HUNT245
0.0(0)
Card Sorting
1/222
There's no tags or description
Looks like no tags are added yet.
Last updated 11:29 PM on 5/29/23
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
223 Terms
1
New cards
Euhydration
refers to a normal state of body water, ith deviations from this norm producing compensatory responses
2
New cards
Hyperhydration
too much water
a sustained increase in body water, although often transient
a sustained increase in body water, although often transient
3
New cards
hypohydration
too little water (hypo=low)
a sustained decrease in body water
a sustained decrease in body water
4
New cards
Dehydration
refers to the process of losing water, rather than a state of low body water
5
New cards
water balance
losses
* faecal
* respiratory
* urine
* sweat
\
Gains
* metabolic water production
* food
* drink
* faecal
* respiratory
* urine
* sweat
\
Gains
* metabolic water production
* food
* drink
6
New cards
measures of pre exercise hydration
* urine osmolality
* urine specific gravity
* urine colour
* serum osmolality
* urine specific gravity
* urine colour
* serum osmolality
7
New cards
pre-exercise guidelines
* start exercise in a euhydrated state
* slowly drink 5-7ml/kg at least 4 hours prior to exercise
* if urine still dark drink further 3-5ml/kg 2 hours prior
* slowly drink 5-7ml/kg at least 4 hours prior to exercise
* if urine still dark drink further 3-5ml/kg 2 hours prior
8
New cards
effects of dehydration
* depends on the event
* decrease in skill performance
* decrease in mental performance
* opening of the blood brain barrier
* increased perception of effort
* decrease in skill performance
* decrease in mental performance
* opening of the blood brain barrier
* increased perception of effort
9
New cards
ACSM drink guidelines
* try to limit dehydration to
10
New cards
effects of overhydration
* increase in body mass
* urination
* dilution of blood sodium
* hyponatremia
* urination
* dilution of blood sodium
* hyponatremia
11
New cards
hyponatremia
* blood sodium concentrate
12
New cards
Risk factors of hyponatremia?
* exercise duration >4hrs
* slow speeds
* females
* low body weight
* excessive fluid intakes
* non-steroidal anti-inflammatories
* extreme environments
* slow speeds
* females
* low body weight
* excessive fluid intakes
* non-steroidal anti-inflammatories
* extreme environments
13
New cards
Pathogenesis
* Excessive water intake
* other etiologies
* hormonal abnormalities
* renal abnormalities
* mobilization of sodium stores
* other etiologies
* hormonal abnormalities
* renal abnormalities
* mobilization of sodium stores
14
New cards
aim of sodium DURING exercise
Assisting with maintenance of
* total body water
* plasma volume
* plasma sodium concentration
* total body water
* plasma volume
* plasma sodium concentration
15
New cards
recovery guidelines (hydration)
* prepare for the next training session
* exercise
* exercise
16
New cards
carbohydrate digestion
mouth
* salivary a-amylase hydrolyses dietary starch
Stomach
* the acidity of the stomach temporarily inhibits a-amylase and stops carbohydrate digestion
small intestine
* bicarbonate secretion from the pancreas neutralizes the stomach contents and pancreatic a-amylase continues to digest starch
* several disaccharidase enzymes breakdown disaccharides in the brush border of the small intestine producing monosaccharides (glucose, fructose, etc)
\
* salivary a-amylase hydrolyses dietary starch
Stomach
* the acidity of the stomach temporarily inhibits a-amylase and stops carbohydrate digestion
small intestine
* bicarbonate secretion from the pancreas neutralizes the stomach contents and pancreatic a-amylase continues to digest starch
* several disaccharidase enzymes breakdown disaccharides in the brush border of the small intestine producing monosaccharides (glucose, fructose, etc)
\
17
New cards
intestinal carbohydrate absorption
small intestine
* glucose is absorbed in the small intestine via a sodium glucose transporter (SGLT-1)
* fructose is absorbed via a different transporter, GLUT5
