NPTE Full Study Guide
1/398
Earn XP
Description and Tags
Lord Help Us
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
399 Terms
Normal Value Adult Blood Pressure
<120/80 mmHg
Elevated 121-129/<80
Stage 1 Hypertension: 130-139/80-89
Stage 2 Hypertension >= 140/90
Hypertensive crisis > 180/120
Normal Value Adult Heart Rate
60- 100 bpm
Tachycardia >100bpm
Bradycardia < 60 bpm
Normal Value Adult Respiratory Rate
12-20 breaths/min
Normal Value Adult Oxygen Saturation
> 95%
Normal Value Adult Temperature
98.6 degrees F (37 degrees C)
Normal Value Pediatric Blood Pressure
Newborn: 60–80/40–50 mmHg;
Infant (1–12 mo): 70–100/50–70;
Child (1–10 yr): 90–110/55–75 mmHg
Normal Value Pediatric Heart Rate
Newborn: 120–160 bpm;
Infant: 100–160;
Child (1–10 yr): 70–120 bpm
Normal Value Pediatric Respiratory Rate
Newborn: 30–60 breaths/min;
Infant: 20–40;
Child (1–10 yr): 18–30 breaths/min
Normal Value Cardiac Output
4-8 L/min
Normal Value Ejection Fraction
55-70%
SV/EDV * 100= EF, Quantity of blood ejected during each heart beat.
Normal Value Central Venous Pressure
0-8 mmHg
Normal Value Right Atrial Pressure
2-6 mmHg
Normal Value R Ventricular Pressure
15-30 mmHg (systolic)
Normal Value Pulmonary Artery Pressure
8-20 mmHg
Normal Value Pulmonary Capillary Wedge pressure
4-12 mmHg
Estimates left atrial pressure = estimates how well the left heart is moving. Higher wedge pressure indicative (potentially) of Left heart failure.
Normal Value Maximum Inspiratory Pressure
>80 cmH2O
Max pressure generated during inspiration. Related to strength of the diaphragm and other inspiratory muscles.
Normal Value Maximum Expiratory Pressure
1.5 * MIP ( >120 cmH2O)
Max pressure generated during expiration. Evaluates strength of expiratory muscles.
Normal Value Mean Arterial Pressure
70-110 mmHg
Normal Value Rate Pressure Product
> 20,000 mmHg/min
Rough estimate off myocardial oxygen demand. Higher RPP= higher workload on the heart = at risk for angina or risk of MI. May occur with heart disease or during exercise.
Normal Value Cardiac Index
2.6-4.24 L/min/m²
Cardiac output based on body size. Most accurate assessment of heart’s ability to perfuse based on patient size. Low= poor perfusion. Below 2.0= activity contraindication
Normal Value Electrocardiogram P-R Interval
0.12-0.20 seconds
Normal Value Electrocardiogram QRS Complex
0.08-0.10 seconds
Normal Value Electrocardiogram Intracranial Pressure
< 15 mmHg
Ankle Brachial Index
Values:
>1.4 Calcified arteries
1.0-1.4 Normal
0.8-1.0 Mild PAD - Compression for edema is safe to use
0.5-0.8 Moderate PAD - Intermittent claudication, use modified compression or none if <0.6
<0.5 Severe PAD - Severe ischemia with resting pain, compression is always contraindicated.
Gold standard test for Peripheral Artery Disease (PAD). Formula= Systolic(ankle)/Systolic(brachial).
Electrocardiogram
Evaluates cardiac electrical activity, rhythm, rate, and conduction.
Common indications: Arrhythmias, ischemia, myocardial infarction, electrolyte imbalances.
Key findings:
HR and rhythm (sinus rhythm vs arrhythmias), PR interval (AV conduction), QRS duration (ventricular conduction), ST segment (ischemia/infarction), QT interval (risk of ventricular arrythmias).
