1.1 - NOT DONE overview of amputation
1/96
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
97 Terms
barbers
initially, who performed amputations?
50
nearly ______% with an amputation due to vascular disease die within 5 years
same mortality rate buuuuuut amputation doesn’t receive as much help (financially, research, etc.)
what is the main takeaway from the epidemiology when comparing people with cancer and amputations
lower
(upper or lower) amputations are more common
neuropathy and vascular conditions (dysvascuality)
what is the most common reason for an amputation
older; PVD is an accumulation/occurs over time
dysvascular amputations typically occur in (younger or older) people, why?
arteriosclerosis
chronic venous insufficiency
thromboangiitis obliterans (burgers disease - vessel spasm)
what are some of the examples of peripheral vascular diseases that can lead to a dysvascular cause of amputation
Foot trauma → wound → wound becomes infected → infection spreads to bone (osteomyelitis) → amputation to prevent life threatening systemic infection
what is the path that leads to a PVD cause for amputation
Trauma or deformity (e.g., charcot foot) → ulcerations (wound) → same process as PVD without DM
what is the path that leads to a diabetes cause for amputation
dysvascular → trauma → cancer → congenital anomalies
order the reasons for amputation from most common to least common
peripheral vascular disease
diabetes
what are the common conditions that fall under the “devascularization” cause for amputations
males
amputation due to trauma is most common in (females or males)
osteosarcoma
_____________ is the most common type of cancer that warrants an amputation
11-20 years
at what age does an amputation typically occur for someone with osteosarcoma
remove the function of inhibiting parts of the limb
create a normal residual limb for prosthetic
what are the 2 reasons for having surgery for a congenital limb difference
dysvascular
dysvascular or traumatic cause for amputation:
older
dysvascular
dysvascular of traumatic cause for amputation:
diabetic, overweight
dysvascualr
dysvascular of traumatic cause for amputation:
healing rate slowed due to poor circulation
dysvascualr
dysvascular of traumatic cause for amputation:
less active
dysvascular
dysvascular of traumatic cause for amputation:
more common for contralateral limb amputation
traumatic
dysvascular of traumatic cause for amputation:
younger
traumatic
dysvascular of traumatic cause for amputation:
more active
traumatic
dysvascular of traumatic cause for amputation:
faster return to activity
traumatic
dysvascular of traumatic cause for amputation:
may have no PMHx
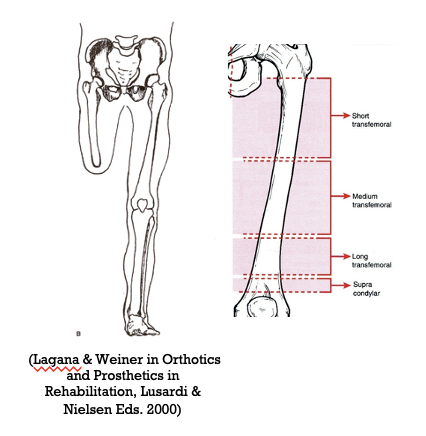
trans (ex. transtibial, transphalangeal)
the term “_________” is used when an amputation extends across the axis of a long bone
disarticulation (ex. Knee disarticulation, Toe disarticulation)
Amputations between long bones or through a joint is called a ____________
partial
the term “_________” is used when a part of the foot or hand distal to the ankle or wrist is amputated
residual limb or stump
the ____________ is the portion of the limb remaining after the amputation
stump
the residual limb is also called the __________
amputated
involved
prosthetic
what are the 3 terms used to describe the side of amputation
non-amputated
sound
uninvolved
intact
what are the 4 terms used to describe the side that is not amputated
fit and control of a prosthesis (bony anatomy, lever arm)
distal weight bearing
contractures
posture and balance (laying, sitting, standing)
gait mechanics and metabolic cost
