Looks like no one added any tags here yet for you.
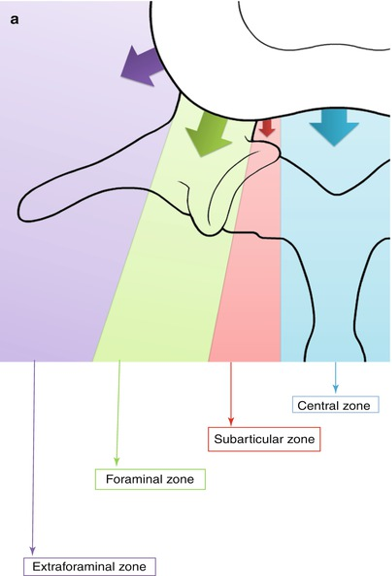
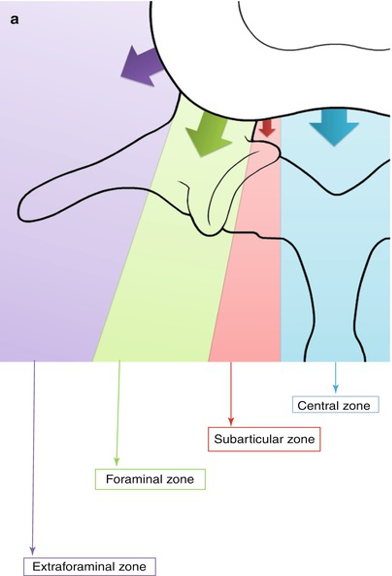
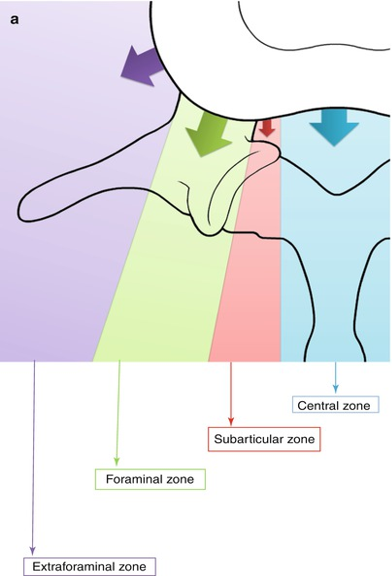
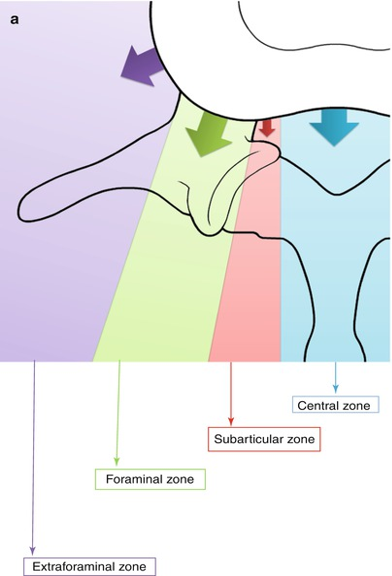
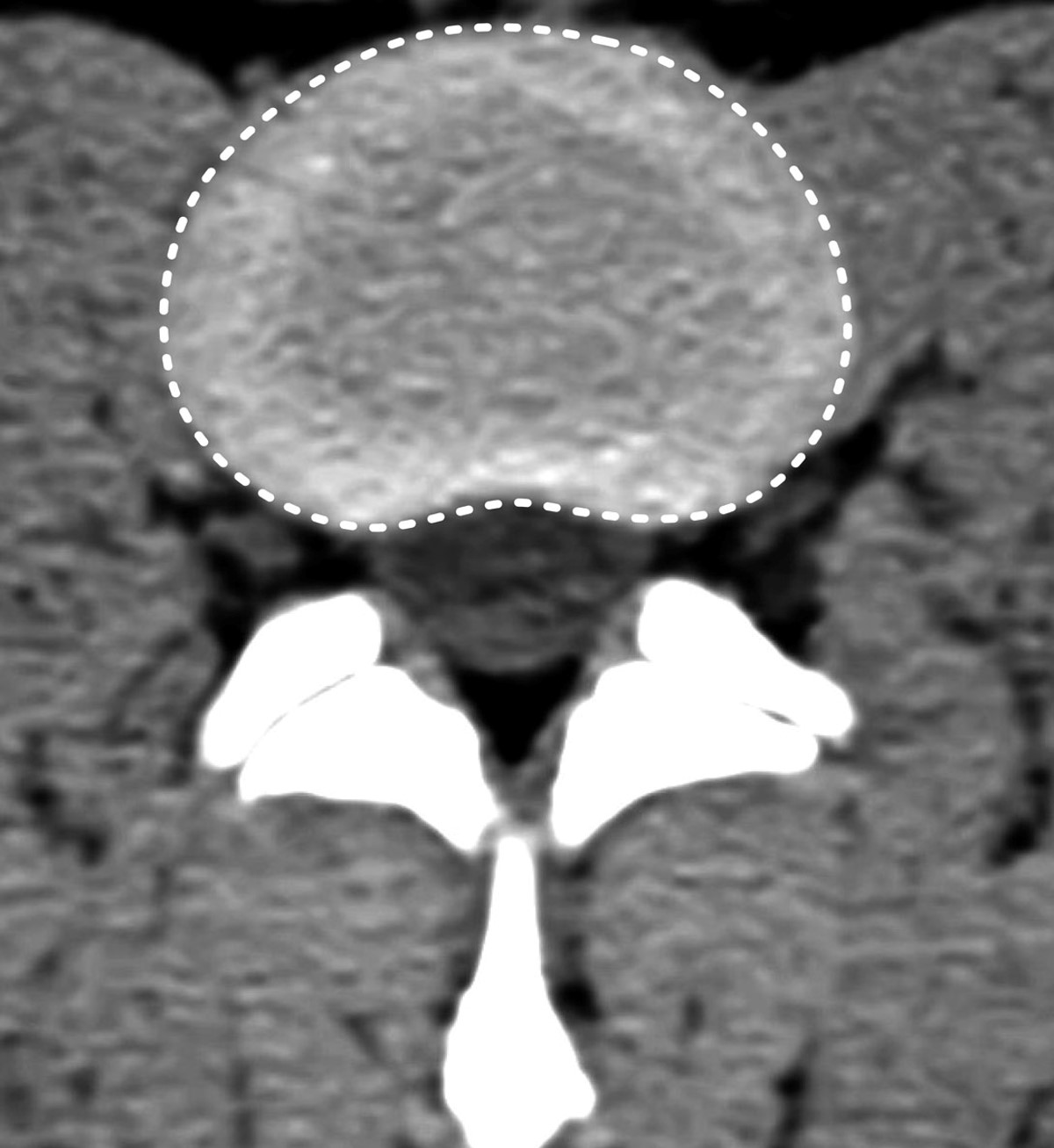
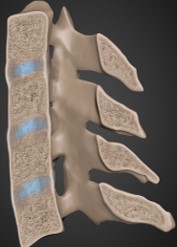
Central Zone
Zone where PLL is thickest
Disc usually herniates slightly lateral to this zone
Subarticular Zone
Aka Lateral Recess or Paracentral
Zone where disc extrudes between the spinal cord and the foramen
Next to spinous process
Foraminal Zone
Disc extrusion into the foramen
Extraforaminal Zone
Far lateral
Disc extrusion beyond the foramen
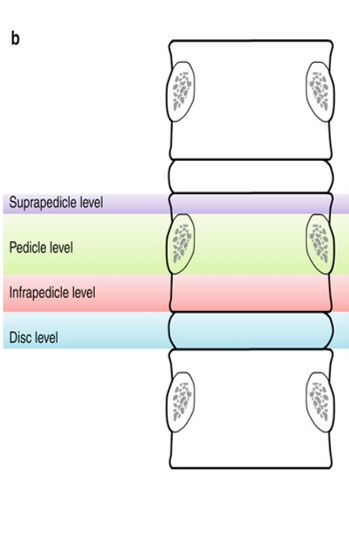
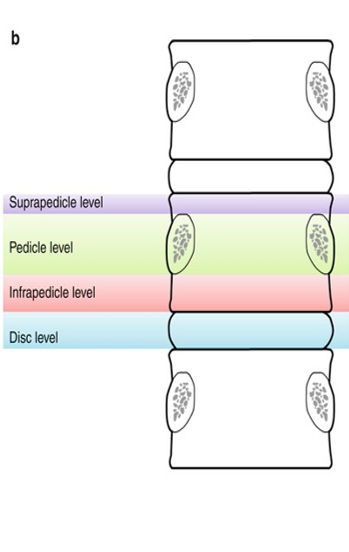
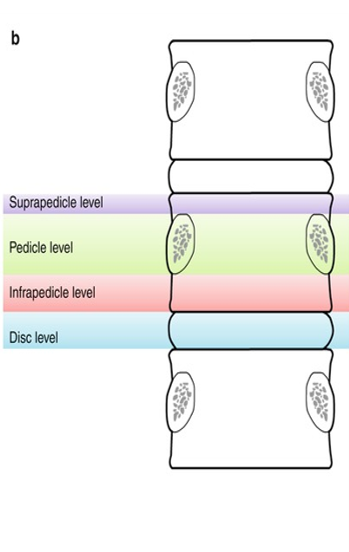
Suprapedicle
Superior portion of vertebra
Pedicle
Below suprapedicle, middle portion of vertebra
Disc level
Level of the disc
Cervical Radiculopathy
Cervical canal or foraminal stenosis at the level where the nerve roots exit the cervical spine
Typically due to disc herniation or facet joint hypertrophy
Radiculopathy Symptoms
Unilateral
Paresthesia - numbness
Weakness in arm, shoulder, or hand
Decreased motor skills
Loss of sensation in a dermatome fashion
Pain associated with neck movement or strain
