[Exam 3 OB Study Guide 1/2] ATI BOOK CONTENT
1/191
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
192 Terms
Chapter 20: Postpartum Disorders
Postpartum disorders are unexpected complications that can occur after childbirth. Nurses must understand each condition to provide effective care and ensure positive outcomes.
Key Postpartum Disorders to Know:
Thrombosis and Embolism:
Superficial and Deep-Vein Thrombosis (DVT): Blood clots in veins, commonly in the legs.
Pulmonary Embolus (PE): A clot that travels to the lungs, potentially life-threatening.
Coagulopathies (Blood Clotting Disorders):
Idiopathic Thrombocytopenic Purpura (ITP): Low platelet count leading to bleeding/bruising.
Disseminated Intravascular Coagulation (DIC): Widespread clotting followed by severe bleeding.
Hemorrhage and Uterine Complications:
Postpartum Hemorrhage: Heavy bleeding after birth.
Uterine Atony: Uterus fails to contract, causing excessive bleeding.
Subinvolution of the Uterus: Uterus does not return to its pre-pregnancy size.
Uterine Structural Issues:
Inversion of the Uterus: Uterus turns inside out, a medical emergency.
Retained Placenta: Placenta remains in the uterus, causing bleeding.
Trauma and Tissue Damage:
Lacerations: Tears in the genital tract during delivery.
Hematomas: Blood collects under the skin or in tissues, causing pain and swelling.
DVT
Risk Factors
Pregnancy and Birth:
Pregnancy itself
Cesarean birth (doubles the risk)
Operative vaginal birth (forceps or vacuum)
Circulation and Movement:
Pulmonary embolism or varicose veins
Immobility (e.g., bed rest)
Lifestyle and Health:
Obesity
Smoking
Multiparity (having multiple pregnancies)
Age and History:
Age > 35 years
History of thromboembolism (previous clots)
DVT S/S
Leg Pain and Tenderness
Unilateral swelling, warmth, and redness (usually one leg)
Hardened vein over the clot
Calf tenderness upon palpation
DVT Dx
Doppler Ultrasound: Checks blood flow and identifies clots.
Computed Tomography (CT): Detailed images to detect clots.
Magnetic Resonance Imaging (MRI): High-resolution images for complex cases.
DVT Care
Nursing Care: Prevention
Promote Circulation:
Sequential Compression Device (SCD): Until the patient can walk.
Range of Motion Exercises: If bed rest is prolonged (>8 hours).
Early and Frequent Ambulation: Encourage walking soon after childbirth.
Elastic Compression Hose: Measure and fit to lower extremities.
Client Education
Movement and Positioning:
Avoid Prolonged Immobility: No long-standing or sitting.
Elevate Legs: When sitting to improve blood flow.
Avoid Leg Crossing: Prevents poor circulation and blood pooling.
Hydration:
Fluid Intake: 2 to 3 liters per day to avoid dehydration and improve circulation.
Management
Positioning and Mobility:
Bed Rest and Leg Elevation: Above heart level (No pillows under knees).
Frequent Position Changes: Encourage the patient to move often.
Comfort and Support:
Warm Compresses: Intermittent or continuous for pain relief.
Leg Measurement: Regular checks for swelling.
Precautions and Safety:
No Leg Massages: To prevent clot dislodgment and embolism.
Antiembolism Stockings: For patients at high risk.
Medications:
Analgesics (NSAIDs)
Anticoagulants
Heparin
Classification: Anticoagulant
Purpose:
Initial treatment of DVT and Acute Pulmonary Embolism (PE)
Prevents new clots and enlargement of existing ones.
Administration: IV infusion with dose adjustments based on aPTT levels.
aPTT Monitoring: Target is 1.5 to 2.5 times the control level (30 to 40 seconds).
Antidote: Protamine sulfate – for reversing Heparin effects.
Nursing Actions:
Monitor aPTT regularly.
Have Protamine sulfate readily available.
Client Education:
Report signs of bleeding:
Gums, nose, vaginal bleeding, blood in urine, or bruising.
Avoid Certain Medications and Substances:
No aspirin or ibuprofen (increases bleeding).
No alcohol (interferes with Warfarin).
Safety Measures:
Use an electric razor for shaving.
Use a soft toothbrush to prevent gum bleeding.
Movement and Positioning:
No massaging or rubbing legs (prevents clot dislodgement).
No prolonged sitting or crossing legs (prevents blood pooling).
Warfarin
Classification: Anticoagulant
Purpose: Long-term treatment of DVT.
Administration: Oral, requires close monitoring of PT and INR levels.
Target INR: Usually between 2.0 and 3.0.
Antidote: Phytonadione (Vitamin K)
Nursing Actions:
Monitor PT and INR levels regularly.
Have Vitamin K readily available.
Client Education:
Bleeding Precautions: Same as Heparin (gums, nose, vaginal bleeding, urine, bruising).
Pregnancy Risk: Use non-hormonal birth control (warfarin is teratogenic).
No Oral Contraceptives: Increases risk for blood clots.
Avoid Certain Medications and Substances:
No aspirin or ibuprofen (increases bleeding).
No alcohol (interferes with Warfarin).
Safety Measures:
Use an electric razor for shaving.
Use a soft toothbrush to prevent gum bleeding.
Movement and Positioning:
No massaging or rubbing legs (prevents clot dislodgement).
No prolonged sitting or crossing legs (prevents blood pooling).
Anticoaguiant Precautions
Avoid Certain Medications and Substances:
No aspirin or ibuprofen (increases bleeding).
No alcohol (interferes with Warfarin).
Safety Measures:
Use an electric razor for shaving.
Use a soft toothbrush to prevent gum bleeding.
Movement and Positioning:
No massaging or rubbing legs (prevents clot dislodgement).
No prolonged sitting or crossing legs (prevents blood pooling).
Pulmonary Embolus
When a blood clot dislodges and travels to the pulmonary artery, blocking blood flow to the lungs.
It is a life-threatening emergency and is a complication of Deep-Vein Thrombosis (DVT).
Risk Factors
Same as for DVT:
Pregnancy, Cesarean birth, obesity, smoking, immobility, age > 35, history of thromboembolism, etc.
Pulmonary Embolus S/S
Respiratory Symptoms:
Dyspnea: Difficulty breathing.
Tachypnea: Rapid breathing.
Cough (may produce blood, called hemoptysis).
Crackles upon lung auscultation.
Hypoxia: Low oxygen levels.
Cardiovascular Symptoms:
Tachycardia: Fast heart rate.
Syncope: Fainting due to low oxygen.
Other Symptoms:
Apprehension and Anxiety: Feeling of impending doom.
Pleuritic Chest Pain: Sharp pain worsening with breathing.
Elevated Temperature: Mild fever.
Pulmonary Embolus Dx
Imaging and Scans:
Ventilation/Perfusion (V/Q) Scan: Assesses airflow and blood flow in lungs.
Magnetic Resonance Angiography (MRA): Detailed imaging of blood vessels.
Spiral Computed Tomography (CT): High-resolution lung imaging.
Pulmonary Angiogram: Direct visualization of lung vessels.
Surgical Intervention:
Embolectomy: Surgical removal of the embolus if life-threatening.
Pulmonary Embolus Care
Nursing Care
Semi-Fowler’s Position: Head of the bed elevated to improve breathing.
Administer Oxygen: Via mask to relieve hypoxia.
Surgical Intervention:
Embolectomy: Surgical removal of the embolus if life-threatening.
Medications
Anticoagulants:
Same as DVT treatment (Heparin, Warfarin).
Prevents new clots and stops existing ones from getting bigger.
Thrombolytic Therapy:
Purpose: Breaks up existing blood clots.
Common Drugs:
Alteplase
Streptokinase
Precautions:
Similar adverse effects and contraindications as anticoagulants (e.g., increased risk of bleeding).
