Gas Exchange and Transport: O2
1/27
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
28 Terms
What is the difference between systemic and pulmonary circulation?
Pulmonary circulation: right heart → lungs → left heart (gas exchange)
Systemic circulation: left heart → body → right heart (tissue perfusion)
Describe the blood supply to the lungs.
1) Pulmonary circulation (low pressure)
Primary function: gas exchange
Pulmonary Arteries (extra-alveolar): carry deoxygenated blood from the heart to pulmonary capillaries around the alveoli
Capillaries: site of gas exchange
Pulmonary veins (extra-alveolar): carry oxygenated blood from the lungs back to the heart
2) Bronchial circulation
Part of the systemic circulation
Bronchial arteries supply oxygenated blood to lung parenchyma
Bronchial veins carry deoxygenated blood that partially drains into pulmonary veins
👉 Because bronchial venous blood (Deoxygenated) mixes with oxygenated pulmonary venous blood, this creates an anatomic (physiologic) right-to-left shunt, slightly lowering arterial O₂ levels.
Describe the oxygen and carbon dioxide exchange occurring in the pulmonary and systemic circuits.
Gas movement is driven by partial pressure gradients:
O₂ moves from high PO₂ → low PO₂
CO₂ moves from high PCO₂ → low PCO₂
Pulmonary circuit
Blood enters the lungs via pulmonary arteries (deoxygenated, high CO₂).
O₂ enters blood, CO₂ leaves blood
Occurs in the lungs (alveoli)
Blood arriving is low in O₂, high in CO₂
Oxygen moves:
From alveoli → into blood
Carbon dioxide moves:
From blood → into alveoli → exhaled
👉 Result: Blood becomes oxygenated
Systemic circuit
O₂ leaves blood, CO₂ enters blood
Oxygenated blood leaves the lungs via pulmonary veins and travels to tissues.
Occurs in body tissues
Blood arriving is high in O₂, low in CO₂
Oxygen moves:
From blood → into tissues (for metabolism)
Carbon dioxide moves:
From tissues → into blood (waste product)
👉 Result: Blood becomes deoxygenated
similar volumes of CO2 and O2 move each minute (Which is why it is called gas EXCHANGE).
Describe how the partial pressure gradients drive gas exchange in systemic and pulmonary circuits.
Pulmonary circulation (gas exchange)
Oxygen
PAO₂ ≈ 100 mmHg
Oxygen pressure in the alveoli
Pulmonary arterial blood (PvO₂) ≈ 40 mmHg
Deoxygenated blood arriving from the right heart
Gradient: PAO₂ (100) → blood (40)
O₂ diffuses into blood
After equilibration:
PaO₂ ≈ 95–100 mmHg
Slightly lower than PAO₂ due to physiologic/anatomic shunt
Carbon dioxide
Pulmonary arterial PCO₂ ≈ 45 mmHg
Alveolar PCO₂ ≈ 40 mmHg
Gradient: blood → alveoli
CO₂ diffuses out of blood
Smaller pressure gradient than O₂, but CO₂ diffuses easily because it is more soluble
👉 Result: blood leaving lungs is oxygenated and low in CO₂
Systemic circulation (tissue gas exchange)
Oxygen
PaO₂ ≈ 95 mmHg = arterial partial pressure of oxygen in systemic arteries
Blood arriving at tissues
Tissue PO₂ ≈ 40 mmHg (or lower)
Gradient: blood → tissues
O₂ leaves blood
Carbon dioxide
Tissue PCO₂ ≈ 45 mmHg
Arterial PCO₂ ≈ 40 mmHg
Gradient: tissues → blood
CO₂ enters blood
👉 Result: blood returning to lungs is deoxygenated and CO₂-rich
Describe the partial pressure values for pulmonary arterial blood, for the systemic arterial, and alveolar pressures.