Normal Values Diaphragmatic Excursion
3-5 cm
The diaphragmatic excursion test measures the movement of the diaphragm, typically 3–5 cm in healthy adults, by percussing the posterior chest at maximal inhalation and exhalation. Reduced movement (< 3 cm) suggests pathology like COPD, paralysis, or pleural effusion
Obstructive Disorders (5). Name and include structures damaged
A- Asthma: Inflammation/swelling of bronchial lining and bronchoconstriction
B- Bronchiectasis: Permanent dilation and thickening of airways due to chronic infection/inflammation. Heavy mucus retention.
C- Chronic Bronchitis: Chronic inflammation, swelling of the airway lining, and increased mucus production.
C- Cystic Fibrosis- Genetic defect causes production of thick, sticky mucus that clogs the airways. (chronic health issues ex: hypoxemia)
E- Emphysema: Destruction of the alveolar walls and loss of elasticity.
COPD = Chronic bronchitis + Emphysema
MET Levels
One MET is the amount of energy your body uses each minute while resting quietly. This increases with activity.
Light activities <3 MET’s are good for elderly persons and those with physical limitations.
Moderate activities (3-6 Mets) Best for people wanting a moderate exercise program.
Vigorous activities (>6 Mets) Best for those with high fitness level and in good health.
Light activates- (Sitting quietly, Walking, Stretching)
Moderate activities -(Archery, Dance, Surfing)
Vigorous activities - (Backpacking, Hockey, Running 7 min/mile)
How do you determine Obstruction vs Restriction?
Obstruction: Low FEV1 or FVC and FEV1/FVC ratio (<80%). RV is high (>120%).
For reversible: +12% or 200mL change post bronchodilator/spirometer
If DLCO <60% = emphysema, if DLCO high >60% = asthma
Restriction: Low TLC (<80%), normal RV, FEV1 and FVC.
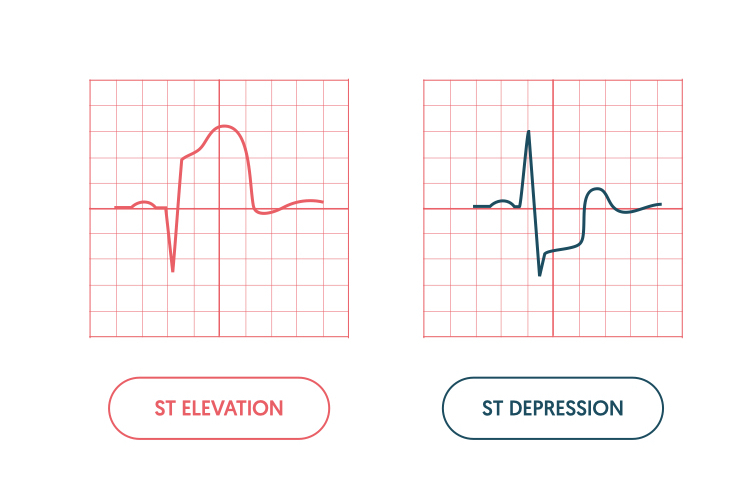
Myocardial ischemia vs infarction. Describe difference and what you see clinically (ECG)
Myocardial infarction: Seen as ST elevation (STEMI) or elevated troponin levels with inverted t-wave/ST depression and pathological Q’s (NSTEMI). Non reversible and treatment must be adjusted/monitored carefully.
STEMI = total arterial blockage, NSTEMI= partial
Myocardial ischemia: Seen as T-wave inversion or ST segment depression. Reversible- ECG readings should return to normal over time. Less contraindications for therapy.
Signs and Symptoms Right Heart Failure
3 Main signs:
Jugular Venous Distention, Ascites/hepatoportal hypertension/liver congestion, and bilateral lower extremity edema
Symptoms: Dyspnea on exertion and decreased exercise tolerance.
Signs and Symptoms Left Heart Failure
Signs and symptoms:
Orthopnea, cardiac arrhythmias, dyspnea on exertion.
Caused by systemic hypertension or CAD.
What is the difference between myocardial ischemia and heart failure?
Myocardial Ischemia- Supply-demand mismatch where reduced blood flow causes O2 shortage in the heart muscle causing pain (angina) and damage.
Heart Failure- Chronic condition where heart can not pump blood efficiently to meet body demands.