Coagulopathies
Disorders that affect the blood's ability to clot, leading to excessive bleeding. Two main types are:
Idiopathic Thrombocytopenic Purpura (ITP):
Cause: Autoimmune bleeding disorder where platelets are destroyed by antibodies.
Risk: Severe bleeding after cesarean birth or lacerations.
Disseminated Intravascular Coagulation (DIC):
Cause: Simultaneous clotting and bleeding due to overactive clotting factors.
Risk: Internal and external bleeding, organ damage from microclots.
Trigger: Often after failure of uterine contraction stimulation to stop bleeding.
Expected Findings (Signs and Symptoms)
Bleeding Symptoms:
Spontaneous Bleeding: From gums or nose (Epistaxis).
Oozing or Trickling Blood: From incision sites, lacerations, or episiotomy.
Petechiae and Ecchymosis: Small red/purple spots and bruising.
Excessive Bleeding: From needle punctures or slight trauma.
Hematuria: Blood in urine.
Gastrointestinal Bleeding: Blood in stool or vomit.
Cardiovascular and Systemic Symptoms:
Tachycardia: Fast heart rate.
Hypotension: Low blood pressure.
Diaphoresis: Excessive sweating.
Idiopathic Thrombocytopenic Purpura (ITP)
Disorders that affect the blood's ability to clot, leading to excessive bleeding.
Cause: Autoimmune disorder where platelets are destroyed by antibodies.
Risk: Severe bleeding after cesarean birth or lacerations.
Risk Factor
Genetic origin.
Disseminated Intravascular Coagulation (DIC)
Disorders that affect the blood's ability to clot, leading to excessive bleeding.
Cause: Simultaneous clotting and bleeding due to overactive clotting factors.
Risk: Internal and external bleeding, organ damage from microclots.
Trigger: Often after failure of uterine contraction stimulation to stop bleeding.
Risk Factor (Usually secondary to other conditions)
Abruptio Placentae (most common cause).
Amniotic Fluid Embolism – Amniotic fluid enters maternal circulation.
Missed Abortion – Fetal death retained in uterus ≥6 weeks.
Fetal Death in Utero – Retained deceased fetus.
Severe Preeclampsia/Eclampsia – Gestational hypertension, HELLP syndrome.
Septicemia – Blood infection.
Cardiopulmonary Arrest – Heart and lung failure.
Hemorrhage – Excessive bleeding.
Hydatidiform Mole – Abnormal pregnancy growth.
Coagulopathies Labs
CBC with Differential: Checks overall blood count.
Blood Typing and Crossmatch: Prepares for blood transfusion.
Clotting Factors to Monitor
Platelet Levels: Decreased (Thrombocytopenia)
Fibrinogen Levels: Decreased (Less clot formation)
Prothrombin Time (PT): Prolonged (Longer to clot)
Fibrin Split Product Levels: Increased (Breakdown of clots)
D-dimer Test: Increased (Indicates clot breakdown)
Coagulopathies Care
Bleeding Assessment and Monitoring:
Check skin, injection sites, lacerations, and episiotomy for bleeding.
Monitor vital signs and hemodynamic status (heart rate, blood pressure).
Observe urinary output using a catheter if needed (assesses kidney perfusion).
Transfusions and Medication:
Transfuse: Platelets, clotting factors, blood products, or volume expanders.
Pharmacologic Interventions: Antibiotics, vasoactive drugs, and uterotonic agents (for DIC).
Surgical Preparation and Support:
Splenectomy Preparation: If ITP doesn't respond to medication.
Hysterectomy for DIC: If bleeding is uncontrollable.
Oxygenation and Injury Prevention:
Ensure optimal oxygenation with supplemental oxygen if needed.
Protect from injury to minimize bleeding risks.
Therapeutic Procedures
Correction of Underlying Cause:
Example: Removal of dead fetus, treating infection.
Splenectomy (for ITP):
Performed if ITP is resistant to medication.
Hysterectomy (for DIC):
Done in severe cases of DIC with uncontrolled bleeding.
DIC Nursing Care
Identify and Treat Underlying Cause:
Examples: Placental abruption, fetal death, infection, preeclampsia.
Fluid Volume Replacement:
Administer blood and blood products to maintain circulation.
Medications:
Use antibiotics for infections and vasoactive medications for blood pressure control.
Oxygen and Safety Measures:
Supplemental oxygen and injury prevention.
Hysterectomy for uncontrolled bleeding
Postpartum hemorrhage
Definition (ACOG):
Blood loss of 1,000 mL or more within 24 hours after childbirth.
Or any blood loss causing hypovolemia (low blood volume).
Complications
Hypovolemic Shock: Leading to decreased organ perfusion.
Anemia
Guidelines
Early Identification of Risk Factors:
Essential for preventing postpartum hemorrhage.
Interprofessional Collaboration:
Nurses should work with the healthcare team for rapid intervention.
Quantification of Blood Loss (QBL):
Recommended with every birth for accurate measurement of blood loss (AWHONN).
Postpartum hemorrhage Risk Factors
Uterine Causes:
Uterine Atony: Weak or boggy uterus (most common cause).
Overdistended Uterus: Due to large baby, multiple pregnancies, or excess amniotic fluid.
Ruptured Uterus
Inversion of Uterus:
Subinvolution of Uterus: Uterus does not return to pre-pregnancy size.
Labor and Delivery Factors:
Prolonged Labor or Oxytocin-Induced Labor
Precipitous Delivery: Very rapid labor and birth.
High Parity: Multiple pregnancies (5 or more).
Lacerations and Hematomas
Retained Placental Fragments
Medical Interventions and Conditions:
Magnesium Sulfate Therapy: Used for preeclampsia.
Complications During Pregnancy:
Placenta Previa (placenta covers cervix).
Abruptio Placentae (placenta separates from uterus).
Coagulopathies: Blood clotting disorders (e.g., DIC).
Postpartum hemorrhage S/S
Lochia Changes:
Increase or change in lochia pattern (heavy bleeding or large clots).
Physical Assessment Findings:
Uterine Atony: Soft or boggy uterus upon palpation.
Blood Clots: Larger than a quarter.
Pad Saturation: Soaking a pad in 15 minutes or less.
Active Bleeding: Continuous oozing or trickling of bright red blood.
Tachycardia and Hypotension: Rapid pulse and low blood pressure.
Pallor and Clammy Skin: Pale, cold, and sweaty skin indicating shock.
Oliguria: Reduced urine output
Postpartum hemorrhage Labs
Hemoglobin (Hgb) and Hematocrit (Hct):
To assess blood loss and anemia.
Coagulation Profile:
Prothrombin Time (PT): Evaluates blood clotting function.
Blood Type and Crossmatch:
In case a blood transfusion is needed.
Postpartum hemorrhage Care
Quantification of Blood Loss (QBL):
Measure QBL immediately after birth by weighing blood-soaked items and calculating fluid volume.
Uterine Assessment and Management:
Fundal Massage: Firmly massage the uterine fundus if boggy to stimulate contractions.
Fundus Assessment: Check height, firmness, and position.
Bleeding and Vital Sign Monitoring:
Monitor for bleeding from lacerations, episiotomy, or hematomas.
Monitor vital signs for tachycardia, hypotension, and signs of shock.
Fluid and Blood Replacement:
IV Fluids: Isotonic solutions (e.g., Lactated Ringer's or Normal Saline).
Blood Products: Packed RBCs or fresh frozen plasma as needed.
Oxygen Therapy: 10-12 L/min via nonrebreather mask.
Positioning: Elevate legs to 20°-30° to improve circulation to vital organs.
Client Education
Activity and Nutrition:
Limit physical activity to conserve strength.
Increase iron and protein intake to rebuild RBC volume.
Take Vitamin C to enhance iron absorption.
Warning Signs to Report:
Excessive bleeding or passing large clots.