PvO₂ / PvCO₂ = mixed venous blood
Blood in the pulmonary arterial = systemic venous blood
Pulmonary arterial blood has:
PvO₂ (~40 mmHg)
PvCO₂ (~45 mmHg)
PaO₂ / PaCO₂ = systemic arterial blood
Pulmonary Veinous = systemic arterial blood
PaO₂: 95–100 mmHg
PaCO₂: ≈ 40 mmHg
Systemic Veinous Blood:
PvO₂: ≈ 40 mmHg
PvCO₂: ≈ 45 mmHg
Partial Pressure in Alveoli
PAO₂ ≈ 100 mmHg
PACO₂ ≈ 40 mmHg
What is the driving force for gas movement?
Diffusion is the driving force for gas exchange at the respiratory surfaces
All animals have some of the thinnest respiratory membranes to allow good diffusion
What is a gas exchange membrane?
Thin partitioning between internal and external compartments promoting flux of respiratory gases
How does the thickness of blood/water/air barriers change from fish, to amphibians, to reptiles, to mammals, to birds?

Describe the partial pressure of gas through the anatomic dead space → the body.
Anatomic Dead Space
PIO2 = 150
PICO2 = 0
Alveoli
PAO2 = 102
PAACO2 = 40
Pulmonary Artery - functionally the same as systemic venous blood
PVO2 = 40
PVCO2 = 46
Pulmonary Veins - functionally same as systemic arteries
PpvO2 = 102
PpvCO2 = 40
Better to write as:
PaO₂ ≈ 95–102 mmHg
PaCO₂ ≈ 40 mmHg
**PI = partial pressure inhaled
What two ways can the partial pressure of O2 be altered?
Atmospheric Pressure Changes (Altitude)
Presence of water vapor
How does a difference in altitude alter the partial pressure of O2?
If atmosphere pressure changes (eg altitude), there will be a change in PO2
• The partial pressure of O2 alters depending on other factors eg atmospheric pressure (Ратм)
• PO, can be calculated by this equation:
PATM in mmHg
FO2 = mole fractional concentration of oxygen in air (0.21 for air), always 21%, unless you change

How can water vapour molecules alter the partial pressure of O2?
Presence of water vapor molecules, which reduces concentration of O2. PO2 is less in humidified air, PO2 of humidified gas in airways is calculated by (Equation in photo)
• PO, is less in humidified air
• PO, of humidified gas in airways is calculated by:

Why does the partial pressure of O2 drop as air enters the alveoli?
Air composition vs alveolar air
Atmospheric air (trachea) has a PO₂ ≈ 160 mmHg (21% of 760 mmHg at sea level)
Alveolar air has PO₂ ≈ 100 mmHg
Why the drop? Two main reasons:
2. Moisture in the airways
As air travels down the trachea and bronchi, it becomes fully humidified
Water vapor contributes ~47 mmHg to total pressure
This reduces the partial pressure of O₂
3. Gas exchange in alveoli
Alveoli aren’t empty — they contain:
Residual CO₂ from blood (~40 mmHg)
Some remaining O₂ from previous breaths
The presence of CO₂ dilutes the O₂, lowering PO₂ further to ~100 mmHg
Why does PAO₂ (alveolar PO₂) equal PpvO₂ (pulmonary vein PO₂), and why is this important in hypoxia?
Equilibration: Pulmonary capillary blood equilibrates with alveolar air, so PAO₂ ≈ PpvO₂.
Mechanism: O₂ diffuses down its partial pressure gradient until no difference remains.
Importance in hypoxia:
Low alveolar PO₂ → low pulmonary vein PO₂ → reduced O₂ delivery to tissues.
Highlights that alveolar oxygen sets the maximum systemic oxygen level.
What are the two forms that O2 can be carried in within the blood?
i) Dissolved (measured clinically in arterial blood Pa°2) -very small %
ii) Bound to haemoglobin (Hb)
Haemoglobin (Hb) is major transport molecule for O, found in red blood cells.
Hb: four heme (iron porphyrin compounds) groups joined to globin protein (two a chains and two ß chains polypeptide chains).