what are the 5 things that the level of the amputation can affect
hemipelvectomy
_____________ is an amputation that involves removal of the entire leg (to include hip, buttock, and pelvic)
R
T/F: a hemipelvectomy is a common amputation
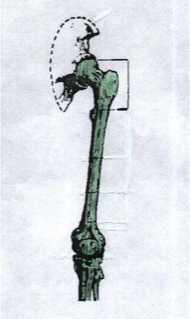
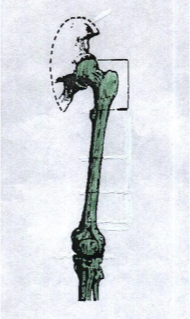
hip disarticulation
_____________ is an amputation that involves excision of the LE at the hip joint and the remaining musculature is closed over the acetabulum
trauma
vascular insufficiency
femoral sarcomas
what are some common causes for a hip disarticulation
F
T/F: a hip disarticulation is a common amputation
T
T/F: contractures are not an issue with a hemipelvectomy and hip disarticulation
hip disarticulation
stuff you would need to consider for a ______________ amputation:
limited bony anatomy for control of a prosthesis
lacks good weight bearing surface
laying, sitting and standing affected
T
T/F: crutches are less cumbersome for individuals with a hemipelvectomy and hip disarticulation
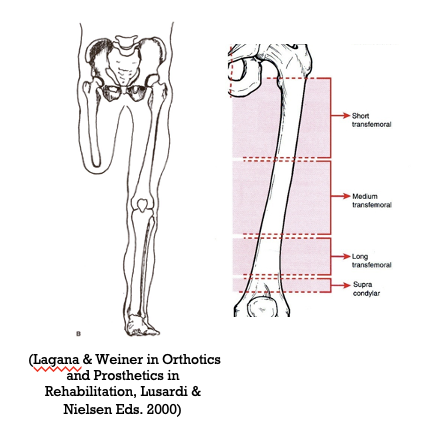
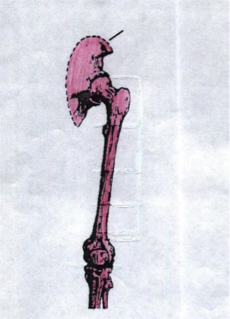
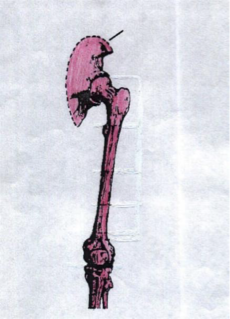
transfemoral amputation
_____________ is an amputation that is above the knee
dysvascular
trauma
what are some common causes for a transfemoral amputation
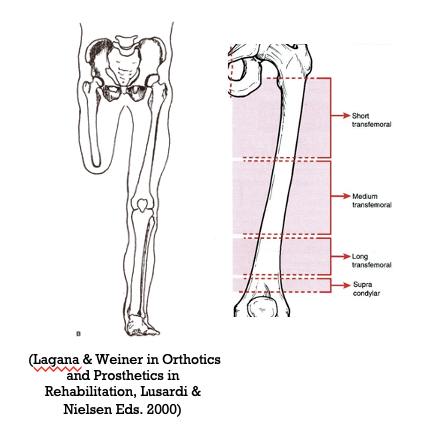
junction of middle and lower 1/3 femur
where is a transfemoral amputation typically performed at
25
a transfemoral amputation accounts for more than _____% of all LE amputation
hip flexion
hip abduction
hip ER
what muscles are at risk for contracture with a transfemoral amputation
tibial
the lever arm of a trans (femoral or tibial) amputation is better at control of the prosthesis
transfemoral
stuff you would need to consider for a ______________ amputation:
lever based on length of residuum and bony anatomy moderate for control of prosthesis
avoid distal end WB
sitting posture (socket) and standing balance affected
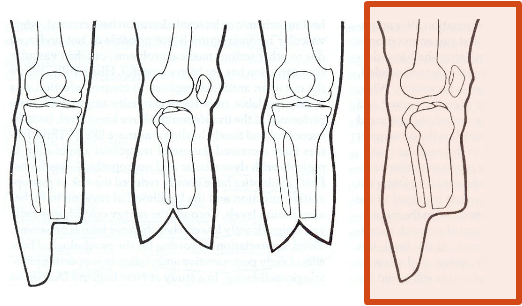
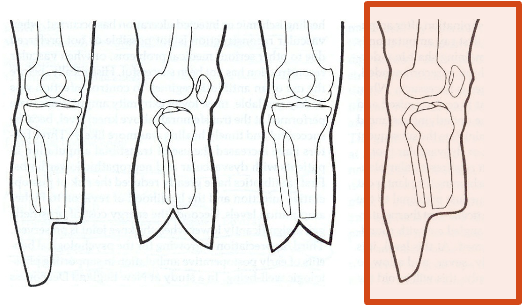
knee disarticulation
_______________ is an amputation that is through the knee joint
diabetes
PVD
trauma
what are some common causes for a knee disarticulation
Gritti-Strokes
a knee disarticulation is also called ______________
hip flexion
hip abduction
hip ER
what muscles are at risk for contracture with a knee disarticulation amputation
knee disarticulation
stuff you would need to consider for a ______________ amputation:
long anatomic lever provides power for ambulation and bony anatomy allows for better control
Bulbus end complicates prosthetic fitting and limits space for knee mechanism
broad, horizontal distal end tolerates WB
transfemoral
a knee disarticulation amputation has the same sitting, standing, and gait as a _____________ amputation
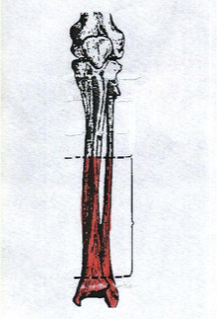
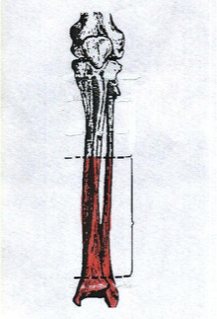
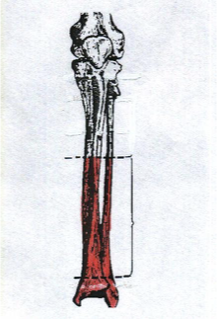
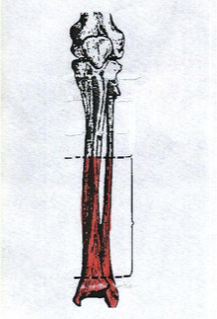
transtibial
a ______________ amputation is below the knee amputation
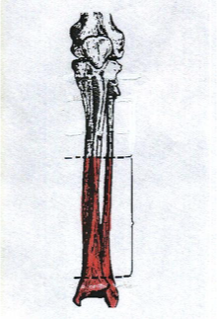
5-6 inches
the standard length of a transtibial amputation is about ____-____ of the tibia remaining from the tibial plateau
25
transtibial amputations account for _____% of LE amputations
diabetes
PVD trauma
what are some common causes for a transtibial amputation
transtibial
stuff you would need to consider for a ______________ amputation:
lever based on length of residuum and bony anatomy better for control of prosthesis
avoid WB on distal end
sitting can be affected by socket
knee flexion
what muscles are at risk for contracture with a transtibial amputation