* GLU and FRU are transported across the basolateral membrane via the transporter GLUT-2
* GLU and FRU are transported to the liver where fructose is removed from the circulation
* glucose is absorbed in the small intestine via a sodium glucose transporter (SGLT-1)
* fructose is absorbed via a different transporter, GLUT5
* GLU and FRU are transported across the basolateral membrane via the transporter GLUT-2
* GLU and FRU are transported to the liver where fructose is removed from the circulation
18
New cards
Glycogenesis
1. CHO ingestion stimulates the release of insulin from the pancreas
2. insulin stimulates GLUT-4 translocation to muscle membrane
3. glucose-6-phosphate stimulates the production of glycogen
19
New cards
Daily needs (carbohydrate)
* fuel for the muscle and brain during exercise
* low levels of carbohydrate stores are a factor in fatigue and reduced performance
* ensuring that stores are increased result in performance enhancements
* low levels of carbohydrate stores are a factor in fatigue and reduced performance
* ensuring that stores are increased result in performance enhancements
20
New cards
factors causing suboptimal intakes (general)
* restricted energy intake
* inadequate practical nutrition skills
* food culture
* poor availability of carbohydrate rich foods
* GI discomfort
* fad diets
* Chaotic lifestyle/travel
* inadequate practical nutrition skills
* food culture
* poor availability of carbohydrate rich foods
* GI discomfort
* fad diets
* Chaotic lifestyle/travel
21
New cards
factors causing suboptimal intakes (assessment techniques)
* recording errors
* altered intake during recording
* inaccurate recording
* errors in quantification
* altered intake during recording
* inaccurate recording
* errors in quantification
22
New cards
pre-event meal - considerations
* time of day the event takes place
* length of the event
* climatic conditions
* at home or away from home
* domestic or overseas
* past experience
* length of the event
* climatic conditions
* at home or away from home
* domestic or overseas
* past experience
23
New cards
during exercise - mechanisms of action
* sparing of skeletal muscle glycogen
* prevention of liver glycogen depletion
* prevention of hypoglycemia
* allow high rates of carbohydrate oxidation
* prevention of liver glycogen depletion
* prevention of hypoglycemia
* allow high rates of carbohydrate oxidation
24
New cards
during exercise considerations
* start early to preserve glycogen depletion
* consider fluid replenishment too, again start early to avoid excess dehydration
* for both may want small amounts spread across the session to avoid GI distress
* think logistics how easily can it be accessed?
* if fluid what temp may be best
* practice all fluid and food strats in training to avoid impaired race performance
* consider fluid replenishment too, again start early to avoid excess dehydration
* for both may want small amounts spread across the session to avoid GI distress
* think logistics how easily can it be accessed?
* if fluid what temp may be best
* practice all fluid and food strats in training to avoid impaired race performance
25
New cards
after exercise considerations (carbs)
* time to next exercise session
* intensity of session just completed
* what’s the overall nutrition strat
* demands of the next training session
* tolerance of gut (+ appetite)
* logistics
* intensity of session just completed
* what’s the overall nutrition strat
* demands of the next training session
* tolerance of gut (+ appetite)
* logistics
26
New cards
amino acid structure - AA composition
AA contain carbon, hydrogen and oxygen (as do CHO and fat) but AA also contain nitrogen
27
New cards
amino acid structure - AA structure
1. Carboxyl group
2. amine group
3. variable group (side chain)
each AA’s has a different side chain
\
28
New cards
Dipeptide
Composed of 2 AA that are joined by a chemical bond, known as a peptide bond
29
New cards
Polypeptide
Longer chains of AA are known as polypeptides (>20 AA)
30
New cards
Proteins
* proteins consist of many polypeptide chains
* __primary structure__ - determined by the AA sequence
