Sys Path FINAL
1/2099
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
2100 Terms
bone matrix consists of what 2 components?
osteoid (organic)
hydroxyapeptite (inorganic)
osteoblast
produces osteoid and line trabeculae
when osteoblasts are highly active, what increases in the blood?
ALP
osteocyte
osteoblast that resides in lacunae surrounded by matrix and sense bone loading
osteoclast
macrophage type cell that resorbs bone via acidic enzymes
cortical bone features:
dense
longitudinal osteons
concentric lamellae around central blood vessel
trabecular bone features:
no osteons
lamellae parallel to surface
woven bone features:
rapid ± reactive growth
no lamellae or osteons
irregular lacunae and collagen
weak bone later replaced by lamellar bone
periosteum covers what parts of bone?
everywhere but articular surfaces plus tendon insertions
periosteum layers:
outer fibrous
inner cambium
where is the primary ossification center of bone?
at diaphysis and extends into metaphysis
where is the secondary ossification center of bone?
epiphysis
physis (growth plate)
band of cartilage between primary and secondary ossification centers until maturity
what are the 3 zones of the physis?
reserve
proliferative
hypertrophic
how does cartilage at physis become metaphyseal bone?
as cartilage hypertrophies, matrix gets mineralized
capillaries invade with osteoblasts, which deposit osteoid on mineralized cartilage (primary spongiosa)
later cartilage removed (secondary spongiosa)
what species has very late physeal closure?
sheep
what 2 major factors affect deposition and resorption of bone?
demand for minerals
mechanical forces