ankle (symes) disarticulation
a _____________ amputation is at the talocrural joint with removal of the inferior projections of the tibia and fibula

T (it attaches to the distal tibia)
T/F: the heel fat pad is preserved with an ankle disarticulation amputation

50
ankle (symes) disarticulation accounts for ________% of LE amputations

diabetes
PVD
traumatic
what are some common causes for an ankle disarticulation

ankle (symes) disarticulation
stuff you would need to consider for a ______________ amputation:
long lever arm of the tibia creates good control of protesis
bulbus end complicates prosthetic fitting and limits space for foot mechanism
ambulation for short distances without prosthesis
transtibial
an ankle (symes) disarticulation amputation will have the same gait as a _____________ amputation
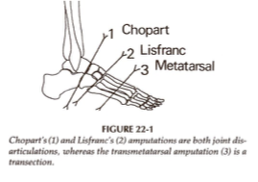
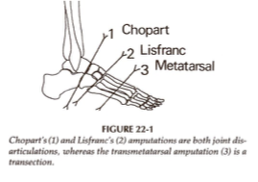
chopart
___________ is a partial foot amputation where there is disarticulation of the midtarsal joint
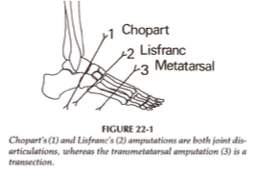
calcaneus; talus
a chopart amputation preserves the _____________ and ____________ bones
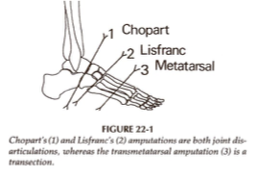
lisfranc
___________ is a partial foot amputation where there is disarticulation of the tarsometatarsal joint
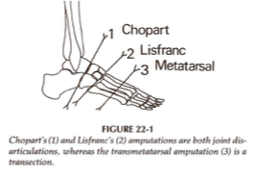
transmetatarsal
___________ is a partial foot amputation that is performed through mid-/proximal MT shaft
dysvascularity
_______________ is the cause of all partial foot amputations