Dizziness or feeling faint (signs of hypovolemia).
Postpartum hemorrhage & Uterine Atony Medications
1. Oxytocin (Uterine Stimulant)
Purpose: Promotes uterine contractions.
Nursing Actions:
Monitor uterine tone and vaginal bleeding.
Watch for water intoxication (nausea, headache, malaise, seizures).
2. Methylergonovine (Uterine Stimulant)
Purpose: Controls postpartum hemorrhage.
Contraindication: Hypertension.
Nursing Actions:
Monitor uterine tone and vaginal bleeding.
Watch for adverse effects like hypertension, nausea, and headache.
3. Misoprostol (Uterine Stimulant)
Purpose: Controls postpartum hemorrhage.
Nursing Actions:
Monitor uterine tone and vaginal bleeding.
4. Carboprost Tromethamine (Uterine Stimulant)
Purpose: Controls postpartum hemorrhage.
Nursing Actions:
Monitor uterine tone and vaginal bleeding.
Watch for adverse reactions: fever, hypertension, chills, headache, nausea, vomiting, and diarrhea.
5. Tranexamic Acid (Antifibrinolytic)
Purpose: Enhances blood clotting.
Indication: For PPH within 3 hours of birth.
Nursing Actions:
Monitor vaginal bleeding and coagulation status.
Uterine Atony
The inability of the uterine muscle to contract adequately after childbirth, leading to postpartum hemorrhage.
Risk Factors
Placental and Labor Issues:
Retained Placental Fragments
Prolonged or Precipitous Labor (very long or very rapid labor)
Oxytocin Use: Induction or augmentation of labor.
Uterine Muscle Overdistention:
Multiparity: Multiple pregnancies.
Multiple Gestations: Twins or more.
Polyhydramnios: Excess amniotic fluid.
Macrosomic Fetus: Large baby.
Medications and Anesthesia:
Magnesium Sulfate: Used as a tocolytic (relaxes the uterus).
Anesthesia and Analgesia: Can relax the uterine muscle too much.
Trauma During Delivery:
Operative Delivery: Forceps, vacuum-assisted birth, or cesarean section.
Uterine Atony S/S
Increased Vaginal Bleeding
Often bright red and heavy.
Boggy Uterus: Soft, spongy, and larger than normal uterus.
Lateral Displacement: Possible shift to one side due to bladder distention.
Prolonged Lochial Discharge: Extended bleeding beyond the typical timeframe.
Irregular or Excessive Bleeding: Clots or continuous trickling of blood.
Vital Signs:
Tachycardia: Fast heart rate.
Hypotension: Low blood pressure.
Skin Appearance:
Pallor and Clammy Skin: Cool, pale, and loss of skin turgor (elasticity).
Uterine Atony Dx
Bimanual Compression:
Manual compression of the uterus by the healthcare provider to stop bleeding.
Surgical Management:
Removal of Retained Placental Fragments
Hysterectomy: In severe cases when other treatments fail.
Uterine Atony Care
Bladder Management:
Ensure Bladder is Empty: A full bladder can displace the uterus and worsen atony.
Uterine Assessment:
Fundal Checks: Monitor height, consistency, and location of the fundus.
Lochia Assessment: Observe quantity, color, and consistency.
Fundal Massage and Clot Expression:
Fundal Massage: Stimulates uterine contractions.
If the uterus becomes firm, continue monitoring.
If atony persists, anticipate surgical intervention (e.g., hysterectomy).
Clot Expression: Only after the uterus is firmly contracted.
Do NOT express clots on an uncontracted uterus—this can cause uterine inversion and severe hemorrhage.
Vital Sign Monitoring and Fluid Management:
Monitor Vital Signs: Watch for tachycardia, hypotension, and shock.
IV Fluids
Surgical Intervention: Required if other methods fail to stop bleeding and firm the uterus.
Uterine Tamponade: Intrauterine balloon to control hemorrhage.
If tamponade fails, hysterectomy may be necessary.
Removal of Retained Placental Fragments
Client Education
Explanation of Interventions:
Educate on rapid intervention and the purpose of procedures.
Activity and Nutrition Post-Stabilization:
Rest and Recovery: Limit physical activity to conserve strength.
Dietary Support:
Increase iron and protein intake to rebuild RBC volume.
Take Vitamin C to enhance iron absorption.
Subinvolution of the Uterus
A condition where the uterus fails to return to its normal size and shape after childbirth
Risk Factors
Pelvic Infection and Endometritis – Infection of the uterine lining.
Retained Placental Fragments – Incomplete expulsion of the placenta.
Subinvolution of the Uterus S/S
Vaginal Bleeding:
Prolonged Vaginal Bleeding – Lasts longer than expected postpartum.
Irregular or Excessive Bleeding – May include large clots.
Enlarged Uterus: Higher and larger than normal relative to the umbilicus.
Boggy Uterus: Soft and not firm upon palpation.
Prolonged Lochia Discharge: Irregular or excessive bleeding with foul odor (if infection is present).
Subinvolution of the Uterus Labs
Bacterial Cultures:
Blood, Intracervical, and Intrauterine Cultures
To check for infection and endometritis
Subinvolution of the Uterus Care
Nursing Care
Uterine and Lochia Monitoring:
Fundal Position and Consistency: Check for height, firmness, and location.
Lochia Assessment: Observe for color, amount, consistency, and odor.
Foul odor may indicate infection (endometritis).
Vital Signs Monitoring:
Monitor for tachycardia, hypotension, and fever (signs of hemorrhage or infection).
Promote Uterine Involution:
Breastfeeding: Stimulates oxytocin release, promoting uterine contractions.
Early and Frequent Ambulation: Encourages uterine drainage and contraction.
Frequent Voiding: Prevents bladder distention, which can impede uterine contraction.
Therapeutic Procedures
Dilation and Curettage (D&C):
Purpose:
Remove Retained Placental Fragments
Debride Placenta Insertion Site if needed to control bleeding.
Subinvolution of the Uterus Medications
Methylergonovine
Classification: Uterine Stimulant
Purpose:
Promotes uterine contractions to expel retained placental fragments.
Controls postpartum hemorrhage.
Nursing Actions:
Monitor uterine tone and vaginal bleeding.
Assess for signs of infection, such as uterine tenderness and foul-smelling lochia.
Contraindication:
Do NOT give to patients with hypertension.
Antibiotic Therapy
Purpose:
To prevent or treat infections such as endometritis.
Indication:
Ordered if infection is suspected or confirmed by bacterial cultures.
Inversion of the Uterus
When the uterus turns inside out and can be partial or complete.
It is a life-threatening emergency leading to severe postpartum hemorrhage and requires immediate intervention.
Risk Factors
Placental and Uterine Issues:
Retained Placenta – Prevents uterine contraction.
Uterine Atony – Weak uterine muscle tone.
Fundal Implantation of the Placenta – Placenta attached to the upper uterine wall.
Abnormally Adherent Placental Tissue – Such as placenta accreta.
Labor and Delivery Factors:
Vigorous Fundal Pressure – Excessive pressure on the fundus during delivery.
Excessive Traction on Umbilical Cord – Pulling too hard on the umbilical cord.
Prolonged Labor
Other Risk Factors:
Tocolysis – Medications that relax the uterus.
Fetal Macrosomia – Large baby.
Nulliparity – First-time pregnancy.
Short Umbilical Cord
Inversion of the Uterus S/S
Severe Lower Abdominal Pain – Sudden and intense.
Vaginal Bleeding and Physical Assessment Findings:
Hemorrhage – Severe vaginal bleeding.
Uterine Protrusion:
Complete Inversion: Fundus visible as a mass in the vagina.
Prolapsed Inversion: Large, red mass outside the vagina (20-30 cm).
Incomplete Inversion: Smooth mass felt through the dilated cervix.