Ischemia=cause, HF= result
Postural Drainage Position Apical Segments
Patient positioned in long sitting with two pillows under knees. Percussion/shaking/vibration on apical segment (above clavicle on mid-clavicular line).
Postural Drainage Position Anterior Segments
Patient supine with 2 pillows under knees. Percussion/shaking/vibration (P/S/V) on mid-clavicular line at the level of 1st-4th ribs.
Postural Drainage Position Superior/Inferior Lingual Segments
Patient in supine on wedge feet elevated 12-15” with 1 pillow on left back to induce ¾ rotation elevating the left side and 1 pillow under knees. Percussion on left lateral chest wall slightly anterior to mid-axillary line at 3rd-5th intercostal spaces.
Postural Drainage Position Medial/lateral Segments
Patient in supine with feet elevated 12-15” with 1 pillow behind back and 2 pillow under the knees. Percussion on right lateral chest wall on mid-axillary line at ribs 4-6.
Postural Drainage Position Anterior Basal Segments
Patient in supine positioned with legs elevated to 18” and 2 pillows under the knees. Percussion anterior to mid-axillary line at level of ribs 6-8.
Postural Drainage Position Posterior Basal Segments
Patient in prone with legs elevated to 18” and 2 pillows under the hips. Percussion below inferior border of scapula.
Postural Drainage Position Lateral Basal Segments
Patient in side-lying with feet elevated to 18” and 1 pillow under head and between legs. Percussion on lateral chest wall at 7th to 10th ribs along mid-axillary line.
Postural Drainage Position Superior Segment (LL)
Patient in prone with 2 pillows under hips. Percussion medial to medial border of the scapula.
Postural Drainage Position Right Posterior Segment (UL)
Patient in prone with pillow under right chest elevating right side to ¾ rotation. Percussion above scapula on mid-clavicular line.
Postural Drainage Position Left Posterior Segment (UL)
Patient positioned in prone with table set to 45 degrees with 1 pillow under hips for ¾ rotation on left side. Percussion above scapula along mid-clavicular line.
Patient presents with the following lab values:
PH: 7.37
PaCO2: 47 mmHg
HCO3: 29 mEq/L
Compensated Respiratory Acidosis
Patient presents with the following lab values:
PH: 7.47
PaCO2: 35 mmHg
HCO3: 32 mEq/L
Uncompensated Metabolic Alkalosis
Patient presents with the following lab values:
PH: 7.39
PaCO2: 32 mmHg
HCO3: 20 mEq/L
Compensated Metabolic Acidosis
Patient presents with the following lab values:
PH: 7.46
PaCO2: 30 mmHg
HCO3: 22 mEq/L
Compensated Respiratory Alkalosis
Diaphragmatic Breathing test and purpose
Have patient place one hand on chest and other on stomach. Instruct to take a deep breath and raise just the hand on the stomach. If needing further help instruct to “sniff”.
This test works on diaphragm activation for inhalation.
Paced breathing test and purpose
Instruct patient to in for 3 seconds and out for 3 seconds (range of time varies 2-4 sec).
Helps lower anxiety and has a calming effect.
Pursed-Lip Breathing test and purpose
Place hand on patient abdominals to ensure no contraction takes place. Instruct patient to breathe deeply in through the nose, make a loose “O'“ with their mouth as they exhale slowly.
Creates a back pressure allowing for more effective exhalation for individuals with obstructive disorders.
Segmental breathing with inspiratory hold technique test and purpose.
Place hands over specific bronchopulmonary segment and instruct patient to breathe into it pushing your hand away. At max inhalation have them hold for 3 seconds before exhaling. During exhalation push down on the segment applying a high-velocity low-amplitude PNF stretch at the end.
Promotes diffusion to specific segment.
Stacked Breathing
Instruct patient to take small-moderate breaths without exhaling until hitting maximum inspiration.
For patients with restrictive issue, bad ventilation, or difficulty with deep breathing due to muscular weakness.
Counter-rotation test and purpose
Patient side-lying, place one hand on scapula and other on ASIS. Have patient breathe in as you push with scapular hand and pull with ASIS hand. Instruct them to exhale as you pull with scapular hand and push with ASIS hand. Do not pull spine past neutral and stay off glenohumeral joint.