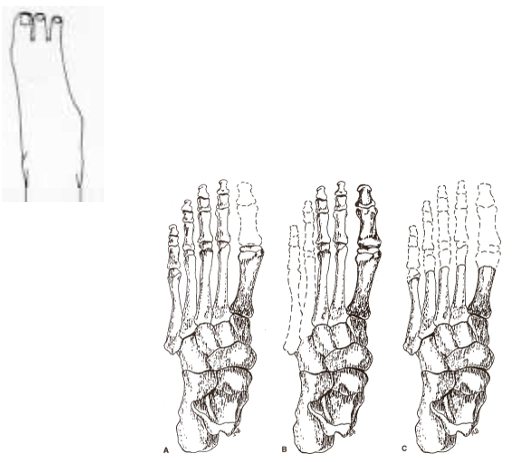
ray
a ___________ amputation is a longitudinal amputation of one or more metatarsals or toes
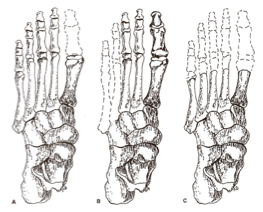
transphalangeal
a ______________ amputation involves the amputation/disarticulation of one or more toes
Dysvascularity or trauma (including frostbite, gangrene, infection)
the cause for both a ray or transphalangeal amputation is either ____________ or _______________
partial foot, ray, and transphalangeal
stuff you would need to consider for a ______________ amputation:
increase risk for tissue breakdown (limited soft tissue envelope)
Can WB on remaining portion of the foot
Risk for remaining foot drawn into equinovarus

loss of great toe lever
the primary impact on gait for a partial foot, ray, and transphalangeal amputation is _____________
equinovarus
_______________ is a common congenital deformity where a baby’s foot is twisted inward and downward due to short, tight ligaments and tendons
T
T/F: a prosthesis is typically not prescribed for a partial foot, ray, and transphalangeal amputation

guillotine
the _____________ surgical approach for an amputation involves all tissues being divided at the same level

guillotine
indications for the _______________ surgical approach for an amputation:
an infection
when all dead tissue has not been removed

equal
a fish mouth amputation technique is when the skin flaps are (equal or unequal)
unequal
a flap amputation technique is when the skin flaps are (equal or unequal)
frontal; sagittal
both the fish mouth and flap amputation techniques orient the incision at the distal end in either _________ or _________ plane
posterior; because the thick gastroc and soleus will cover the residual limb and the incision goes on the anterior end away from pressure/WB
a ______________ flab amputation approach is most common in the LE, why?
transfemoral
transtibial
the sciatic nerve is cut and permitted to retract proximally to prevent formation of a neuroma in what types of amputations?
symes (ankle disarticulation)
the anterior and posterior nerves are cut and permitted to retract proximally to prevent formation of a neuroma in what types of amputations?
5cm
tissue and muscle are separated from the bone at least ________ proximal to the incision line (TF: femur; TT: tibia)
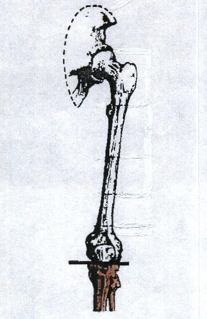
myodesis
______________ is soft tissue management that anchors muscle to bone
myoplasty
______________ is soft tissue management where the muscle is looped around the end and sewen to each other
tendosis
______________ is soft tissue management that attaches the tendons to bone

agonist-antagonist myoneural interface (AMI)
___________________ is an experimental soft tissue management where the muscles are linked together so that control and proprioception feedback (via EMG recording) can be used to control a prosthesis
osseointegration (OI)
__________________ is an internal prosthetic implant (“abutment”) that protrudes through soft tissue and skin to external components
bone
an osseointegration (OI) is anchored by ___________
osseointegration (OI)
_____________ is an option when a traditional socket is NOT tolerated
transtibial (TT)
the Ertl procedure is a modification of the ___________ procedure
Ertl
the _____________ procedure installs a bone as a “bridge” between the fibula and tibia to allow for distal end WB
length (viable tissue)
the goal for prosthetic surgery is to preserve as much ___________ as possible
Lever for stabilization
Total surface for distribution on forces and for thermoregulation
Proprioceptive feedback
Phantom pain and sensation
Energy requirements for ambulation
the benefits for preserving as much length as possible (5)