* __secondary structure__ - determined by the interactions between groups (short)
* __tertiary structure -__ determined by interactions between side chains (3D)
* __primary structure__ - determined by the AA sequence
* __secondary structure__ - determined by the interactions between groups (short)
* __tertiary structure -__ determined by interactions between side chains (3D)
31
New cards
Protein Digestion
Stomach
* hydrochloric acid denatures the proteins and pepsin degrades proteins to large polypeptides and AA
Pancreas
* pancreatic enzymes include trypsin and chylotrypsin degrade polypeptides to oligopeptides and AA
Small intestine
* aminopeptidase degrade oligopeptides to peptides and AA
* AA and small peptides are hydrolysed in the cytosol and thus AA enter the circulation
* hydrochloric acid denatures the proteins and pepsin degrades proteins to large polypeptides and AA
Pancreas
* pancreatic enzymes include trypsin and chylotrypsin degrade polypeptides to oligopeptides and AA
Small intestine
* aminopeptidase degrade oligopeptides to peptides and AA
* AA and small peptides are hydrolysed in the cytosol and thus AA enter the circulation
32
New cards
Amino acid metabolism summary
* we cannot store excess AA within the body
* the AA in the blood and ECF represent the AA pool (170g)
* proteins are degraded and synthesized
* this AA pool is constantly turning over (contributes\~20% to BMR)
* AA from the diet can enter this pool as can AA released from liver and muscle
* AA can also be extracted by liver and muscle
* the liver plays a critical role in regulating the composition of the AA pool
* the AA in the blood and ECF represent the AA pool (170g)
* proteins are degraded and synthesized
* this AA pool is constantly turning over (contributes\~20% to BMR)
* AA from the diet can enter this pool as can AA released from liver and muscle
* AA can also be extracted by liver and muscle
* the liver plays a critical role in regulating the composition of the AA pool
33
New cards
Protein Quality
Complete Proteins
* all EAA present
Incomplete Proteins
* plant proteins are deficient in one EAA (lysine, tryptophan, methionine)
Vegetarians
* digestibility
* cell walls of plant proteins (inhibit digestion)
* anti-nutritional factors (inhibit digestion)
* all EAA present
Incomplete Proteins
* plant proteins are deficient in one EAA (lysine, tryptophan, methionine)
Vegetarians
* digestibility
* cell walls of plant proteins (inhibit digestion)
* anti-nutritional factors (inhibit digestion)
34
New cards
Leucine (BCAA)
essential AA
the trigger AA for muscle protein synthesis
the trigger AA for muscle protein synthesis
35
New cards
what is an essential amino acid
we have to have it in our diets bc we cannot synthesize them from the breakdown of other amino acids in the body
36
New cards
what is a supplement?
A food, food component, nutrient, or non-food compound that is purposefully ingested in addition to the habitually consumed diet with the aim of achieving a specific health and/or performance benefit.
37
New cards
overseas contamination research (supplements)
10-20% of supplements contaminated
38
New cards
supplement testing companies process
Stage 1 - manufacturing critical control audit
stage 2 - ongoing testing (every batch plus additional blind sampling)
Stage 3 - use of logo
stage 2 - ongoing testing (every batch plus additional blind sampling)
Stage 3 - use of logo
39
New cards
if chose supplements need to minimise risk
* “assess the need, assess the risk”
* choose a product with proven efficacy
* ensure product is made to high quality standards
* ensure product has been tested for banned contaminants by a recognized sports anti-doping lab
* choose a product with proven efficacy
* ensure product is made to high quality standards
* ensure product has been tested for banned contaminants by a recognized sports anti-doping lab
40
New cards
potential reasons for supplement use
* some nutrients are difficult to obtain from food without excessive intakes
* some essential nutrients are only available in foods some athletes won’t eat