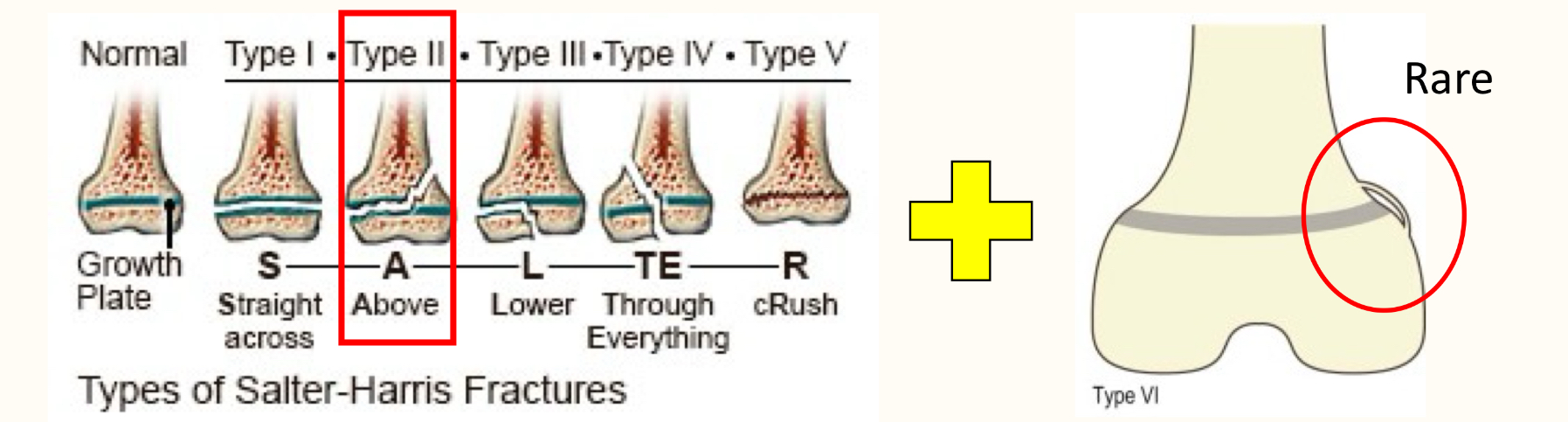
fracture classifications:
simple vs comminuted
impacted (one fragment in another)
compound (open)
greenstick (intact periosteum with minimal fragment separation)
avulsion (excess traction on tendon or ligament tears off piece of bone)
microfractures (tiny fractures of trabecular or cortical bone)
infraction (multiple microfractures together)
stress fracture
combining stress related cortical microfractures
salter harris fracture classification:
fractures of physis
fracture repair timeline:
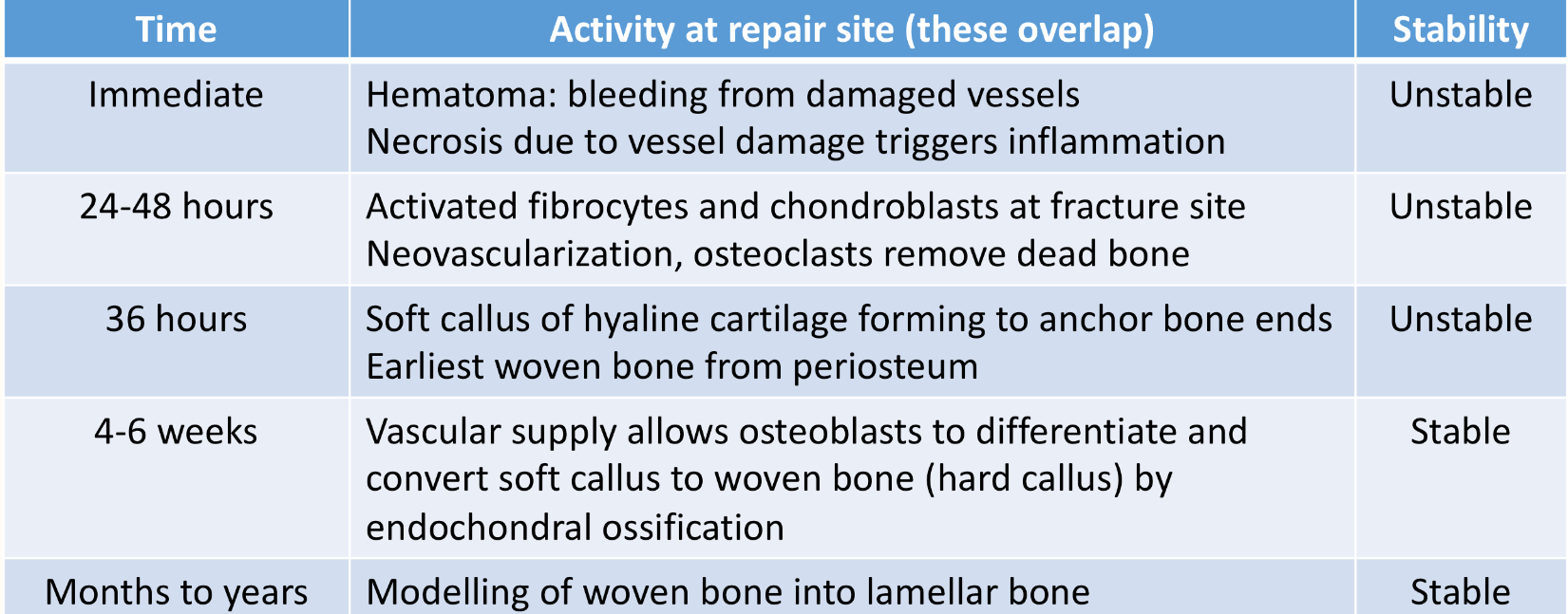
perfect fracture realignment speeds/slows healing
slows
fracture repair complications:
large fragments of necrotic bone interfere with healing
infection
excess movement and displacement can result in pseudoarthrosis (false joint)
angular limb deformity due to physis damage pathogenesis:
one side of physis is detroyed and other side keep growing and bending toward damaged side
valgus
lateral deviation of distal joint
varus
medial deviation of distal joint
causes of bone necrosis:
trauma
neoplasia
inflammation
embolism
sequestra
large fragments of necrotic bone
outcomes for necrotic bone:
osteoclasts resorb it in areas that have blood flow
bone can heal with some dead bone
pyogenic infections lead to sequestra
separates from viable tissue and forms sequestra
involucrum
granulation tissue wall that forms to wall off sequestrum
legg-calve-perthes disease
avascular necrosis of femoral head due to delayed incorporation of blood vessels into bone channels
spina bifida
failure of dorsal midline closure
what are the main causes of generalized skeletal dysplasia?