Vital Signs and Systemic Symptoms:
Dizziness
Hypotension and Tachycardia – Low blood pressure and rapid pulse (shock).
Pallor – Pale skin indicating poor circulation.
Inversion of the Uterus Care
Nursing Care
Assessment and Recognition:
Visualize the Introitus: Look for uterine tissue protruding through the vaginal opening.
Perform Pelvic Exam to confirm the diagnosis of uterine inversion.
Supportive Care and Stabilization:
Maintain IV Fluids
Administer Oxygen
Stop Oxytocin: If being given at the time of inversion, as it may worsen the condition.
Avoid Excessive Traction on the Umbilical Cord to prevent further inversion.
Prepare for Medical and Surgical Intervention:
Anticipate Surgery if manual repositioning is unsuccessful.
Prepare for Manual Replacement: Get necessary equipment ready for the provider.
Therapeutic Procedures
Manual Replacement of the Uterus:
Manual Repositioning by the healthcare provider to place the uterus back in the pelvic cavity.
Repositioning of the Uterus to its normal anatomical position.
Inversion of the Uterus Medications
Terbutaline
Classification: Tocolytic
Purpose: Relaxes the uterus before the provider attempts manual repositioning of the uterus.
Nursing Actions:
Observe Client's Response: After repositioning, closely monitor for stabilization of vital signs.
Avoid Aggressive Fundal Massage – It can reinvert the uterus.
Administer Oxytocics: Once the uterus is repositioned to promote contractions and prevent re-inversion.
Antibiotic Prophylaxis: Administer broad-spectrum antibiotics to prevent infection.
Retained Placenta
When placental tissue remains in the uterus beyond 30 minutes after childbirth.
This prevents the uterus from contracting properly, leading to uterine atony or subinvolution, and can cause postpartum hemorrhage.
Risk Factors
Placental Separation Issues:
Partial Separation of a normal placenta.
Entrapment by Constricting Ring: Placenta trapped by a constriction in the uterus.
Excessive Traction on Umbilical Cord before complete placental separation.
Placental Adhesion Abnormalities:
Abnormal Adherence: Such as placenta accreta (attached too deeply).
Other Risk Factors:
Preterm Births: Between 20 and 24 weeks of gestation.
Retained Placenta S/S
Vaginal Bleeding and Uterine Issues:
Uterine Atony, Subinvolution, or Inversion – Soft, boggy uterus.
Excessive Bleeding – Blood clots larger than a quarter.
Return of Lochia Rubra – Bright red bleeding after progression to pink or white lochia.
Infection Signs:
Malodorous Lochia or Vaginal Discharge – Foul-smelling discharge.
Elevated Temperature – Possible fever indicating infection.
Retained Placenta Labs
Hemoglobin (Hgb) and Hematocrit (Hct):
To assess blood loss and anemia.
Retained Placenta Care
Uterine and Lochia Monitoring:
Fundal Assessment: Monitor for height, consistency, and position.
Lochia Assessment: Observe for color, amount, consistency, and odor.
Foul odor may indicate infection (endometritis).
Vital Signs Monitoring:
Monitor for tachycardia, hypotension, and fever (signs of hemorrhage or infection).
Fluid Management and Surgical Preparation:
IV Fluids: Maintain or initiate to stabilize blood pressure.
Surgical Intervention:
Dilation and Curettage (D&C): Performed if oxytocics are ineffective in expelling placental fragments..
Hysterectomy: In severe cases if bleeding persists.
Manual Removal: Manual Separation and Removal of the placenta by the healthcare provider.
Client Education
Activity and Nutrition Post-Stabilization:
Rest and Recovery: Limit physical activity to conserve strength.
Dietary Support:
Increase iron and protein intake to rebuild RBC volume.
Take Vitamin C to enhance iron absorption.
Warning Signs to Report:
Excessive bleeding, fever, foul-smelling discharge, or dizziness.
Retained Placenta Medications
Oxytocin
Classification: Uterine Stimulant
Purpose:
Promotes uterine contractions to expel retained placental fragments.
Nursing Actions:
Monitor Uterine Tone and Vaginal Bleeding.
Watch for Water Intoxication: Symptoms include:
Lightheadedness, Nausea, Vomiting, Headache, Malaise.
Severe cases can lead to cerebral edema, seizures, coma, and death.
Lacerations
Tearing of soft tissues during labor and birth.
Can affect the cervical, vaginal, vulvar, perineal, and/or rectal areas.
Types:
Spontaneous Occur naturally during childbirth.
Episiotomy Extension: A planned surgical cut that may extend to become a third or fourth-degree
Complication: Hemorrhage
Hematomas
A collection of clotted blood within tissues, appearing as a bulging bluish mass.
Can occur in the pelvic region, vagina, or broad ligament.
Key Symptom:
Pain (not bleeding)
Complication: Infection & Hemorrhage
Lacerations and Hematomas Risk Factors
Labor and Delivery Factors:
Operative Vaginal Birth: Forceps or vacuum-assisted delivery.
Precipitous Birth: Very rapid labor and birth.
Cephalopelvic Disproportion: Baby's head too large for the maternal pelvis.
Abnormal Fetal Presentation: Breech or transverse lie.
Macrosomic Infant: Large baby (>4000 g).
Prolonged Pressure: Fetal head pressure on vaginal mucosa.
Maternal History:
Previous Scarring: From infection, injury, or surgery in the birth canal.
Lacerations S/S
Sensation of Oozing or Trickle of Blood – Continuous flow.
Excessive Vaginal Bleeding – With or without clots.
Vaginal Bleeding despite a firm and contracted uterus.
Continuous Slow Trickle of bright red blood from:
Vagina, Laceration Site, or Episiotomy.
Hematomas S/S
Persistent Perineal or Rectal Pain – Unrelieved by analgesics.
Difficulty Voiding – Due to pressure or swelling.
Bulging Bluish Mass or Red-Purple Discoloration on:
Vulva, Perineum, or Rectum.
Area is Painful and Firm on palpation.
Lacerations and Hematomas Care
Assessment and Monitoring:
Pain Assessment: Evaluate location, intensity, and type of pain.
Visual Inspection:
Inspect the vulva, perineum, and rectum for lacerations and hematomas.
Lochia Evaluation:
Monitor for color, amount, consistency, and odor to assess bleeding.
Vital Signs:
Check for tachycardia, hypotension, and other shock symptoms.
Bleeding Identification and Support:
Identify the Source: Attempt to locate the bleeding site.
Assist with Repair Procedures: Help the provider during suturing or evacuation.
Pain Management and Comfort:
Ice Packs: Apply to small hematomas within the first 24 hours to reduce swelling.
Sitz Baths: After 24 hours to promote healing and relieve pain.
Pain Medication: Administer analgesics as prescribed.
Hygiene and Education:
Perineal Hygiene: Encourage frequent cleaning to prevent infection.
Patient Education:
Teach signs of infection: Fever, foul-smelling discharge, or increased pain.
Instruct on proper perineal care and sitz bath usage.
Therapeutic Procedures
Suturing and Repair
Hematoma Management:
Ligation of Bleeding Vessel: To stop bleeding from the injured vessel.
Surgical Incision and Evacuation:
Incision to drain clotted blood from large masses
Chapter 21: Postpartum Infections
Diagnostic Criteria
Fever of 38°C (100.4°F) or higher:
After the first 24 hours postpartum, OR
For 2 days during the first 10 days postpartum.
Types of Postpartum Infections
Uterine Infection (Endometritis):
Infection of the uterine lining.
Wound Infection:
At the site of episiotomy, cesarean incision, or laceration.
Mastitis:
Breast infection typically involving the milk ducts.
Urinary Tract Infection (UTI):
Infection in the bladder or urinary tract.
Major Complication
Septicemia (Sepsis):
A life-threatening bloodstream infection resulting from untreated postpartum infection.