Mobilizes a tight chest increasing tidal volumes and requires no active participation on the part of the patient.
Active Cycle of Breathing Purpose
Effective for secretion drainage.
Coughing vs Huff techniques for Secretion Clearance
Coughing techniques- Voluntary coughing, prone on elbows, Long-sitting paraplegia butterfly, Wheelchair paraplegia butterfly, hands and knees rocking.
Huff techniques- Long-sitting quadriplegia and wheelchair hook-arm quadriplegia
Techniques involve looking up and breathing in and then looking down and breathing out for 3-5 reps before “throwing” head/arms down and coughing for airway clearance.
Coughing vs Huff activity indications
Huff is ideal for patients with asthma, reactive airways, or lack of muscle control to cough effectively.
Cough works better for everyone else.
Huff technique and Forced Expiratory Technique
Instruct patient to breath out warm air as if fogging a pair of glasses.
FET- medium breath 2 huffs, then small breath two huffs, and repeat.
Splinting technique
Instruct patient to tightly hold pillow over incision cite then take a deep breath in and cough.
Heimlich Maneuver test
For a choking individual, stand behind individual and administer 5 abdominal thrusts under the xiphoid process, then 5 back blows. Repeat until object can be clearly seen and swept from throat.
For pregnant women administer 5 chest thrusts instead.
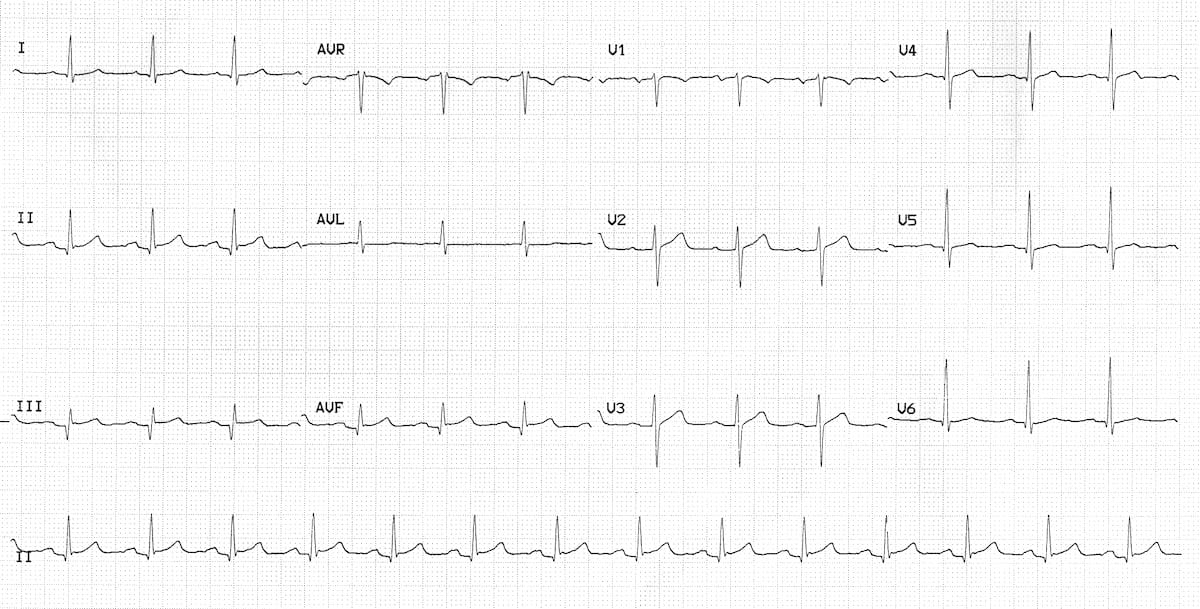
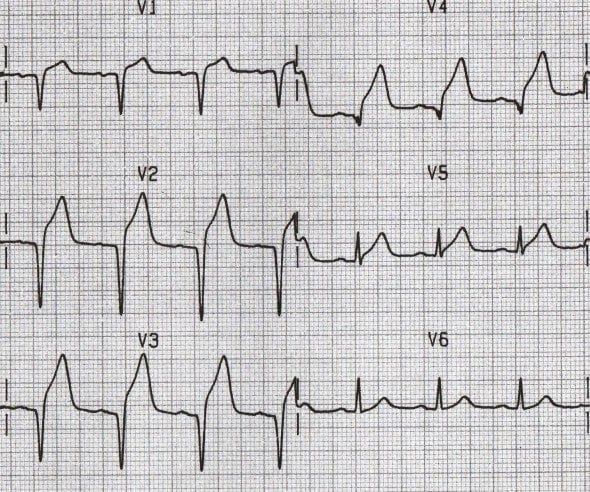
Patient presents with the following ECG and a troponin value of 0.24 ng/ml. What is the diagnosis?