cartilage defects
bone matrix problems
bone remodeling defects
achondroplasia
absence of cartilage development
chondrodysplasia
disorder of cartilage development
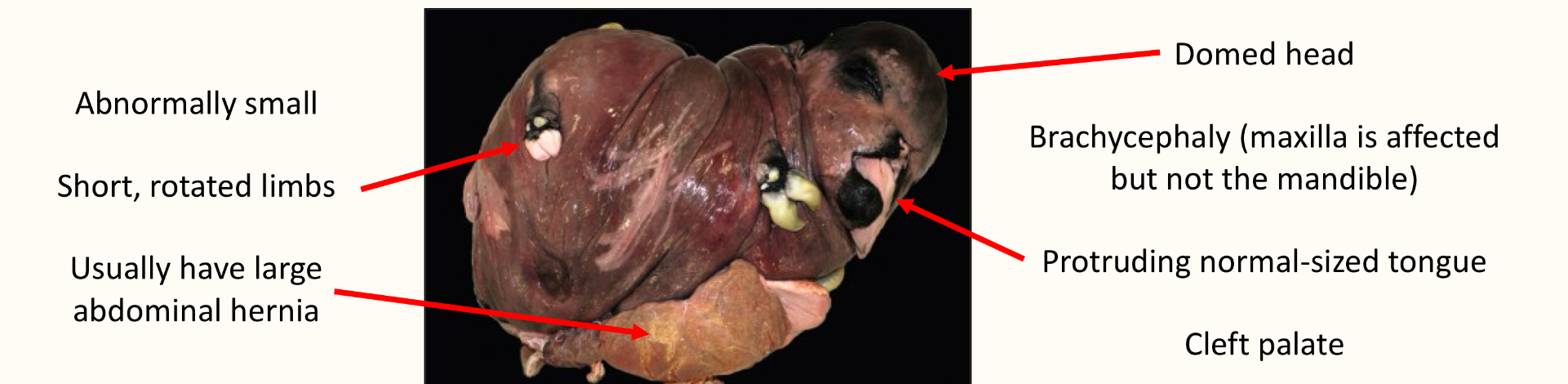
chondrodysplasia bulldog type:
seen in dexter cows
autosomal recessive
chondrodysplasia spider lamb syndrome:
suffolk and hampshire sheep breeds
FGF3 receptor defect
long necks and limbs, spinal curvature, angular limb deformities
multiple ossification centers
FGF4 defect
chondrodysplasia in corgis, pekingnese, and bassett hounds
physeal dysplasia of femoral capital physis
persistence of mutiple physes after they should close
osteopetrosis
autosomal recessive disease causing defective osteoclast numbers and/or activity
congenital hyperostosis
rare lethal disease in newborn pigs that causes periosteal new bone and soft tissue edema
craniomandibular osteopathy
bilateral bone proliferation on skull, mandibles, ± tympanic bulla
craniomandibular osteopathy signs:
4-7 months
painful chewing or inability to open mouth
fever
atrophy of masticatory muscles
hypertrophic osteopathy
diffuse periosteal new bone formation along limbs, associated with chronic inflammatory or neoplastic lesion in thorax
benign bone cyst pathology:
long bones
erode cortex
can cause fractures
resolve with curettage, steroid, or bone graft
aneurysmal bone cyst pathology:
ballooned periosteum
soap bubble appearance
resolve with excision
can cause fractures
signs of malnutrition or starvation in bone:
growth arrest lines
osteoporosis
serous atrophy of fat
where is the majority of body Ca and P stored?