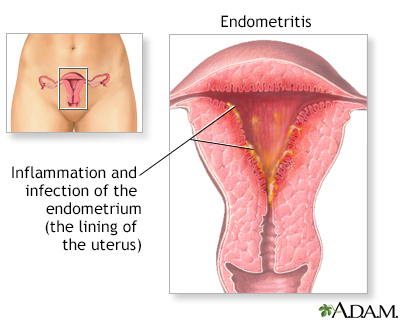
Uterine Infection (Endometritis)
Most common puerperal infection after childbirth.
Onset and Progression:
Usually begins on the 3rd to 4th postpartum day.
Starts as a localized infection at the placental site.
Can spread to the entire uterine lining if untreated.
Wound Infections
Sites of Infection:
Cesarean Incisions
Episiotomies and Lacerations
Trauma Wounds from delivery (e.g., forceps or vacuum-assisted birth).

Mastitis
Usually unilateral
Involves the interlobular connective tissue.
Onset and Timing:
Can occur as early as the 7th postpartum day.
Most common during the first 6 weeks of breastfeeding but can happen anytime during lactation.
Staphylococcus aureus is the most common causative organism.
Complications:
Can progress to an abscess if untreated.
Encourage complete emptying of breasts to prevent milk stasis
Mastitis Risk Factors
1. Milk Stasis
Milk buildup in the breast due to blocked ducts or engorgement.
Causes:
Blocked Duct: From improper latch or infrequent feeding.
Engorgement: Overfull breasts without adequate milk removal.
Tight Bras or Underwire: Restricts milk flow.
2. Nipple Trauma
Cracked or Fissured Nipples:
Due to poor latching technique or improper positioning.
Provides entry point for bacteria.
3. Poor Breastfeeding Technique
Improper Latch:
Leads to sore and cracked nipples.
Incomplete emptying of the breast.
4. Decreased Breastfeeding Frequency
Causes:
Supplementation with Bottle Feeding: Reduces breastfeeding frequency.
Skipping Feedings: Leads to milk stasis and engorgement.
5. Contamination of Breasts
Poor Hygiene:
Introduces bacteria from hands, skin, or environment.
Postpartum Infections: Endometritis, Mastitis, and Wound Infections
1. Uterine Infection (Endometritis)
Definition:
Infection of the uterine lining (endometrium).
Most common puerperal infection after childbirth.
Onset and Progression:
Usually begins on the 3rd to 4th postpartum day.
Starts as a localized infection at the placental site.
Can spread to the entire uterine lining if untreated.
2. Wound Infections
Sites of Infection:
Cesarean Incisions
Episiotomies and Lacerations
Trauma Wounds from delivery (e.g., forceps or vacuum-assisted birth).
3. Mastitis
Definition:
Infection of the breast tissue, usually unilateral (one breast).
Involves the interlobular connective tissue.
Onset and Timing:
Can occur as early as the 7th postpartum day.
Most common during the first 6 weeks of breastfeeding but can happen anytime during lactation.
Staphylococcus aureus is the most common causative organism.
Complications:
Can progress to an abscess if untreated.
Postpartum Infections Risk Factors
1. Pre-Existing Conditions:
Infections:
UTI, Mastitis, Pneumonia, or Previous Venous Thrombosis.
Chronic Conditions:
Diabetes Mellitus, Immunosuppression, Anemia, Malnutrition.
Substance Use:
Alcohol or Substance Use Disorder.
2. Labor and Delivery Factors:
Cesarean Birth: Higher risk due to surgical incision.
Prolonged Labor: Extended exposure to potential pathogens.
Operative Vaginal Birth: Use of forceps or vacuum extraction.
Postpartum Hemorrhage: Increased risk of infection.
3. Procedural and Intervention-Related Risks:
Premature Rupture of Membranes: Leads to potential ascending infections.
Retained Placental Fragments: Prevents proper uterine contraction and clearance.
Manual Extraction of the Placenta: Direct manipulation increases infection risk.
Bladder Catheterization: Risk of urinary tract infection.
Intrauterine Infections:
Internal Fetal/Uterine Pressure Monitoring.
Multiple Vaginal Exams after rupture of membranes.
4. Anesthesia and Tissue Trauma:
Epidural Analgesia/Anesthesia: Can suppress immune response.
Hematomas: Create an environment for bacterial growth.
Episiotomy or Lacerations: Open wounds prone to infection.
Endometritis (Uterine Infection) S/S
Pelvic Pain
Chills and Fatigue
Loss of Appetite
Uterine Tenderness
Dark, Profuse Lochia
May be malodorous or purulent (foul-smelling or pus-like).
Fever ≥ 38°C (100.4°F)
Tachycardia
Endometritis (Uterine Infection) Management & Discharge
Vaginal and Blood Cultures if prescribed.
IV Antibiotics and Analgesics as ordered.
Clindamycin
Cephalosporins, Penicillins, and Gentamicin
Wound Management:
Incision and Drainage:
If the wound is abscessed or has purulent drainage.
Wound Debridement:
Removal of necrotic tissue to promote healing.
Effective Hand Hygiene to prevent spread of infection.
Maintain interaction with the newborn for bonding.
Medication Adherence:
Complete the full course of antibiotics as prescribed.
Notify the provider if experiencing:
Watery, bloody diarrhea (sign of Clostridium difficile infection).
Allergic reactions (rash, itching, difficulty breathing).
Inform the provider if breastfeeding to ensure safe medication use.
Mastitis (Breast Infection) S/S
Tender, Red, Swollen Breast Area
Usually unilateral (one side).
Enlarged, Tender Axillary Lymph Nodes
Swollen, Warm, and Tender area of inflammation.
Flu-like Symptoms:
Chills, Fever, Body Aches
Fatigue
Mastitis (Breast Infection) Management & Discharge
Antibiotics to treat infection.
Pain Management:
Ice Packs for pain relief.
Warm Packs before breastfeeding to encourage milk flow.
Breast Hygiene and Feeding Practices:
Wash Hands before breastfeeding.
Change breast pads frequently to keep the area dry.
Proper Latch Technique to prevent nipple trauma.
Breastfeeding Continuation:
Continue feeding every 2-4 hours, especially on the affected side.
Manually express milk or pump if breastfeeding is too painful.
Fluid Intake and Nutrition:
3,000 mL/day of fluids for hydration and milk production.
High protein intake for tissue repair and healing.
Clothing and Support:
Wear a well-fitting bra without underwire for support.
Warning Signs to Report:
Increased redness, pain, fever, or malaise.
Wound Infections S/S
Signs of Local Inflammation:
Warmth, Erythema, Tenderness, Pain, Edema (swelling)
Seropurulent Drainage: Cloudy or yellowish discharge.
Wound Dehiscence:
Separation of the wound edges.
May include evisceration (protrusion of internal contents).
Fever ≥ 38°C (100.4°F)
Wound Infection Management & Discharge
Wound Care and Hygiene: Keep the area clean and dry.
IV or Oral Antibiotics as prescribed.
Comfort Measures:
Sitz Baths, Perineal Care, Warm or Cold Compresses.
Good Hygiene Techniques:
Change perineal pads front to back.
Perform thorough hand hygiene before and after perineal care.
Postpartum Infections Expected Findings
1. General Puerperal Infections:
Flu-like Symptoms:
Body Aches, Chills, Fever, Malaise
Gastrointestinal Symptoms:
Anorexia and Nausea
Fever:
≥ 38°C (100.4°F) for 2 or more consecutive days
Tachycardia:
Increased heart rate as a response to infection.
2. Endometritis (Uterine Infection):
Pelvic Pain
Chills and Fatigue
Loss of Appetite
Uterine Tenderness
Dark, Profuse Lochia
May be malodorous or purulent (foul-smelling or pus-like).