Each heme group contains iron in the reduced ferrous form (Fe**), which is the site of 0, binding.
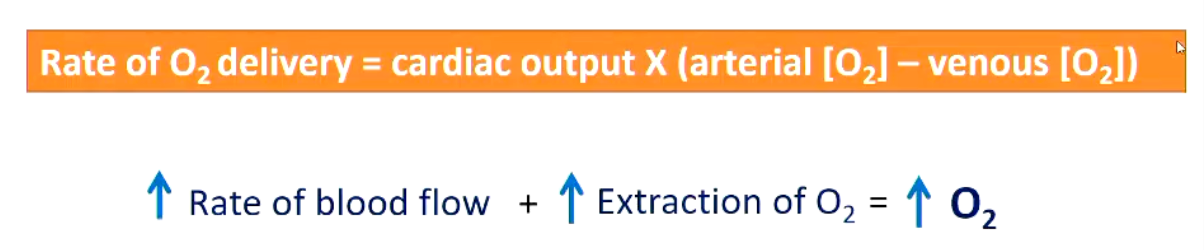
Oxygen transport can be modified by what three mechanisms?
1. Concentration of pigment (Hemoglobin conc.)
2. Rate of circulation (cardiac output etc) - how quickly it moves around body
3. O2 affinity of pigment (Hemoglobin)
How does concentration of pigment vary amongst different species?
Concentration of pigments is very variable
• birds and mammals 15-20ml/100ml
Lower in invertebrates with Hb
• annelid 4-6ml/100ml)
Animals with haemocyanin tends to be even lower
• squids and octopuses 3.7ml/100ml
• crabs/prawns 1ml/100ml
How does the rate of circulation change with exercise?
• Circulatory system of mammals and birds operates at leisurely pace at rest
• During exercise O2 demand increases so circulatory system responds
Venous blood becomes much more deoxygenated during exercise than at rest
What factors affect the oxygen affinity of haemoglobin?
• Degree of Hb oxygenation depends on PO2
High PO2 = at lungs (promote uptake onto the haemoglobin)
Low PO2 = at tissues (promote oxygen being pushes off - into the tissues)
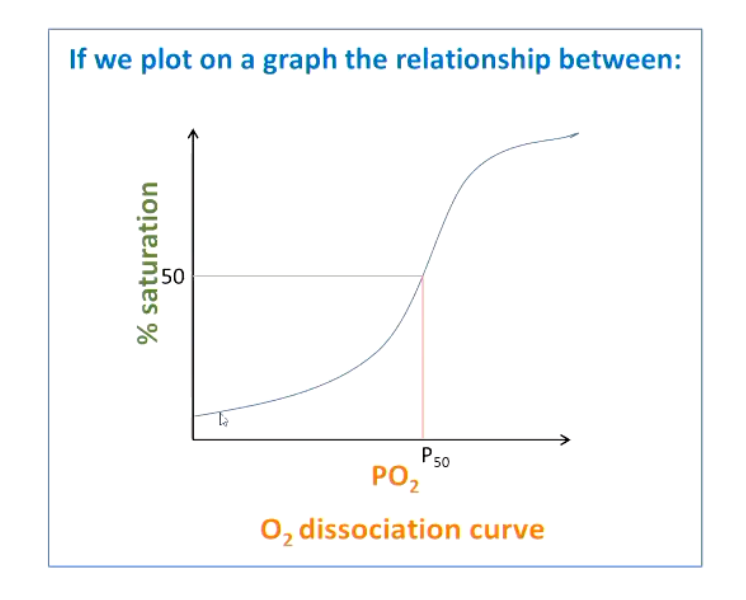
Describe the oxygen affinity curve, waht is P50?
P50 = the partial pressure of O2 at which 50% of pigment is bound to O2
How does the oxygen affinity curve change with hemoglobin and myoglobin?