NSTEMI
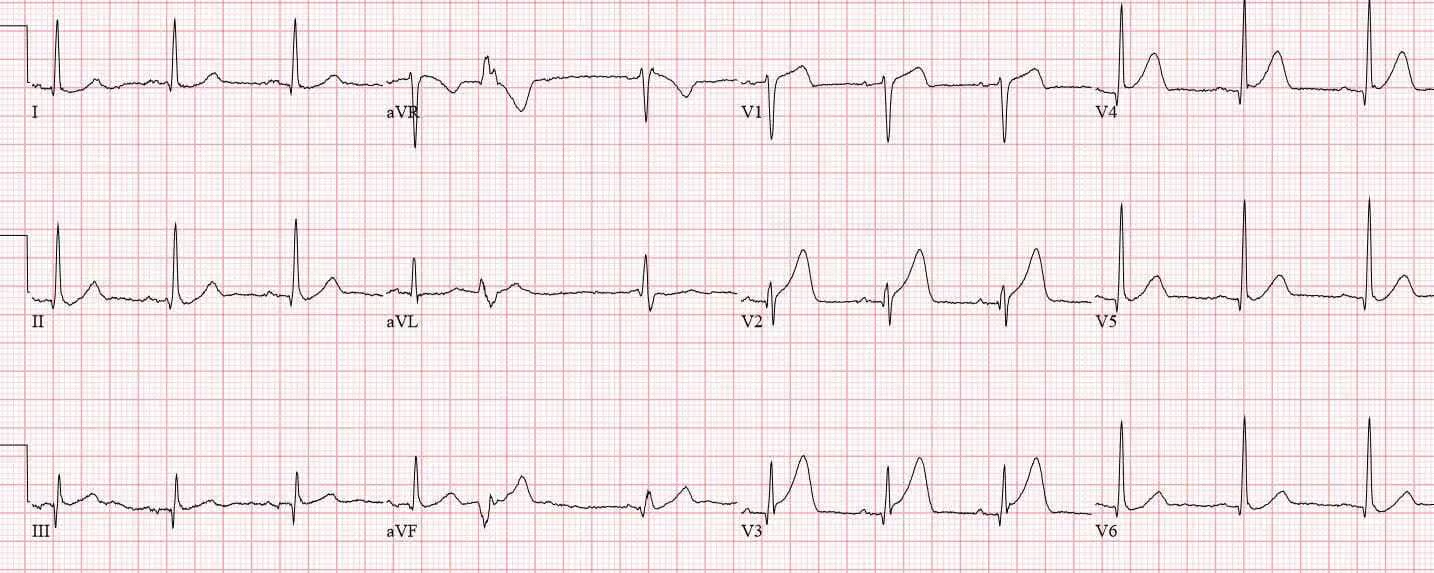
Patient presents with the following ECG. What is the diagnosis?
STEMI
What extra test is needed to identify NSTEMI
Troponin Values
List out most common Congenital Heart Defects that are Acyanotic and what their effects/clinical implications are.
Ventricular Septal Defect (Hole in Septum between ventricular heart chambers)
Atrial Septal Defect (Hole in Septum between L and R atria)
Patent Ductus Arteriosus (Vessel btw. pulmonary artery and aorta remains open after birth.)