Disc herniation
Displacement of intervertebral disc
Involves less than 25% of the circumference
Protrusions
Base wider than the dome
Confined to disc level
Outer annular fibers intact
Involves less than 90 degrees of the disc circumference
Extrusions
Base is narrower than the herniation dome
Conservative Disc Herniation Treaments
Managed with non-surgical treatments as the majority of patients will improve
Collar Immobilization
Short course (1 week) may be beneficial during the acute inflammatory period
Traction
Widens the neuroforamen and relieves the stress placed on affected nerve. Involves approximately 8 - 12 lbs of traction over a period of 15-20 minutes
Pharmacotherapy
No evidence the efficacy of NSAIDs in the treatment of cervical radiculopathies. Commonly used and can be beneficial for some patients. Opioids effective in relieving acute pain (risk of addiction)
Physical Therapy
No evidence demonstrates efficacy over placebo
Cervical Manipulation
Short-term benefits for neck pain and cervicogenic headaches
Interventional Treatments
Spinal steroid injections into the epidural space decreases the swelling of irritated nerve roots and are common alternative to surgery.
Surgical Treatments
Indications: severe or progressive neurological compromise; significant pain that is refractory to non-operative measures
Anterior Cervical Discectomy and Fusion
Gold standard treatment
Allows the removal of the pathology
Prevention of recurrent neural compression by performing a fusion
Posterior Laminoforaminotomy
Considered in patients with anterolateral herniations and/or osteophytes
Prognosis with conservative treatment
Symptoms subside on their own over six weeks in the majority of patients
Symptoms persist in ¼ of patients despite intervention
Prognosis with surgical intervention for disc disease
More rapid resolution of symptoms.
No significant difference from non-surgical treatment after 5 years.
Disc Bulge
Displacement of the outer fibers of the annulus beyond the margins of the endplate
Involves more than 25% of the circumference of the intervertebral disc
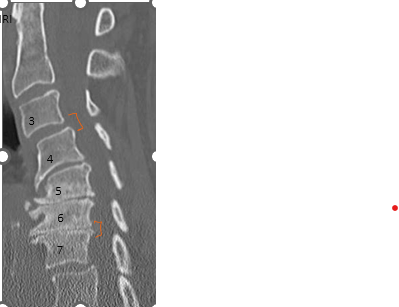
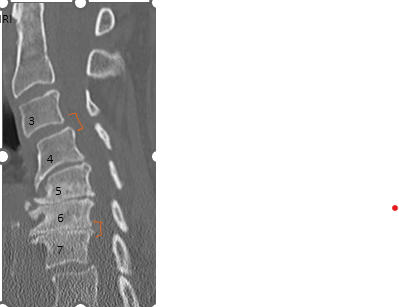
Cervical Degenerative Spondylosis or DDD
Osteophyte formation, disc height narrowing, and end-plate sclerosis
Normal: no degenerative change
Minimal: minimal anterior osteophyte formation, no reduction of disc height, no end-plate sclerosis
Mild to Moderate-increasing anterior osteophytes, decrease of disc height, increased endplate sclerosis and osteophyte sclerosis.