Fever ≥ 38°C (100.4°F)
Tachycardia
3. Mastitis (Breast Infection):
Tender, Red, Swollen Breast Area
Usually unilateral (one side).
Enlarged, Tender Axillary Lymph Nodes
Swollen, Warm, and Tender area of inflammation.
Flu-like Symptoms:
Chills, Fever, Body Aches
Fatigue
4. Wound Infection:
Signs of Local Inflammation:
Warmth, Erythema, Tenderness, Pain, Edema (swelling)
Seropurulent Drainage: Cloudy or yellowish discharge.
Wound Dehiscence:
Separation of the wound edges.
May include evisceration (protrusion of internal contents).
Fever ≥ 38°C (100.4°F)
Postpartum Infections Labs
Bacterial Cultures:
Blood, Intracervical, Intrauterine to identify the organism.
WBC Count:
Leukocytosis (Increased white blood cells).
RBC Sedimentation Rate:
Increased (indicates inflammation).
RBC Count:
Anemia due to infection or hemorrhage.
Postpartum Infections Management & Discharge
General Assessment and Monitoring:
Frequent Vital Signs: Monitor for fever and tachycardia.
Pain Assessment: Determine location, intensity, and nature of pain.
Fundal Checks: Monitor height, position, and consistency for uterine involution.
Lochia Observation: Assess for color, quantity, consistency, and odor.
Inspect Incisions and Lacerations: Look for redness, swelling, drainage, or separation.
Breast Inspection: Assess for redness, warmth, tenderness, or lumps.
Infection Control and Prevention:
Aseptic Technique: During procedures and perineal care.
Proper Hand Hygiene: Before and after patient contact.
Use Gloves: During labor, birth, and postpartum care.
Supportive Care and Comfort Measures:
Maintain IV Access: For antibiotics and fluid administration.
Administer Broad-Spectrum Antibiotics:
Penicillins, Cephalosporins, Clindamycin, Gentamicin as prescribed.
Comfort Measures:
Warm Blankets or Cool Compresses depending on symptoms.
General Education for Puerperal Infections:
Signs of Worsening Infection: Report fever, increased pain, or foul-smelling discharge.
Adherence to Antibiotics: Complete the full course to prevent resistance.
Hygiene Practices:
Handwashing and proper perineal care (front to back wiping).
Dietary Recommendations:
High protein intake to promote tissue healing.
Urinary Tract Infection (UTI)
Common postpartum infections due to bladder trauma during delivery or poor aseptic technique during catheterization.
Complication: Can progress to pyelonephritis (kidney infection) and potentially lead to kidney failure.
Risk Factors
Bladder and Urethral Issues:
Postpartum Hypotonic Bladder or Urethra: Leads to urinary stasis and retention.
Urinary Catheterization: Increased risk of infection.
Anesthesia and Delivery Factors:
Epidural Anesthesia: Causes urinary retention and stasis.
Cesarean Birth: Increased risk due to surgical manipulation.
Procedures and History:
Frequent Pelvic Examinations – Introduces bacteria.
History of UTIs – Higher risk of recurrence.
Trauma and Injury:
Genital Tract Injuries: From birth trauma (e.g., lacerations).
Urinary Tract Infection (UTI) S/S
Urinary:
Urgency, Frequency, Dysuria (painful urination), and Discomfort in the pelvic area.
Cloudy, Blood-Tinged, or Malodorous Urine with sediment visible.
Systemic:
Fever, Chills, and Malaise (generalized feeling of discomfort).
Vital Signs:
Elevated Temperature and tachycardia.
Pain and Discomfort:
Urinary Retention – Inability to fully empty the bladder.
Suprapubic Pain – Above the pubic bone.
Costovertebral Angle (CVA) Tenderness – Indicates pyelonephritis.
Early Detection
Prevention Strategies:
Encourage Frequent Voiding – Every 2-4 hours to prevent stasis.
Proper Perineal Hygiene: Front-to-back wiping.
Adequate Hydration: Encourage fluid intake of at least 3,000 mL/day.
Urinary Tract Infection (UTI) Labs & Dx
Urinalysis:
Check for WBCs, RBCs, Protein, and Bacteria.
Urine Culture:
To identify the causative organism and determine antibiotic sensitivity.
Obtain Urine Sample:
Random or Clean-Catch Urine Sample for urinalysis and culture.
Urinary Tract Infection (UTI) Management & Discharge
Medication Administration:
Antibiotics:
Administer as prescribed and educate on the importance of completing the full course.
Pain Management:
Acetaminophen for discomfort and pain relief
Hygiene and Infection Prevention:
Proper Perineal Hygiene:
Teach wiping from front to back to prevent bacterial spread.
Hydration and Bladder Health:
Encourage Increased Fluid Intake:
At least 3,000 mL/day to dilute bacteria and flush the bladder.
Chapter 22: Postpartum Mental Health Disorders
1. Postpartum Blues
Occurrence:
Up to 85% of clients within the first few days after birth.
Lasts up to 10 days and resolves without intervention.
Symptoms:
Mood Swings, Anxiety, Sadness, Crying, Insomnia, Loss of Appetite.
Fatigue and irritability.
2. Postpartum Depression (PPD)
Occurrence:
Within 12 months of birth.
Affects 8% to 20% of new parents.
Occurs in 1 in 7 clients.
Symptoms:
Persistent Sadness, Intense Mood Swings, Anxiety, Irritability.
Loss of Appetite, Insomnia, Fatigue, and Loss of Interest in Normal Activities.
Risk Factors:
History of Depression, Anxiety, Bipolar Disorder.
Lack of Support, Stressful Life Events, Complicated Birth.
Complications:
Interference with Infant Care and Bonding.
Suicidal Thoughts and Harmful Intentions towards self or newborn.
3. Perinatal Mood Disorders (PMSs)
According to AWHONN:
Can occur anytime during pregnancy or first year postpartum.
Includes:
Depression, Bipolar Disorder, Anxiety, Postpartum Psychosis.
4. Postpartum Psychosis
Occurrence:
Within 2 to 3 weeks postpartum.
Higher risk in clients with bipolar disorder history.
Symptoms:
Confusion, Disorientation, Hallucinations, Delusions.
Obsessive Behaviors and Paranoia.
Complications:
Risk of Harm:
To self or newborn (e.g., suicidal or infanticidal thoughts).
Immediate Action Required:
Considered a psychiatric emergency.
Requires hospitalization and psychiatric intervention.
Postpartum Mood Disorders Risk Factors
1. Biological Factors:
Hormonal Changes:
Rapid decline in estrogen and progesterone levels after childbirth.
Medical Conditions:
Thyroid Imbalance, Diabetes, Infertility.
2. Psychological Factors:
History of Depression
Low Self-Esteem
Anxiety and Stress
3. Social and Environmental Factors:
Decreased Social Support
Socioeconomic Challenges
History of Partner Violence
4. Pregnancy and Birth-Related Factors:
Unintended Pregnancy:
Emotional distress and lack of preparedness.
Complications with Breastfeeding:
Difficulty with latching, milk supply issues, or pain.
Parent of Multiples:
Increased physical and emotional demands.
Younger Age
Postpartum Blues
Occurrence:
First few days postpartum, resolves by 10 days without intervention.
Symptoms:
Sadness, Anxiety, Irritability, Mood Swings
Crying Easily with no apparent reason.
Restlessness, Insomnia, Fatigue
Headache and Loss of Appetite
Feelings of Inadequacy or Anger
Physical Assessment Findings:
Crying
Postpartum Depression (PPD)
Occurrence:
Within 12 months postpartum.
Symptoms:
Feelings of Guilt and Inadequacy
Irritability, Anxiety, Intense Mood Swings
Persistent Sadness and Hopelessness
Feeling of Loss or Being Overwhelmed
Fatigue persisting beyond a reasonable time.
