MDL242 - Week 7 Learning Objectives
1/39
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
40 Terms
Identify the enzyme that degrades fibrin.
Plasmin
Describe how plasminogen functions in the clotting process.
initiates fibrinolysis, is converted to plasmin by Tissue Plasminogen Activator
Discuss the formation of plasmin and how it works as an anticoagulant.
Plasminogen converted to plasmin by TPA and UPA
Describe what DIC is, different causes of DIC, clinical presentation of DIC, and how it is diagnosed in the laboratory.
Disseminated Intravascular Coagulation (DIC) is an acquired bleeding disorder characterized by excessive thrombin and plasmin caused by tissue/organ clots and hemorrhages. Stages are Compensated, or Acute (non-compensated)
Treated by looking for the cause and treating the cause:
Can be caused by sepsis, tissue necrosis, amniotic fluid, tumors, snake venom
Explain various causes of thrombosis.
Disturbances of regulatory mechanisms: Protein S, Protein C, Antithrombin III, plasminogen
Hereditary: factor V Leiden mutation, Prothrombin gene mutation; ATIII, Protein S, and Protein C deficiencies
Acquired Antiphospholipid antibody, malignacy, increased factor VIII and increased fibrinogen
Describe how heparin functions to inhibit clotting.
Explain why D-Dimer and FDP are important and how they are formed.
Identify heparin's mechanism of action, what LMWH is and how it differs.
Low Molecular Weight Heparin, only effects Factor X,
Identify the factors, in order, in the coagulation pathway, including factors I,II,VII,VIII,IX, X, XIII .
I -
II -
VII - feedback loop with factor X
VIII -
IX -
X - activates factor VII, feedback loop
XIII -
Explain the role of Factor XIII.
Factor XIII stabilizes fibrin clot
Describe the three major pathways in the cascade theory of coagulation
Extrinsic, Intrinsic, and Common
Correlate the coagulation cascade and the role of fibrin
Explain the consequence of a Factor V Leiden gene mutation.
causes an impaired Degradation of factor 5 by activated protein C, causes recurring thrombosis
Identify the substrate for plasmin
Fibrin/fibrinogen
Discuss the vitamin K dependent factors that are affected by Coumadin/Warfarin
II, VII, IX, X, PC, and PS
Identify and define INR including its importance in testing.
International Normalized Ratio is the standardized test results for PT worldwide
Reference range: 0.9 - 1.1
Therapeutic: 2.0 - 3.5
Describe secondary hemostasis including the major steps and how it related to coagulation testing
Differentiate primary and secondary hemostasis.
Primary is the initial response to vascular injury resulting in a platelet plug, and secondary is the formation and stabilization process of a clot
Explain the similarities and differences between Hemophilia A and B.
Hemophilia A - male, linked to recessive X chromosome of mother, deficiency of factor 8, bleed longer
Hemophilia B - deficiency of factor 9, still linked to recessive X chromosome of mother
Identify the coagulation factors that are vitamin K dependent and why is it important
Factors II, V, and VII
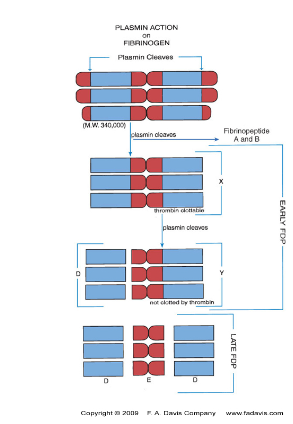
Describe the process of fibrinolysis, the enzymes involved, and the products of fibrinolysis.
Fibrinolysis is the removal of fibrin deposits through enzymatic cleavage, converts fibrin into soluble fragments in order to regain regular blood flow
Plasminogen - inactive plasma protein produced in the liver, activated by Tissue Plasminogen Activator (t-PA)
t-PA - found in vascular endothelium, converted to plasmin
Plasmin breaks Fibrin (fibrinogen) into X monomer
Plasmin splits X monomer into 1 Y and 1 D fragments
Y monomer is split into 1 D and 1 E fragments, resulting in 2 D and 1 E fragments, known as Fibrin Degradation Products (FDP/FSP)
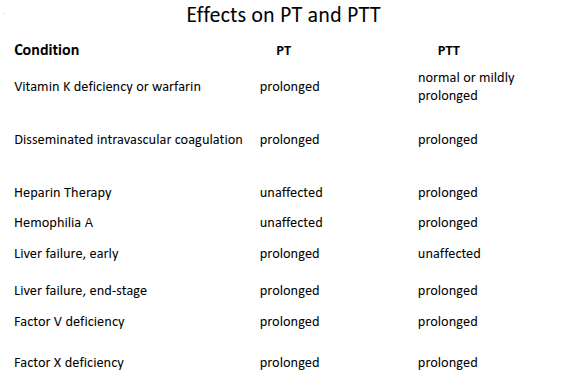
Identify the basic tests for hemostasis in the lab and what can interfere or cause incorrect test results.
Vitamin K deficiency/Warfarin - prolongs PT, mildly prolongs PTT
PT: Low caused by microclots, High caused by blood clotted, overdosed heparin, and blood drawn from arterial line(heparin contamination)
PTT: Low caused by microclots, High caused by blood clotted, overdosed heparin, and blood drawn from arterial line(heparin contamination)
Describe the common laboratory tests for evaluation of hemostasis and what pathways each test detects.
D-dimer: <0.5 ug/ml, measures Proteins S and C, only tests for D monomer, does not test for both FDP’s (D and E fragments)
Thrombin Time (TT):
Prothrombin Time (PT): 12-15 sec
Partial Thrombin Time (PTT):
Fibrinogen: 200 - 400 mg/dl
Review and understand the general mechanism of the other natural anticoagulants (ATIII, Protein C and S)
Antithrombin III - inhibits THROMBIN, Xa, IXa, XIa, XII, activated protein C, and Kallikren. Cofactor of heparin, heparin increases ATIII by 1000x
Protein C - activated by thrombin and protein S, vitamin K dependent
Protein S - activates protein C and is enhanced by protein C
What is the reference range for RBC?
4.0 - 6.0 × 10⁶/uL
What is the reference range for HGB?
12.0 - 18.0 g/dL
What is the reference range for HCT?
35 - 50%
What is the reference range for MCV?
76 - 100 fL
What is the reference range for MCH?
26 - 34 pg
What is the reference range for MCHC?
32 - 36 g/dL
What is the reference range for RDW?
11.5 - 14.5%
What is the reference range for RETICULOCYTES?
(Absolute) 20 - 115 × 10³/uL
(Relative) 0.5 - 2.5%
What is the reference range for nRBCs?
0 nRBCs per 100 WBCs
What is the reference range for PLATELETS?
150 - 450 × 10³/uL
What is the reference range for WBC?
3.6 - 10.6 × 10³/uL
What is the reference range for NEUTROPHILS?
(Absolute) 1.7 - 7.5 × 10³/uL
(Relative) 50 - 70%
What is the reference range for LYMPHOCYTES?
(Absolute) 1.0 - 3.2 × 10³/uL
(Relative) 18 - 42%
What is the reference range for MONOCYTES?
(Absolute) 0.1 - 1.3 × 10³/uL
(Relative) 2 - 11%
What is the reference range for EOSINOPHILS?
(Absolute) 0 - 0.3 × 10³/uL
(Relative) 1 - 3%
What is the reference range for BASOPHILS?
(Absolute) 0 - 0.2 × 10³/uL
(Relative) 0 - 2%