Left→Right Shunt= Oxygenated blood into right heart= increased workload on right ventricle= hypertrophy and stiffening of R ventricle.
Clinically: Mild to small effects, exercise is generally tolerated well.
List out most common Congenital Heart Defects that are Cyanotic and what their effects/clinical implications are.
Tetralogy of Fallot (Pulmonary Aorta and Aortic Arch are switched)
Transposition of the Great Arteries (Aorta and Pulmonary artery reversed)
Tricuspid Atresia (Tricuspid fails to develop properly)
Right→Left shunt= Unoxygenated blood to left heart= chronic hypoxemia
Clinically Severe limitation in exercise
Cardiac Output Equation
SV * HR = CO
Inverse relationship between SV and HR, Low CO = Hypoxemia/heart failure/shock
Rate Pressure Product Equation
HR * Systolic Blood Pressure
Rough estimate off myocardial oxygen demand. Higher RPP= higher workload on the heart = at risk for angina or risk of MI. May occur with heart disease or during exercise.
Mean Arterial Pressure Equation
Formula: DBP + 1/3(SBP - DBP)
Average pressure in arteries during 1 cardiac cycle. Helps to evaluate tissue perfusion. < 60 mmHg = activity contraindication. 60-70 mmHg minimum to enable perfusion to vital organs. Low MAP = Hypertension or shock.
Equation for Calculation of Oxygen in E cylinder
0.28(Cylinder Pressure-500)/ Flow Rate(L)
Patient is on 4L of O2 with a cylindrical pressure of 1750PSI and a 30 minute walk home. What is the total number of minutes you can work with them?
57 minutes and 30 seconds
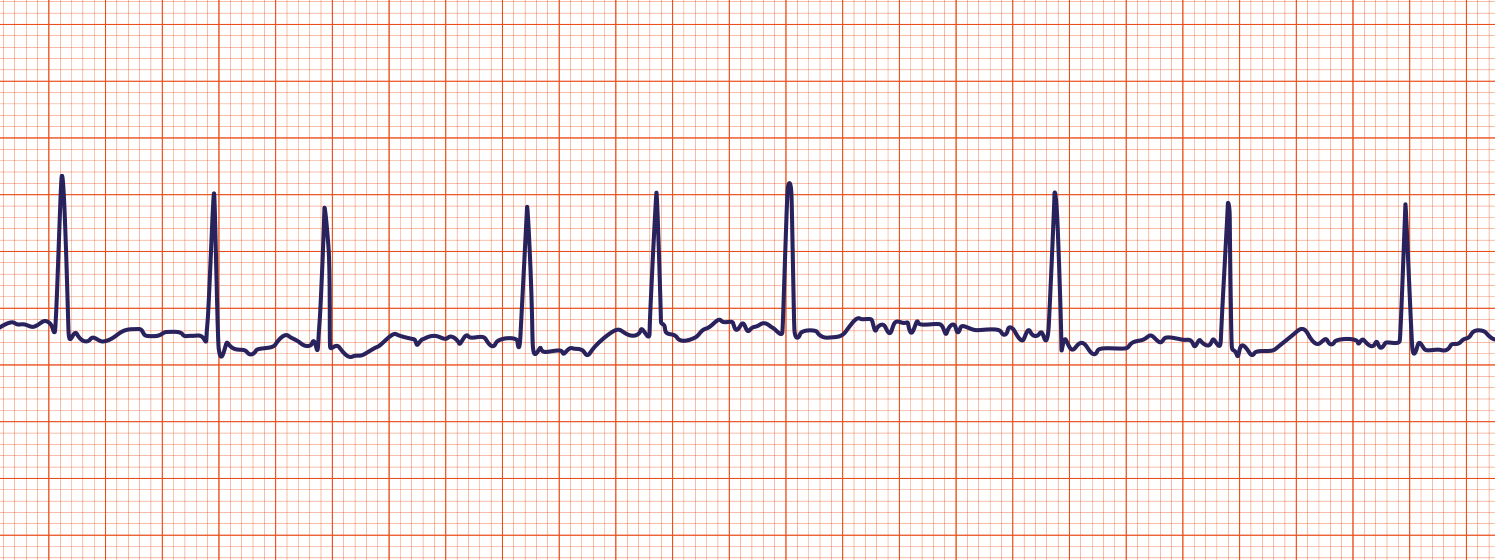
What pathology is shown on the ECG? What are the defining characteristics?