* its difficult to determine the exact amounts of some nutrients in food
* food sources maybe difficult to consume close to, during or after exercise
* some nutrients maybe required in high doses to improve health
* some essential nutrients are only available in foods some athletes won’t eat
* its difficult to determine the exact amounts of some nutrients in food
* food sources maybe difficult to consume close to, during or after exercise
* some nutrients maybe required in high doses to improve health
41
New cards
creatine
* creatine is a molecule that is produced in the body from amino acids
* creatine stores high-energy phosphate groups in the form of phosphocreatine
* these phosphate groups are donated to ADP to regenerate it to ATP
* creatine is found in some animal-based foods and is most prevalent in meat and fish
* creatine stores high-energy phosphate groups in the form of phosphocreatine
* these phosphate groups are donated to ADP to regenerate it to ATP
* creatine is found in some animal-based foods and is most prevalent in meat and fish
42
New cards
how do we get energy from food to power muscle contractions
* food digested
* absorbed in the small intestine
* nutrient travel to cell
* nutrients utilized to create ATP
* ATP = energy currency of the body
* ATP broken down to ADP releasing energy
* Need nutrients to resynthesize ATP
* different exercise results in different pathways for ATP resynthesis
* absorbed in the small intestine
* nutrient travel to cell
* nutrients utilized to create ATP
* ATP = energy currency of the body
* ATP broken down to ADP releasing energy
* Need nutrients to resynthesize ATP
* different exercise results in different pathways for ATP resynthesis
43
New cards
ATP resynthesis pathways
pathway for ATP resynthesis depends on intensity
high-intensity exercise can result in up to a 1000-fold increase in the rate of ATP demand compared to that at rest
\
Resynthesis:
break down is stored in chemical containing a high-energy phosphate bond so that the energy released by its breakdown can be used to reconstitute ATP from ADP and Pi:
PCr (creatine) decomposes to creatine plus a phosphate ion plus energy
high-intensity exercise can result in up to a 1000-fold increase in the rate of ATP demand compared to that at rest
\
Resynthesis:
break down is stored in chemical containing a high-energy phosphate bond so that the energy released by its breakdown can be used to reconstitute ATP from ADP and Pi:
PCr (creatine) decomposes to creatine plus a phosphate ion plus energy
44
New cards
Australia institute of sport
* the A, B, C, D classification system focuses on sports foods and individual ingredients rather than specific supplement products and brands
* a = strong evidence
* B = emerging evidence: needs more research to be used under monitoring or research protocols
* c = no supportive evidence
* D = banned/high risk
* a = strong evidence
* B = emerging evidence: needs more research to be used under monitoring or research protocols
* c = no supportive evidence
* D = banned/high risk
45
New cards
electrolyte balance (hydration)
* major electrolyte lost in sweat is sodium
* 20-80 mmol/l (460-1840 mg/L)
* sweat potassium concentrates \~2-8 mmol/L
* 20-80 mmol/l (460-1840 mg/L)
* sweat potassium concentrates \~2-8 mmol/L
46
New cards
Why include sodium (hydration)
Generally included to
* major electrolyte lost in sweat
* improves palatability
* maintains extracellular volume
* may attenuate the decline in blood sodium
* major electrolyte lost in sweat
* improves palatability
* maintains extracellular volume
* may attenuate the decline in blood sodium
47
New cards
palatability
* increasing palatability could increase fluid intake thereby delaying the onset of dehydration
* BUT large amounts of salt decrease palatability
* fluid intakes greatest with 30mmol/L NaCl solution
* BUT large amounts of salt decrease palatability
* fluid intakes greatest with 30mmol/L NaCl solution
48
New cards
sodium and thirst
* sodium ingestion may promote fluid intake via increasing thirst
* delay dehydration
* delay dehydration