Sleep Pattern Disturbances (Insomnia or Hypersomnia)
Loss of Appetite or Overeating
Thoughts of Harming Self or Newborn
Physical Assessment Findings:
Crying, Weight Loss, Flat Affect (emotionless expression)
Irritability and Agitation
Rejection of the Newborn
Severe Anxiety and Panic Attacks
Postpartum Psychosis
Occurrence:
Within 2 to 3 weeks postpartum.
Psychiatric Emergency requiring immediate intervention.
Symptoms:
Pronounced Sadness or Depression
Confusion and Disorientation
Paranoia and Rapid Mood Swings
Delusions and Hallucinations (e.g., hearing voices)
Obsessive Thoughts or Delusions about the newborn.
Physical Assessment Findings:
Behaviors Indicating Hallucinations or Delusions
Self-Harm or Harm to Newborn Thoughts
Postpartum Mood Disorders Management & Discharge
1. Screening and Assessment
Routine Assessment:
During pregnancy and postpartum for perinatal mood disorders (PMDs).
Include questions about mood, anxiety, and thoughts of self-harm.
Postpartum Depression Screening:
Before discharge and reassessed at 4 weeks postpartum.
Use tools like the Edinburgh Postnatal Depression Scale.
2. Observation and Interaction
Monitor Interactions:
Client-Newborn Bonding: Encourage bonding activities (holding, feeding, talking to the newborn).
Observe Mood and Affect:
Watch for sadness, irritability, anxiety, detachment, or withdrawal.
3. Emotional Support and Communication
Normalize Feelings:
Reinforce that feeling down is normal in the postpartum period.
Encourage open communication about emotions.
Empathy and Validation
Adequate Rest: Nap when the newborn sleeps to avoid exhaustion.
Self-Time: Emphasize the importance of taking breaks and self-care.
4. Education and Reinforcement
Medication Adherence
Educate about signs of mood disorders and when to seek help.
Emphasize that postpartum blues are temporary but persistent sadness needs intervention.
5. Safety and Crisis Intervention
Assess for Suicidal or Harmful Thoughts:
Directly ask about self-harm, suicidal ideation, or thoughts of harming the newborn.
Immediate Intervention:
Ensure Safety: Priority is the safety of the newborn and client.
Psychiatric Referral for clients with severe depression or psychosis.
6. Community Resources and Follow-Up
Community Support:
Schedule Follow-Up Visits for clients at high risk for postpartum depression.
Connect clients with support groups, counseling, or mental health resources.
Social Support Involvement:
Involve partners and family for emotional and practical support.
Postpartum Depression (PPD) Management
Antidepressants:
Selective Serotonin Reuptake Inhibitors (SSRIs) like Sertraline (Zoloft) or Fluoxetine (Prozac).
Tricyclic Antidepressants (TCAs) if SSRIs are ineffective.
Postpartum Psychosis Management
Antipsychotics:
To manage hallucinations and delusions.
Mood Stabilizers:
For clients with bipolar disorder history.
Benzodiazepines:
To reduce anxiety and promote sleep.
Chapter 10: Early Onset of Labor
Understanding the importance of identifying the onset of early labor in a client who is pregnant is crucial for maternal and fetal well-being. This chapter includes preterm labor, prelabor rupture of membranes, and preterm prelabor rupture of membranes.
QEBP
Preterm Labor: Usually modified bed rest with bathroom privileges. Encourage the client to engage in activities that can be completed in bed or on the couch. Strict bed rest can have adverse effects.
Encourage the client to rest in the left lateral position to increase blood flow to the uterus and decrease uterine activity
Preterm Labor
Uterine contractions and cervical changes occurring between 20 and 36 weeks + 6 days of gestation.
Categories:
Very Preterm: < 32 weeks
Moderately Preterm: 32–34 weeks
Late Preterm: 34–36 weeks
Key Risk:
Shorter gestation = Higher neonatal risks.
Other Risk Factors:
Infections: UTI, vaginal infection, HIV, herpes, intrauterine infection.
Obstetric History: Previous preterm birth, multifetal pregnancy, uterine abnormalities.
Lifestyle Factors: Smoking, substance use, violence, lack of prenatal care.
Other: Low prepregnancy weight, advanced maternal age.
Preterm Labor S/S
Contractions, Cramping
Menstrual-like, pelvic pressure, persistent backache.
Gastrointestinal Symptoms: Cramping, diarrhea.
Urinary Symptoms: Frequency.
Vaginal Changes: Discharge (increased, foul-smelling, bloody).
Cervical Changes: Dilation, effacement.
Uterine Activity: Contractions every ≤10 min, lasting ≥1 hr.
Rupture of Membranes: Prelabor PROM.
Discomfort: Pelvic pressure, back pain.
Preterm Labor Labs/Dx
Fetal Fibronectin (fFN)
Presence between 24–34 weeks → ↑ risk of labor.
Cervical Cultures: Infection screening.
CBC & Urinalysis: Detect infections and inflammation.
Ultrasound
Cervical length <30mm = ↑ preterm labor risk.
Biophysical Profile & Nonstress Test: Assess fetal well-being.
Nursing Care for Preterm Labor
Goal: Stop uterine contractions and prevent progression
Activity Restriction:
Modified bed rest (with bathroom privileges).
Left lateral position → Improves uteroplacental blood flow, reduces contractions.
Avoid sexual intercourse → Can stimulate contractions.
Hydration:
Prevent dehydration → Reduces oxytocin release and contraction stimulation.
Identifying and Treating Infection:
Assess vaginal discharge (amount, color, consistency, odor).
Monitor vital signs & temperature → Fever and tachycardia suggest intrauterine infection.
Fetal Monitoring:
FHR & Contraction Pattern:
Fetal tachycardia (FHR >160 bpm) may indicate infection or fetal distress.
Nifedipine (Calcium Channel Blocker)
Action: Suppresses contractions by inhibiting __ entry into smooth muscles.
Nursing Actions:
Monitor for headache, flushing, dizziness, nausea (orthostatic hypotension).
Do not use with magnesium sulfate or beta-adrenergic agonists.
Client Education:
Change positions slowly to prevent dizziness.
Hydrate to counteract hypotension.
Magnesium Sulfate (CNS Depressant & Tocolytic)
Action: Relaxes smooth muscles, suppresses contractions, and provides fetal neuroprotection before 32 weeks.
Nursing Actions:
Contraindications: Vaginal bleeding, intrauterine infection, gestation >34 weeks, fetal distress.
Monitor closely for toxicity:
Pulmonary edema: Chest pain, respiratory distress, wheezing, productive cough.
Toxicity signs: Decreased deep tendon reflexes (DTRs), urine output <30 mL/hr, RR <12, severe hypotension.
Antidote: Calcium gluconate or calcium chloride.
Client Education:
Report blurred vision, nausea, vomiting, headache, or breathing difficulty.
Terbutaline (Beta-Adrenergic Agonist & Tocolytic)
Action: Relaxes smooth muscles to stop contractions.
Nursing Actions:
Contraindications: Cardiac disease, pregestational/gestational diabetes, preeclampsia, hyperthyroidism, hemorrhage.
Monitor for adverse effects:
Chest pain, tachycardia (>130 bpm), dysrhythmias, myocardial infarction.
Hypotension, tremors, hyperglycemia, nervousness.
Dosing: 0.25 mg subcutaneously every 4 hours (max 24 hours).
Discontinue if adverse effects occur.
Betamethasone (Glucocorticoid for Fetal Lung Maturity)
Action: Enhances fetal lung surfactant production for preterm infants 24–34 weeks gestation.
Nursing Actions:
Administer IM (12 mg, 2 doses, 24 hours apart).
Ideally, give at least 24 hours before birth (not more than 7 days prior).
Use ventrogluteal or vastus lateralis site for injection.
Monitor for maternal hyperglycemia.