Atrial Fibrillation
Irregularly Irregular, no distinguishable P-waves

What pathology is shown on the ECG? What are the defining characteristics?
Atrial Flutter
Jagged “sawtooth” like P-waves.
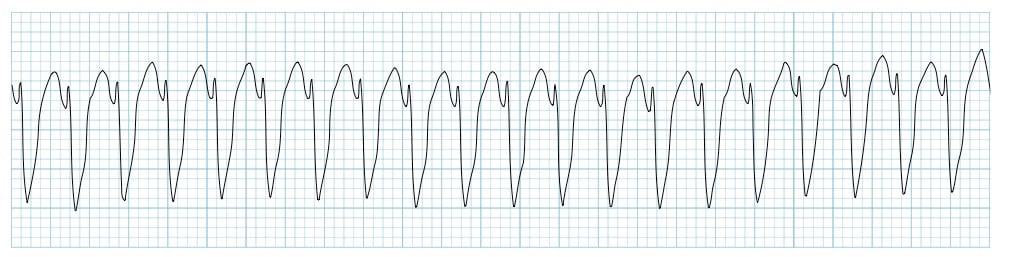
What pathology is shown on the ECG? What are the defining characteristics?
Ventricular Tachycardia
QRS complex is abnormal with a single ectopic focus (look the same). Can lead to V fib.

What pathology is shown on the ECG? What are the defining characteristics?
1st Degree Heart Block
Prolonged PR Interval

What pathology is shown on the ECG? What are the defining characteristics?
2nd degree heart block Type I (Mobitz I)
PR interval increases in length each beat then a beat is skipped. Longer-longer-drop=Weinkebach

What pathology is shown on the ECG? What are the defining characteristics?
2nd Degree Type II (Mobitz II)
Multiple P-waves before every QRS complex.

What pathology is shown on the ECG? What are the defining characteristics?
3rd Degree Heart Block
Multiple P waves before every QRS. QRS complexes are wide. Bridge is out btw atria and ventricle.

What pathology is shown on the ECG? What are the defining characteristics?
Torsades de Pointes
Undulating waveform. Due to electrolyte imbalance (magnesium)
What pathology is shown on the ECG? What are the defining characteristics?
Significant Q’s
Q> 1 small box, depth of 1/4th the height of following R, abnormally tall QRS complex
Irreversible damage: fingerprint on ECG shows MI happened in the past.

What pathology is shown on the ECG? What are the defining characteristics? What is another way to identify this pathology?
Bundle Branch Block
“Rabbit ears” or abnormally shaped “R” on the QRS complex
What 2 pathologies are shown on the ECG? What is the difference between them?
STEMI = Non reversible, tissue death
Myocardial ischemia = Reversible, impaired blood flow
Blood pressure Response to Exercise Absolute Contraindications to Continue Activity
SBP drops >/= 10mmHg from baseline with increased workload
SBP >/= 250mmHg
DBP >/= 115 mmHg
Failure of SBP to rise with increased workload.
Blood pressure Response to Exercise Normal SBP and DBP
SBP: Increases about 10mmHg per MET or stage of exercise intensity. Peak at 160-220mmHg in health adults
DBP: Unchanged or decreases slightly (</= 10mmHg drop is normal)
Orthostatic Hypotension- What Vital Signs are seen?
Drop in Systolic BP >/= 20mmHg or Diastolic BP >/= 10mmHg
Occurs within 3 min of standing (after supine/sitting for 5 min)
HR increases (compensatory tachycardia)
Accompanied by dizziness, lightheadedness, near-syncope
Tracheal Deviation- Chest Exam
Assessed by palpation in the suprasternal notch (compare space bilaterally)
Normal: Trachea is midline
Tracheal deviation away from injured site (list pathologies)
Pleural effusion
Space Occupying Tumor
Pneumothorax
Tracheal deviation towards injured site (list pathologies)
Atelectasis
Excursion- Chest Exam: Describe the test and what it measures.