49
New cards
Gastric emptying / intestinal absorption
* sodium is important for intestinal absorption
* however, the inclusion of sodium in a drink does not effect gastric emptying or intestinal absorption
* however, the inclusion of sodium in a drink does not effect gastric emptying or intestinal absorption
50
New cards
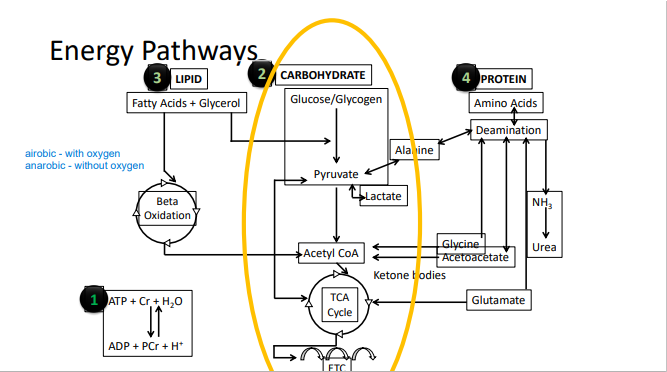
Energy pathways
51
New cards
Anaerobic Glycolysis
carbohydrate broken down to release energy to phosphorylate ADP and form ATP
Final product = Lactate and H+
\
glycogen - stored form in our muscles and in the liver
can produce 3ATP if it is from glycogen and only two ATP from glycose
Final product = Lactate and H+
\
glycogen - stored form in our muscles and in the liver
can produce 3ATP if it is from glycogen and only two ATP from glycose
52
New cards
Aerobic vs Anaerobic
aerobic = with oxygen
anaerobic = without oxygen
anaerobic = without oxygen
53
New cards
Aerobic metabolism
Oxidative phosphorylation - carbohydrate, protein, fat
Continuous supply of ATP as long as O2 is available
Occurs: Mitochondria
3 Phases:
1. preparation
2. Krebs cycle / Tricarboxylic acid (TCA) cycle - oxidises, removes, electrons
3. Electron transport chain (ETC) - electrons undergo a number of reactions releasing energy to rephosphorylate ADP to ATP
30-32 ATP
Continuous supply of ATP as long as O2 is available
Occurs: Mitochondria
3 Phases:
1. preparation
2. Krebs cycle / Tricarboxylic acid (TCA) cycle - oxidises, removes, electrons
3. Electron transport chain (ETC) - electrons undergo a number of reactions releasing energy to rephosphorylate ADP to ATP
30-32 ATP
54
New cards
Energy metabolism
mainly from plasma glycose and muscle glycogen
* when we are at rest over half (2/3) of our energy comes from fat and a tiny bit from carbs - when we exercise it comes mainly from carbs
* carbs are really important for high intensity or high level sports
* we cant just convert our lipid and fat stores fast enough so we have to rely on carbs
* ever at 75% we do have a little bit of lipids used by majority of the energy is coming from carbs
* when we are at rest over half (2/3) of our energy comes from fat and a tiny bit from carbs - when we exercise it comes mainly from carbs
* carbs are really important for high intensity or high level sports
* we cant just convert our lipid and fat stores fast enough so we have to rely on carbs
* ever at 75% we do have a little bit of lipids used by majority of the energy is coming from carbs
55
New cards
What happens when insufficient CHO ingested - Dietary CHO and Training
* progressive decrease in muscle glycogen with low carb diet
* glycogen content of muscles can be manipulated by dietary intakes
* glycogen content of the working muscle is a determinant for their capacity to perform heavy exercise
* glycogen content of muscles can be manipulated by dietary intakes
* glycogen content of the working muscle is a determinant for their capacity to perform heavy exercise
56
New cards
Gastrointestinal distress (carbs)
Gastrointestinal problems occur frequently, especially in long-distance races
* problems seem to be highly individual and perhaps genetically determined
May also be related to the intake of
* highly concentrated carb solutions (gels without water)
* hyperosmotic drinks
* the intake of fibre, fat and protein
* problems seem to be highly individual and perhaps genetically determined
May also be related to the intake of
* highly concentrated carb solutions (gels without water)
* hyperosmotic drinks
* the intake of fibre, fat and protein
57
New cards
Carbohydrate loading
* super-compensated muscle glycogen levels, improve performance 2-3%
* no need for the depletion phase prior to loading
* requirements can vary from around 8 to 12 g-kg-1-day-1 depending on the athlete and their activity
* glycogen storage is associated with weight gain as a result of water retention (approx 3g per gram of glycogen)
* no need for the depletion phase prior to loading
* requirements can vary from around 8 to 12 g-kg-1-day-1 depending on the athlete and their activity