Advanced-Large and multiple osteophyte formation, severe narrowing of the disc space (>75%), end-plate sclerosis with irregularities.
Grade level for C3-C4
Minimal
Grade level for C6-C7?
Advanced
Aging Disc
Disc herniates, annulus fibers begin to weaken-bulging
Surrounding ALL, PLL, and facet joint capsules weaken
Osteophyte formation and eventual bridging of disc space
How the bone reacts in an attempt to stabilize the disc space and facet joints
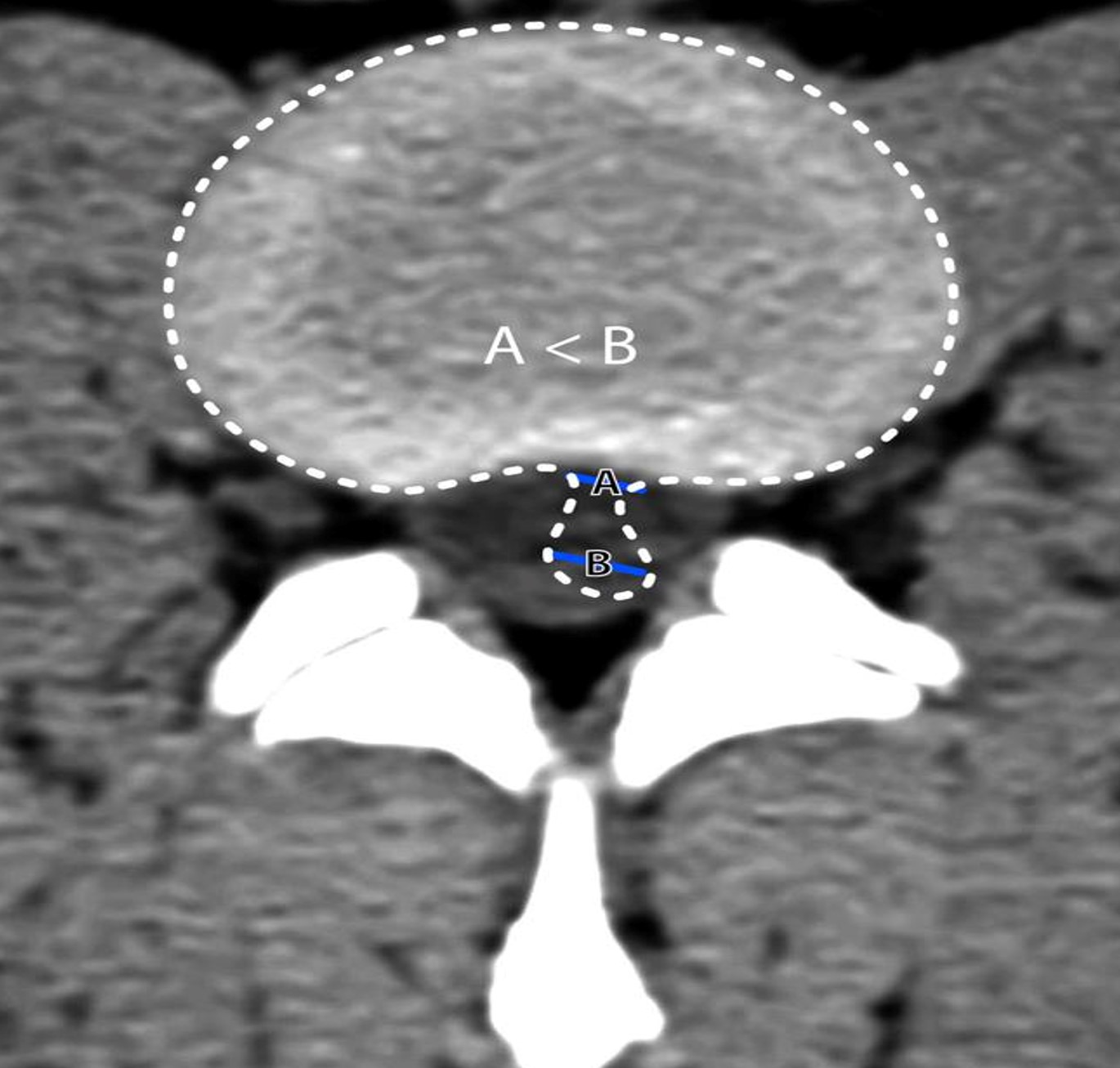
Compressive Cervical Myelopathy
Upper motor neuron signs:
-hand weakness
-spasticity
-clumsiness
-altered tonus
-hyperreflexia
Causes of compressive cervical myelopathy
Spondylotic osteophyte/disc complex most common
Central disc herniation
Congenital cervical spinal stenosis
OPLL
Rheumatoid arthritis of the neck
Malalignment of cervical spine
Spondylolisthesis: one vertebral body slips forward (or backward) out of alignment with the column. Relative to the vertebral body above.
Results in an unstable spine that can eventually narrow the spinal canal, the neuroforamina or both.
Spondylosis
Degenerative changes in the spine with disc space narrowing and osteophytes
Spondylolisthesis
Off set of the vertebral bodies from the spinal column
Spondylolysis
Stress fracture of the pars interarticularis
Ossification of PLL (OPLL)
High cervical region (C2-C4)
Myelopathy pain, neurological deficits
Majority without significant symptoms
Posterior cervical decompression
Removing the lamina or reconstructing in order to release pressure on the cord. May or may not include a fusion and instrumentation depending on risk of instability.
Discitis and Osteomyelitis
Results from direct inoculation, extension or hematogenous spread (S. aureus most common).
Symptoms: neck pain, back pain, focal tenderness, fever and myelopathy. Pain with pounding.
Pyogenic: predisposing factors - IV drugs, immmunocompromised
Early: subtle disc space narrowing, mild endplate irregularity (best seen on sagittal views
