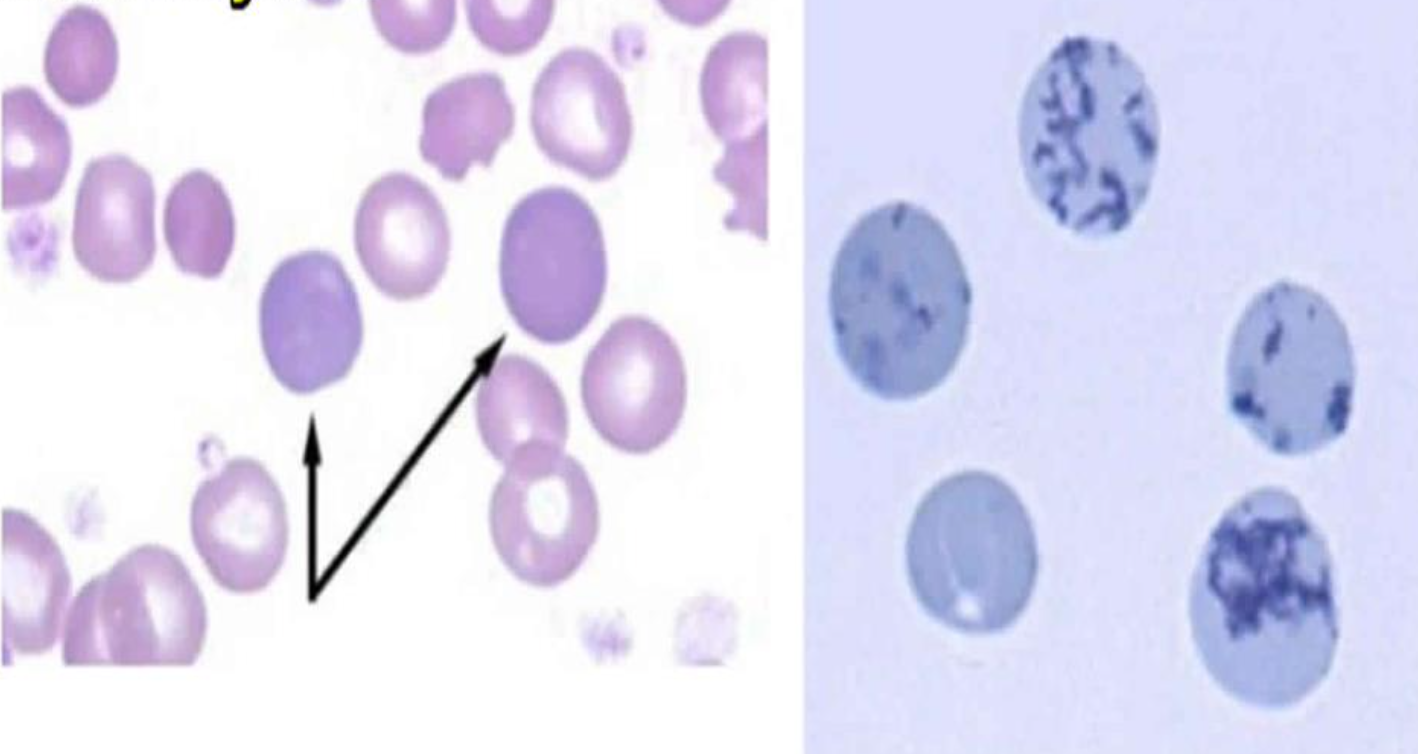
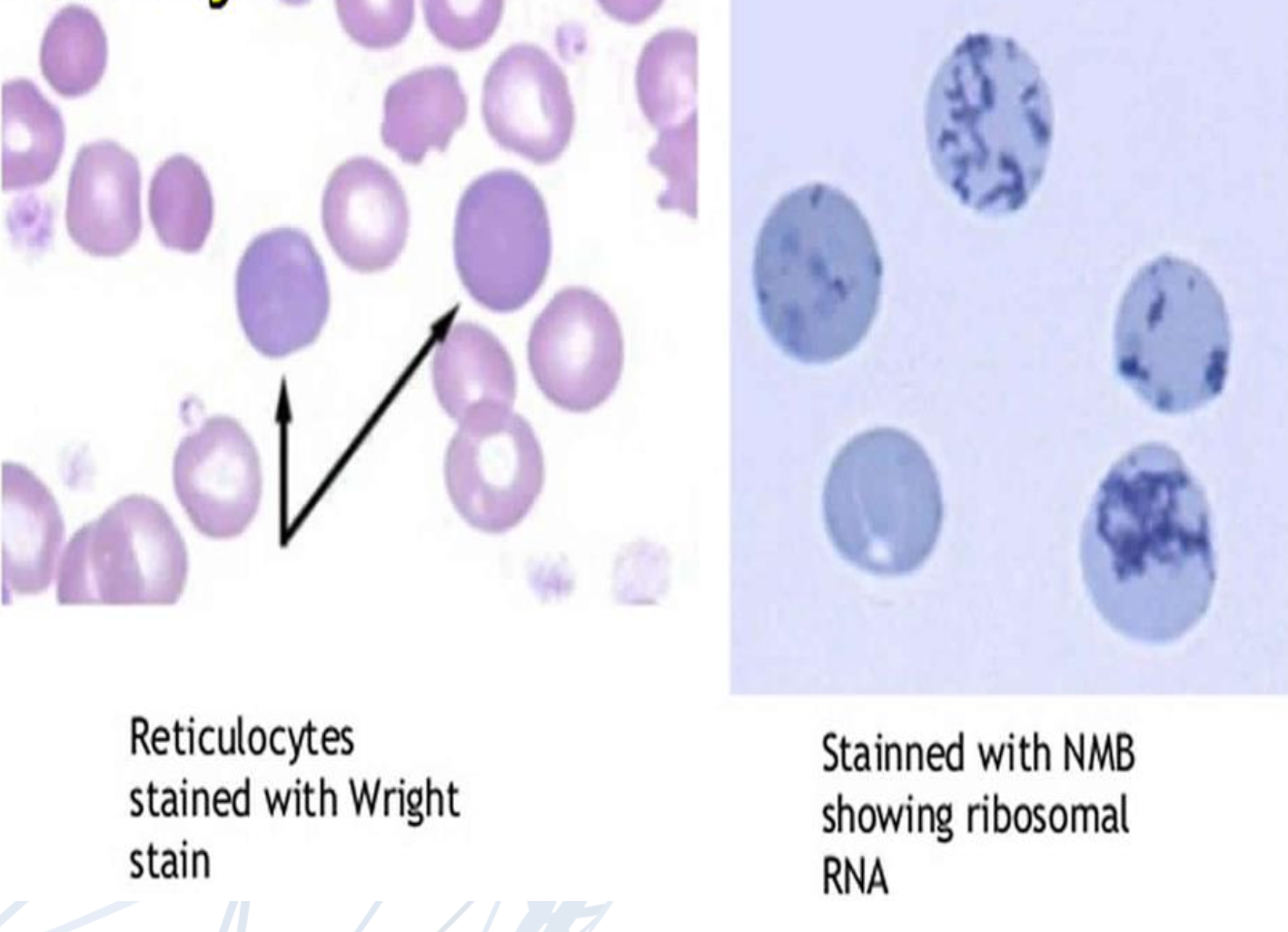
Reticulocytosis
Liver diseases
- Megaloblastic anemia
Vit B12 and folate deficiencyNormocytic Normochromic Anemias:
• Hemorrhage
• Hemolysis:
✓ Intravascular:
• G-6-PD deficiency anemia
• Paroxysmal nocturnal hemoglubinuria
✓ Extravascular:• Hereditary : spherocytosis
• Sickle cellAcquired : AIHA
Mention microcytic hypochromic anemias.
• 1.Iron deficiency anemia
• 2.Thalassemia
• 3.Anemia of chronic illness and could be normo
Mention type of cell present in blood film of iron deficiency anemia.
Pencil Cell
Mention blood and bone marrow findings in megaloblastic anemia.
• Peripheral blood:
•Red Cells:
•Oval macrocytes: earliest sign
• Anisopoikilocytosis
•MCV increases.