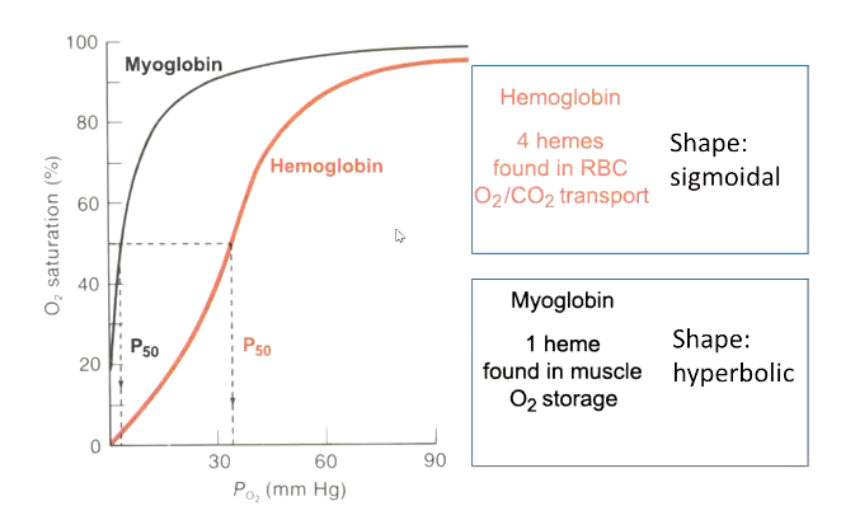
Why does hemoglobin show a sigmoidal curve?
Cooperative binding, binding at one site increased affinity at the remaining sites
Partially oxygenated Hb is more likely to bind O2 than fully deoxygenated molecule
Cooperatively enhances the responsiveness to changes in PO2
Cooperative binding means:
Binding of O₂ to one subunit → increases the affinity of the remaining subunits for O₂
Releasing O₂ from one subunit → decreases affinity of the others
How does oxygen affinity vary?
If oxygen affinity is lowered, how will the curve shift?
Respiratory pigments of various animals vary in their O2, affinity
• Pigments that bind O2 at low PO2 HIGH AFFINITY
• Pigments that require a higher PO2, to bind O2 LOW AFFINITY
Shift to the right, means O2 more difficult to bind to Hb, but easier to release O2
What are the factors affecting O2 affinity?
1. pH and CO2 - The Bohr effect
2. Temperature
3. lons
4. Organic compounds
How does pH or the Bohr effect alter oxygen affinity?
• Oxygen affinity depends on the PCO2 and the pH
Low pH (more acidic) or high CO₂ → stabilizes deoxygenated Hb (T state) → reduces O₂ affinity - right shift
High pH (more basic) or low CO₂ → stabilizes oxygenated Hb (R state) → increases O₂ affinity - left shift
In tissues (high CO₂, low pH from metabolism):
Hb releases O₂ more readily → oxygen delivered to metabolically active cells
In lungs (low CO₂, higher pH):
Hb binds O₂ more tightly → efficient oxygen loading

Enhancing oxygen delivery means lowering oxygen _____.
affinity
How does temperature alter O2 affinity?
• Increase in temperature decreases O, affinity → shift to right
Enhancing O2 delivery to muscles, similar to Bohr effect
How do inorganic ions and organic compounds alter O2 affinity?
3. Inorganic ions O, affinity
• lons in the blood can allosterically modulate O2 affinity of respiratory pigments
• Cl ions in RBCs critical allosteric modulator
They bind to hemoglobin at specific sites → stabilize the deoxygenated (T) state.
Decreases O₂ affinity → Hb releases O₂ more easily to tissues
4. Organic compounds
• 2,3-diphosphoglycerate (DPG) reduces O2, affinity of Hb molecules it binds
2,3-DPG is a molecule produced in red blood cells during glycolysis
• Human Hb continuously exposed to 2,3-DPG so constantly modulated by a "normal" DPG level
• 2,3-DPG is increase by chronic hypoxia, anaemia and acclimation to high altitude