Late: overt body collapse, paraspinal/epidural swelling and fluid collection
MRI is the most sensitive for osteomyelitis and epidural abscess/phlegmon
Bone metastatic disease
Sites: thoracic, lumbar, ribs, pelvis, skull, and proximal femur
Bone is the third most common location for metastasis after lung and liver
CT scans and nuclear medicine bone scans detect bone metastases before becoming symptomatic
Diffuse Idiopathic Skeletal Hyperostosis (DISH)
Aka Forestier disease
Common condition - bony proliferation site of tendinous and ligamentous insertion of the spine (at least four contiguous bodies) - affects elderly individuals
Characterized by flowing ossification of ALL - cervical and thoracic spine and enthesopathies.
DISH clinical presentation
Spine stiffness and decreased mobility. Monoarticular synovitis, dysphagia and airway obstruction are less common.
Focal and diffuse calcification and ossification of ALL.
Hypervascularity, chronic inflammatory cellular infiltration, ossification of entheses-bony attachments of tendons and ligaments.
Periosteal new bone formation on the anterior surface of the vertebral bodies.
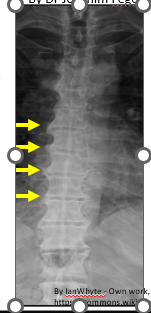
DISH
“Melted candle wax” appearance of calcification and ossification. Note the preponderance on the patient’s right side.
Ankylosing spondylitis
Seronegative spondyloarthropathy (RF negative) results in fusion of the spine and SI joints
HLA B27 is the gene with the strongest association
Radiographic features: “bamboo spine” appearance. Axial skeleton is predominantly affected. 20% of cases the peripheral joints are also involved.
Syndesmophytes
Classically described as paravertebral ossification running parallel to the spine
Dagger spine
Linear ossification along the central spine representing the interspinous ligament ossification
CT
Excellent at evaluating bony changes and ossification
MRI
Soft tissue abnormalities and evaluation of the cord