•Severe anemia: marked anisopoikilocytosis,
• White blood cells: normal or decreased
•Hypersegmented neutrophils:early sign
•Bone Marrow findings:
• Hyper cellular bone marrow: with erythroid predominance.
Mention causes of aplastic anemia.
✓ Constitutional: Fanconi’s anameia, Dyskeratosis congenital
✓ Acquired : Idiopathic, Drugs, radiation, Infectious diseases, pregnancy.
Mention bone marrow appearance in aplastic anemia.
The characteristic honey comb appearance showing predominance of fat cells and sparse haematopoietic elements
Shperocytosis
Mention clinical presentation of G6PD hemolytic anemia.
– Acute, acquired hemolytic anemia
Associated with exposure to primaquine, sulfa drugs. Sudden development of pallor, jaundice and dark colored urine (due to haemglobinuria ) 1-3 days after exposure to the drug
– Chronic mild hemolytic anemia (common in Africans, Caucasians, as compared to Mediterranean's)
Mention blood film of G6PD anemia.
Peripheral blood examination: general features of haemolytic anaemia: polychromasia, spherocytes, bite cells ( red cells are bitten out margins due to plucking out of the precipitated haemoglobin by splenic macrophages ) and ghost cells ( one half of the red cell appears empty while other half is filled with haemoglobin)
Mention content of granules of platelets.
Alpha granules contain platelet thrombospondin, fibrinogen, fibronectin, platelet factor 4, vWillebrand Factor, platelet derivedgrowth factor, β-thromboglobulin, and coagulation factors V and VIII.
Dense granules contain ADP, adenosine triphosphate (ATP),and serotonin.
Mention coagulation factors inhibitors and mention the first of them to act.
•Tissue factor pathway inhibitor (TFPI) •Antithrombin
•Heparin cofactor II
•α2-Macroglobulin
•α1-antiplasmin
•C1-esterase inhibitor
•α2-antitrypsin
•Protein C
•Protein S
>>> The first inhibitor to act is TFPI which inhibits tissue factor, VIIa and Xa , while the others exert inhibitory effects on circulating serine proteases.
Mention normal values for bleeding tests.
Bleeding time (BT):
Normal value: 1 - 4 min.
Prothrombin time (PT): Normal value: 10 - 14 sec.
(International normalized ratio INR to standardize PT results
among different labs).
Activated partial thromboplastin time APTT: Normal value: 30 - 40 sec.
Thrombin time TT: Normal value: 14 - 16 sec.
Fibrinogen Level
Normal value: 200 to 400 mg/dL (2.0 to 4.0 g/L)
Mention bleeding time sensitivity.
The sensitivity and specificity of the bleeding time for platelet-mediated coagulopathy is low.
Prolonged bleeding times are generally found when : 1.The platelet count is below 50,000/μL.
2.When there is platelet dysfunction.
• Platelet function assay (i.e PFA 100) has largely replaced bleeding time.
Mention causes for isolated prolonged PTT.
Deficiency of FXII, XI, IX, VIII
Lupus Anticoagulant antibodies
Antibodies to FVIII or FIX (i.e. acquired haemophilia)
Unfractionated heparin
Mention use of thrombin time.
Thrombin time is defined as a test that measures the duration required for a clot to form in plasma after adding excess thrombin, evaluating the conversion of soluble fibrinogen to insoluble fibrin.
Clot formation failure within 10–14 seconds may indicate fibrinogen deficiency.
Mention interpretation of prolonged thrombin time.
Congenital Hypofirbinogenaemia
Acquired Hypofirbinogenaemia – eg DIC, Malignancy
Liver disease
Following thrombolysis
Direct Thrombin inhibitors (eg dabigatran)
Mention vascular system disorders for bleeding.
Hereditary:
1.Hereditary hemorrhagic telangiectasia (Osler–Rendu–Weber syndrome)
2.Connective Tissue Disorder: Ehlers–Danlos syndrome
Acquired:
a) Anaphylactoid purpura b) Infections
c) Scurvy
d) Senile purpura
e) Purpura simplex
f) Mechanical purpura
g) Drugs, e.g. corticosteroids h) Cushing’s syndrome
Mention diagnosis of vascular disorders of bleeding.