hydroxyapatite
what stimulates activation of vitamin D?
direct: PTH, low P
indirect: low Ca
phosphatonins
reduce P
calcitonin
reduces serum Ca
osteopenia
increased radiolucency of bone that can be due to many factors
causes of osteoporosis:
aging
disuse
starvation (serous atrophy)
pure Ca deficiency
copper deficiency (reduced collagen crosslinking)
steroids
GI malabsorption
radiographs only show osteoporosis when ______% of bone calcium is lost
30-50
osteoporosis lesions:
loss of trabeculae
remaining trabeculae become thick
enlarged medulla
thin cortices
growth arrest line
serous atrophy
rickets
defective bone mineralization in young animals
osteomalacia
defective bone mineralization in adult animals
phosphorus deficiency signs:
pica
rickets signs:
lameness
angular limb deformities
swollen joints
segmentally thickened physes
enlarged costochondral junctions
fibrous osteodystrophy
excess bone resorption and replacement by excess fibrous tissue due to persistent increases in PTH
what can cause fibrous osteodystrophy?
primary hyperparathyroidism
secondary hyperparathyroidism
renal secondary hyperparathyroidism (reduced P excretion and loss of Ca)
nutritional secondary hyperparathyroidism (high P:Ca diet)
nutritional secondary hyperparathyroidism signs:
soft bones
bilateral skull enlargement
vitamin C deficiency pathogenesis:
reduced collagen production and crosslinking (scurvy)
vitamin A toxicity pathology:
narrowing or destruction of physes
osteoporosis
exostoses (bony outgrowths) in chronic exposure
teratogenic
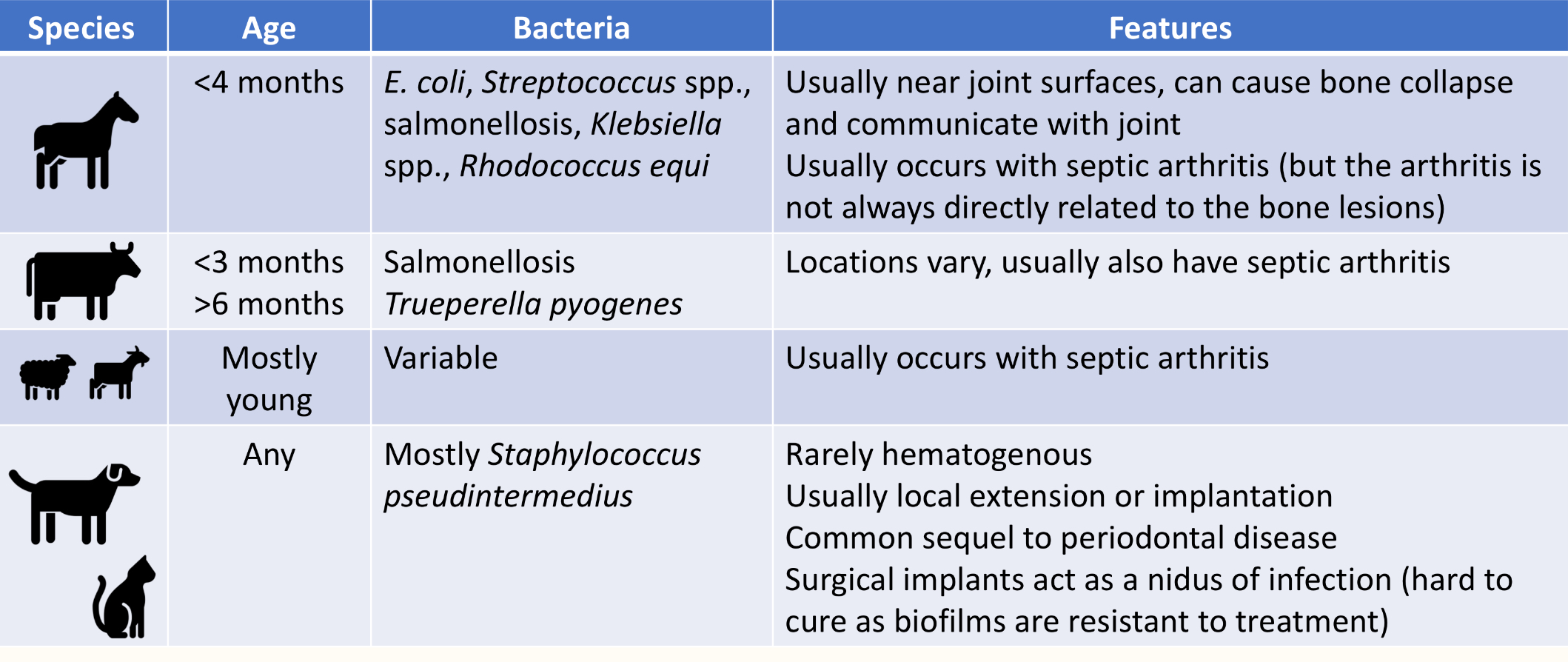
osteomyelitis
inflammation of medulla
exostosis
nodular, benign, bony growth projecting from bone’s surface
enostosis
bony growth within medullary cavity
what are the 3 routes of bacterial entry for osteomyelitis?
hematogenous
local extension
implantation
outcomes of bone infection:
resolution
abscess
sequestration
what bacteria can cause osteomyelitis?
pasteurella multocida and bordetella bronchiseptica in pigs (atrophic rhinitis)
actinomyces bovis (lumpy jaw)
actinomyces bovis bone pathology:
pyogranulomatous inflammation
bone enlargement with honeycomb appearance
sulfur granules
fungal osteomyelitis pathology:
pyogranulomatous inflammation
what fungi can cause fungal osteomyelitis?
coccidioides immitis
blastomycosis
cryptococcus spp
metaphyseal osteopathy signs:
large breed puppies
fever
pain
lameness
double physis sign parallel to physis
panosteitis
a non-inflammatory condition that affects long bones large breed dogs
panosteitis signs:
shifting lameness
increased medullary density starting at nutrient foramen and spreading outward
primary bone tumors are common in ____
dogs
osteoma
benign tumor that is smooth, hard, dense and well differentiated that is common in large animals
ossifying fibroma
benign tumor that is hard, slow-growing and well differentiated that is common in horses
fibrous dysplasia
replacement of bone by fibrous tissue and disorganized osteoid matrix
osteosarcoma pathology:
production of osteoids
what is the most common primary tumor of the appendicular skeleton in cats and dogs?
osteosarcoma
osteochondroma presentation in dogs:
benign tumor that arises near physis or articular cartilage or bones formed by endochondral ossification
have cartilage cap
osteochondroma presentation in cats:
arises in periosteum
affects flat bones
not connected to underlying marrow
multilobular tumor of bone
slow growing, aggressive cartilage tumor that occurs mostly on skull
chondrosarcoma
malignant tumor that produces chondroids and can invade and cross link joints
giant cell tumor of bone appearance:
expansile osteolytic mass usually in long bones
benign
soap bubble appearance
fibrous joints
united by fibrous tissue
kinds of fibrous joints:
sutures
syndesmosis
gomphosis
sutures are on the _____ only
skull
syndesmosis
bones connected by ligament
gomphosis
connect teeth to jaw by periodontal ligament
kind of cartilaginous joints:
synchondrosis
symphysis
synchondrosis
temporary joint at physis
nucleus pulposis
gelatinous central part of intervertebral disc
annulus fibrosis
fibrocartilage outer part of intervertebral disc
synovial joint components:
articular hyaline cartilage
joint capsule
synovial fluid
articular joint capsule is continuous with…
periosteum of adjacent bones
synovial membrane is lined by _________
synoviocytes
type A synoviocytes:
macrophage lineage
phagocytic
long lifespan