Client Education:
Report signs of pulmonary edema (chest pain, shortness of breath, crackles).
Medications for Preterm Labor
1. Nifedipine (Calcium Channel Blocker)
Action: Suppresses contractions by inhibiting calcium entry into smooth muscles.
Nursing Actions:
Monitor for headache, flushing, dizziness, nausea (orthostatic hypotension).
Do not use with magnesium sulfate or beta-adrenergic agonists.
Client Education:
Change positions slowly to prevent dizziness.
Hydrate to counteract hypotension.
2. Magnesium Sulfate (CNS Depressant & Tocolytic)
Action: Relaxes smooth muscles, suppresses contractions, and provides fetal neuroprotection before 32 weeks.
Nursing Actions:
Contraindications: Vaginal bleeding, intrauterine infection, gestation >34 weeks, fetal distress.
Monitor closely for toxicity:
Pulmonary edema: Chest pain, respiratory distress, wheezing, productive cough.
Toxicity signs: Decreased deep tendon reflexes (DTRs), urine output <30 mL/hr, RR <12, severe hypotension.
Antidote: Calcium gluconate or calcium chloride.
Client Education:
Report blurred vision, nausea, vomiting, headache, or breathing difficulty.
3. Terbutaline (Beta-Adrenergic Agonist & Tocolytic)
Action: Relaxes smooth muscles to stop contractions.
Nursing Actions:
Contraindications: Cardiac disease, pregestational/gestational diabetes, preeclampsia, hyperthyroidism, hemorrhage.
Monitor for adverse effects:
Chest pain, tachycardia (>130 bpm), dysrhythmias, myocardial infarction.
Hypotension, tremors, hyperglycemia, nervousness.
Dosing: 0.25 mg subcutaneously every 4 hours (max 24 hours).
Discontinue if adverse effects occur.
4. Betamethasone (Glucocorticoid for Fetal Lung Maturity)
Action: Enhances fetal lung surfactant production for preterm infants 24–34 weeks gestation.
Nursing Actions:
Administer IM (12 mg, 2 doses, 24 hours apart).
Ideally, give at least 24 hours before birth (not more than 7 days prior).
Use ventrogluteal or vastus lateralis site for injection.
Monitor for maternal hyperglycemia.
Client Education:
Report signs of pulmonary edema (chest pain, shortness of breath, crackles).
PROM (Prelabor Rupture of Membranes)
Spontaneous rupture of amniotic membranes before the onset of true labor.
Risk Factors
Infection
Prior preterm birth
Cervical shortening
Second/third-trimester bleeding
Pulmonary/connective tissue disorders
Low BMI
Copper or vitamin C deficiency
Tobacco/substance use
pPROM (Preterm Prelabor Rupture of Membranes)
Rupture of membranes after 20 weeks but before 37 weeks of gestation, occurring before labor begins.
Risk Factors
Infection
Prior preterm birth
Cervical shortening
Second/third-trimester bleeding
Pulmonary/connective tissue disorders
Low BMI
Copper or vitamin C deficiency
Tobacco/substance use
Prelabor Rupture of Membranes (PROM/pPROM) S/S
Gush or leakage of clear fluid from the vagina
Presence of clear fluid
Assess for Prolapsed Umbilical Cord
Abrupt fetal heart rate (FHR) variability or prolonged deceleration
Visible or palpable cord at the vaginal opening
Prelabor Rupture of Membranes (PROM/pPROM) Labs
Nitrazine test: Positive if pH is 6.5 to 7.5 (blue color)
Fern test: Confirms amniotic fluid presence
Medications for Prelabor Rupture of Membranes (PROM/pPROM)
Ampicillin (Antibiotic)
Use: Treats intrauterine infections.
Nursing Actions: Obtain vaginal, urine, and blood cultures before administration.
Betamethasone (Glucocorticoid)
Use: Enhances fetal lung maturity and surfactant production in fetuses 24-34 weeks gestation.
Nursing Actions:
Administer 12 mg IM, two doses, 24 hours apart.
Use ventrogluteal or vastus lateralis muscle for injection.
Monitor for maternal hyperglycemia.
Client Education: Report pulmonary edema symptoms (chest pain, shortness of breath, crackles).
Ampicillin (Antibiotic)
Use: Treats intrauterine infections.
Nursing Actions: Obtain vaginal, urine, and blood cultures before administration.
Complications of Prelabor Rupture of Membranes (PROM/pPROM)
1. Infection
Intrauterine infection is the most common complication.
2. Other Complications
Placental abruption
Umbilical cord compression or prolapse
Fetal pulmonary hypoplasia
Fetal death
Client Education
Activity restriction – Limited activity with bathroom privileges.
Hydration – Drink plenty of fluids.
Monitor for labor signs – Self-assess uterine contractions.
Fetal movement tracking – Record daily kick counts.
Infection prevention
Report foul-smelling vaginal discharge.
Avoid inserting anything into the vagina (no intercourse, no tub baths).
Wipe perineal area front to back after voiding.
Take temperature every 4 hours and report >38°C (100°F).
Chapter 16: Complications Related to the Labor Process
Emergent Labor Complications
Immediate intervention is required for maternal-fetal safety in the following conditions:
Prolapsed umbilical cord
Meconium-stained amniotic fluid
Fetal distress
Dystocia (dysfunctional labor)
Precipitous labor
Uterine rupture
Amniotic fluid embolism (Anaphylactoid syndrome of pregnancy)
QEBP
Reposition the client in a knee-chest, Trendelenburg, or modified lateral semi-prone recumbent position with a rolled towel under the client’s right or left hip to relieve pressure on the cord.
Encourage the client to maintain a side-lying position to optimize uteroplacental perfusion and fetal oxygenation.
QS
Using a sterile-gloved hand, insert two fingers into the vagina, and apply finger pressure on either side of the cord to the fetal presenting part to elevate it off of the cord. Stay in this position until the birth of the baby.
Prolapsed Umbilical Cord
The umbilical cord slips ahead of the fetal presenting part, leading to cord compression and reduced fetal circulation.
Risk Factors:
Rupture of membranes (especially with unengaged fetal head)
Abnormal fetal presentations (breech, transverse lie)
Small-for-gestational-age fetus
Long umbilical cord
Multifetal pregnancy
Polyhydramnios (excess amniotic fluid)
Prolapsed Umbilical Cord S/S
Client reports feeling something in the vagina
Visible or palpable cord at the vaginal opening
FHR decelerations (variable/prolonged)
Excessive fetal movement followed by reduced movement (signs of hypoxia)
Prolapsed Umbilical Cord Care
Call for assistance & notify the provider immediately.
Do not leave the client alone.
Use a sterile-gloved hand to insert two fingers into the vagina and elevate the fetal presenting part off the cord. Maintain this position until delivery.
Reposition the client in knee-chest, Trendelenburg, or lateral recumbent position with a rolled towel under one hip.
Apply a warm, sterile, saline-soaked towel to prevent cord drying.
Monitor FHR continuously for signs of distress.
Administer oxygen via face mask and IV fluids as ordered.
Prepare for immediate delivery (vaginal if fully dilated, C-section if not).
Educate & support the client and partner about interventions.
Meconium-Stained Amniotic Fluid
Fetal stool is present in the amniotic fluid, indicating fetal bowel movement in utero.
Loss of fetal sphincter control due to hypoxia, maturity, or fetal distress.
Can occur before or during labor and may or may not indicate fetal compromise.
Risk Factors:
Common after 38 weeks gestation due to fetal maturity.
Umbilical cord compression → Fetal hypoxia → Stimulates vagal nerve → Sphincter relaxation → Meconium passage.
Meconium-stained amniotic fluid S/S
Color: Black, greenish, or yellow (often green).
Consistency: Thin or thick.
Meconium-stained amniotic fluid Dx
Electronic fetal monitoring to assess FHR patterns.