DKA & HHS
1/10
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
11 Terms
DKA Labs
Usually type 1
Rapid onset
>250 glucose
<7.3 pH
Present ketones
<15 bicarb
Elevated kidney labs
HHS Labs
Slower (several days)
>600 glucose
normal pH
Absent ketones
Normal bicarb
Elevated kidney labs
DKA rf
13-25 age
female
previos episodes
HHS rf
Older than 65
african american
native american
hispanic
morbid obesity
DKA impact on health
Metabolic acidosis
Muscle weakness
Dehydration leading to decreased cardiac output
Loss of electrolytes
Cardiac arrhythmias
High POtassium initially
Kussmaul respirations
Decreased perfusion to kidneys
HHS impact on health
More profound neurological manifestations
Muscle weakness
Profound dehydration
Thromboembolic disease (clot risk)
Decreased perfusion to the kidneys
Loss of electrolytes
Cardiac arrhythmias
DKA + HHS Presentation
Decreased level of consciousness: fatigue, lethargy, coma
Nausea and vomiting
Abdominal pain
Fruity breath odor (DKA)
Hyperventilation
Hypotension
Arrhythmias
Blurred vision
Polydipsia
Weight loss
Hypokalemic
Labs and diagnostic studies
Serum blood glucose: DKA greater than 250mg/dL and HHS greater than 600 mg/dL
Complete blood count: assess WBC
Electrolytes: K, MG, NA, Cl, Phos,
ABGs: clients in DKA will be in metabolic acidosis pH less than 7.3 and HCO3less than 15
Anion gap: DKA greater than 10 mEq/L indicating acidosis. HHS: within normal limits
Serum osmolality: HHS greater than 320 mOsm/kg
Urine studies: UA, Ketones, Urine culture: DKA will have both glucose and ketones present. Urine osmolality will be above expected range in DKA.
Chest X-Ray: determine presence of respiratory illness (pneumonia)
ECG: assess for dysrhythmias
Blood and Urine Cultures: looking for sepsis
DKA and HSS treatment
Circulatory volume
Large bore IV or central line
Replace half of the deficit in 12-24hrs
IV Isotonic fluid to increase intravascular volume
monitor sodium
switch to IV hypotonic
BG <250 in DKA, <250 in HHS, → switch fluid to D5 in 0.45% NS
Treat hyperglycemia
Avoid a rapid drop in blood glucose levels
Bolus of IV regular insulin based on client’s weight (0.1 units/kg)
Continuous IV regular insulin at 0.1 units/kg/hour
Goal is to decrease blood glucose by 50 to 70 mg/dL/hr (adjust rate if this is not met)
Once blood glucose is consistently less than 200 mg/dL for DKA and less than 300 mg/dL for HHS IV insulin rate can be decreased to 0.02-0.05 units/kg/hour.
Adjust rate hourly to keep blood glucose of 150 to 200 mg/dL
Once DKA or HHS is resolved and client tolerates oral intake, transition to SQ insulin (dose will vary depending on client’s history)
IV insulin continued for at least 2 hours after the first dose of SQ insulin
Correct electrolyte ibalance
Potassium: 4.0-5.0
Sodium: correct with fluids
Magnesium as needed
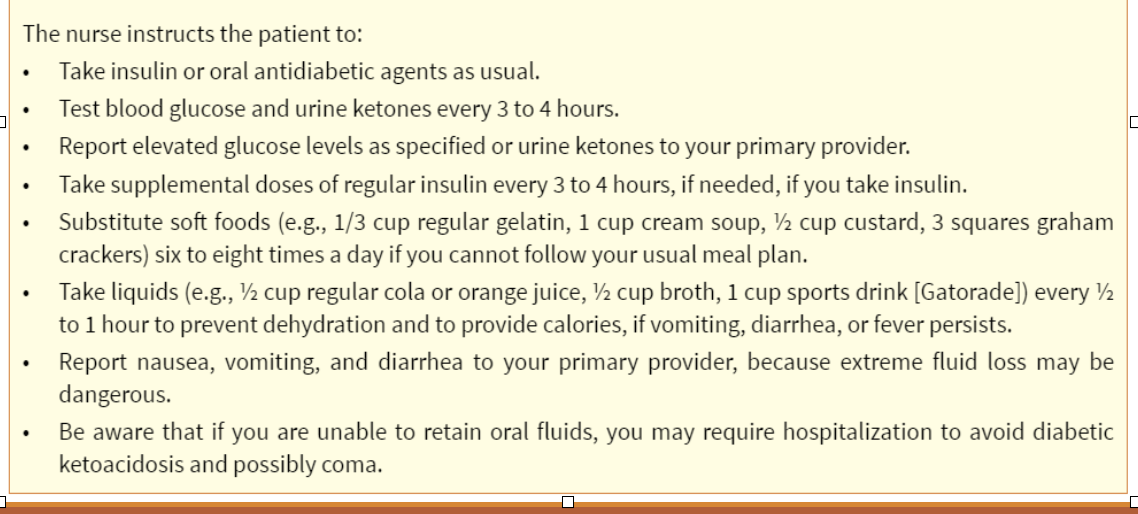
Sick day rules
Insulin drip and IV push
need a 2nd nurse to verify the order
discard first 50ml of fluid