• Platelet count : normal
• Bleeding time: usually normal
• PT/PTT/TT: Normal
• Platelet function: normal
• Hess test: > 15 purpuric spots
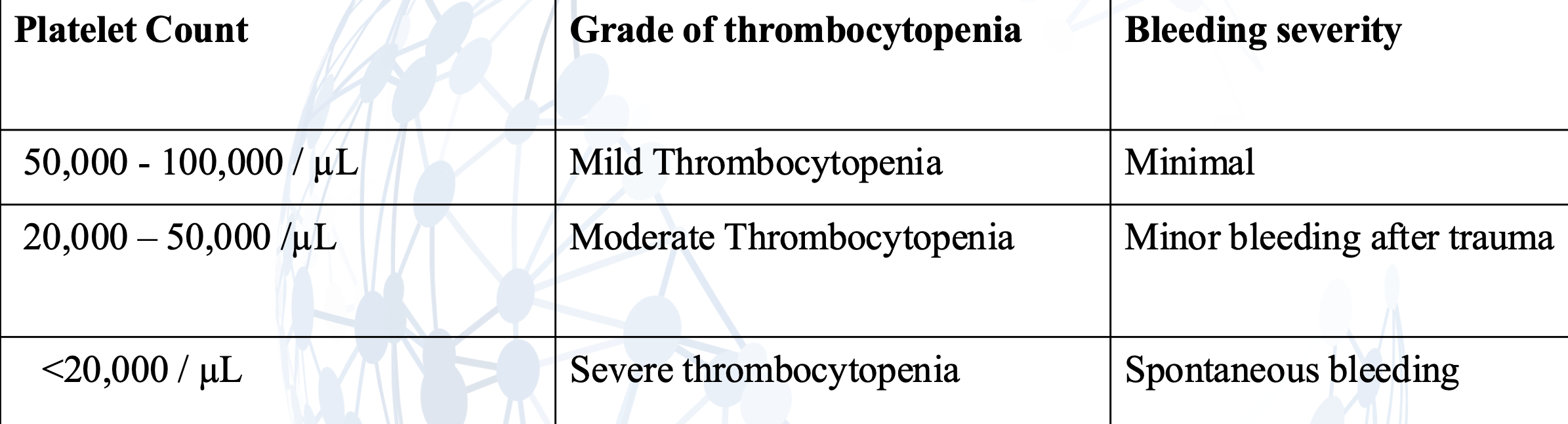
Mention different bleeding risks depending on trauma.
Mention qualitative platelete disorders.
Hereditary:
- Thrombasthenia (Glanzmann’s disease)
- Bernard-Soulier syndrome
- Storage pool disease
- Von Willebrand disease vWD
Acquired:
- Anti-platelet drugs
- Hyperglobulinemia
- Myeloproliferative neoplasia MPN
- Myelodysplastic syndrome MDS
- Uremia
What is the most common hereditary hemorrhagic disorder?
Hemophilia
Mention value of d-dimer and fibrin degradation products in cirrhosis.
Normal D-dimer but increased FDPs
Mention lab findings in DIC.
• Low platelets count with Schistocytes (fragmented red cells) on blood smear.
• Prolonged bleeding time
• Prolonged PT
• Prolonged APTT
•Prolonged Thrombin time
• Low fibrinogen
• Low plasma levels of coagulation inhibitors: ATIII or protein C.
• FDP and D-dimer: Increased
Mention monitoring anticoagulant therapy.
1. Heparin therapy monitored by : APTT:
- It must be given in a dose sufficient to prolong PTT 1.5-2.5 times the
upper limit of normal values.
- APTT should be checked 4-6 hours after administration of heparin or
a change in the infusion rate.
2. Oral anticoagulant ( Warfarin) therapy: by PT:
- Recommended therapeutic range of INR= 2.0-3.0 in DVT,
pulmonary embolism, Atrial fibrillation, inherited thrombophilia or
acute myocardial infarction.
- Recommended therapeutic range of INR= 2.5-3.5 in recurrent
embolism, mechanical prosthetic heart valves & anti-phospholipid syndrome.
3. LMWH (CLEXAN): monitored by anti factor X activity.