Assesses chest wall and diaphragmatic movement/expansion during deep breathing
Normal thoracic excursion: Symmetric bilateral chest wall expansion ≥3 cm
Abnormal (reduced or asymmetric): Pleural effusion, pneumothorax, atelectasis, pulmonary fibrosis, diaphragmatic paralysis/weakness, or pain/guarding
Fremitus- Chest Exam: Describe the test and what it measures.
Tactile (vocal) fremitus: Palpate symmetric chest wall (ulnar border or palms) while patient repeats “99” or “blue moon” in a deep voice
Normal: Symmetric bilaterally; stronger over large airways/upper lobes, decreases toward periphery
Increased fremitus: Lung consolidation (pneumonia, atelectasis with patent bronchus) – vibrations transmit better through solid tissue
Decreased or absent fremitus: Pleural effusion, pneumothorax, emphysema/COPD (air trapping), bronchial obstruction, or thick chest wall/obesity
Egophony - Chest exam
Patient says “Eeee” – Normal: muffled “E”; Positive: sounds like nasal “Aaa” (E-to-A change)
Positive in all three = lung consolidation (pneumonia, atelectasis with patent bronchus)
All three decreased/absent with pleural effusion, pneumothorax, or emphysema
Bronchophony- Chest Exam
Bronchophony: Patient says “99” – Normal: muffled/indistinct; Positive: words heard louder & clearer
Positive in all three = lung consolidation (pneumonia, atelectasis with patent bronchus)
All three decreased/absent with pleural effusion, pneumothorax, or emphysema
Whispered Pectoriloquy- Chest Exam
Patient whispers “1-2-3” or “99” – Normal: faint or inaudible; Positive: whispered words heard clearly & distinctly
Positive in all three = lung consolidation (pneumonia, atelectasis with patent bronchus)
All three decreased/absent with pleural effusion, pneumothorax, or emphysema
Mediate Percussion- Chest Exam
Place middle finger of non-dominant hand flat & firm on intercostal space; strike distal interphalangeal joint with tip of dominant middle finger using quick wrist motion
Normal: Resonant (low-pitched, hollow) sound over air-filled lung tissue; symmetric bilaterally
Dullness (flat sound): Increased density (pleural effusion, consolidation/pneumonia, atelectasis, tumor, or fibrosis)
Hyperresonance (boomier/louder): Excess air (pneumothorax, emphysema, asthma, or large bullae)
Heart Sound Auscultation- Name the location of the 4 valves for auscultation
Auscultate in 4 areas (patient supine/sitting):
Aortic (2nd R ICS),
Pulmonic (2nd L ICS),
Tricuspid (4th–5th L ICS),
Mitral/Apex (5th L ICS midclavicular)
Heart Sound S1
“Lub” contracting of ventricles. Semilunar valves open and AV valves closed.
Normal heart sound.
Heart Sound 2
“Dub” relaxing of ventricles. Semilunar valves closed and AV valves opened
Normal heart sound.
Heart Sound S3- Describe the sound, its cause, and the effect.
(ventricular gallop): Low-pitched early diastolic sound (rapid ventricular filling);
normal in children/young adults/pregnant/athletes;
pathologic in adults >40 (heart failure, volume overload)
A sign of Chronic Heart Failure.
Heart Sound S4- Describe the sound, its cause, and the effect.
(atrial gallop) Low-pitched late diastolic sound (atrial contraction into stiff ventricle);
always pathologic (ventricular hypertrophy, ischemia, hypertension, aortic stenosis)
Sign of stiff left ventricle often due to systemic hypertension.
Vesicular Breath Sounds
Soft, low-pitched; inspiration > expiration (3:1 ratio); heard over most peripheral lung fields (normal)
Bronchial Breath Sounds
(Tracheal): Loud, high-pitched; expiration > inspiration; heard over trachea & large airways (Normal)
Abnormal when heard over peripheral lung fields.