* glycogen storage is associated with weight gain as a result of water retention (approx 3g per gram of glycogen)
58
New cards
Mechanisms of Action - during exercise (carbs)
* sparing of skeletal muscle glycogen
* prevention of liver glycogen depletion
* prevention of hypoglycemia
* allow high rates of carbohydrate oxidation
* prevention of liver glycogen depletion
* prevention of hypoglycemia
* allow high rates of carbohydrate oxidation
59
New cards
muscle protein synthesis (MPS)
* varies between different dietary protein sources, depends on post-prandial rise in plasma essential amino acid concentrations (esp leucine)
* Leucine is sensed by sestrin2, which promotes translocation of mammalian target of rapamycin complex 1 (mTORC1) to the lysosome membrane where it becomes activated, resulting in the activation of the downstream anabolic signaling pathways that control muscle tissue protein synthesis
* Plasma amino acid concentrations also provide the necessary precursors for protein synthesis rates to increase
* Ingesting 20–25 g whey protein (providing 2.2–2.7 g leucine) strongly increases muscle protein synthesis rate
* Leucine is sensed by sestrin2, which promotes translocation of mammalian target of rapamycin complex 1 (mTORC1) to the lysosome membrane where it becomes activated, resulting in the activation of the downstream anabolic signaling pathways that control muscle tissue protein synthesis
* Plasma amino acid concentrations also provide the necessary precursors for protein synthesis rates to increase
* Ingesting 20–25 g whey protein (providing 2.2–2.7 g leucine) strongly increases muscle protein synthesis rate
60
New cards
absorption of protein
* plant-based whole foods have a lower absorbability when compared with animal-based whole foods
* \~ 85-95% of the protein in egg whites, whole eggs, and chicken is absorbed
* \~ 50-75% of the protein in chickpeas, mung beans and yellow peas in absorbed
why?
* anti-nutritional factors in plant-based protein sources, e.g. fibre and polyphenolic tannins attenuate absorption
\
summary
* Animal protein = higher protein quality, is usually considered to be superior to plant protein for building muscle mass
* Healthcare professionals encourage the replacement of animal protein, particularly red meat, with plant protein to help decrease the risk of cardiovascular diseases.
* Plant protein also reduces harm to the environment by decreasing the demand for animal protein, animal farming tends to be more resource intensive with higher greenhouse gas emissions
* \~ 85-95% of the protein in egg whites, whole eggs, and chicken is absorbed
* \~ 50-75% of the protein in chickpeas, mung beans and yellow peas in absorbed
why?
* anti-nutritional factors in plant-based protein sources, e.g. fibre and polyphenolic tannins attenuate absorption
\
summary
* Animal protein = higher protein quality, is usually considered to be superior to plant protein for building muscle mass
* Healthcare professionals encourage the replacement of animal protein, particularly red meat, with plant protein to help decrease the risk of cardiovascular diseases.
* Plant protein also reduces harm to the environment by decreasing the demand for animal protein, animal farming tends to be more resource intensive with higher greenhouse gas emissions
61
New cards
recovery summary (protein)
The timing and composition of the post-competition or post-exercise meal or snack depend on the level of athlete, length and intensity of the exercise session, and when the next intense workout will occur.
* Eating a source of high quality protein soon after exercise will promote muscle protein synthesis.
* High quality protein particularly from food sources will provide multiple nutrients
* It may help to choose a protein source that is rapidly digested, i.e. whey protein (from foods and drinks).
* Protein powders or liquid meal replacements can be suitable for convenient options
* Eating a source of high quality protein soon after exercise will promote muscle protein synthesis.
* High quality protein particularly from food sources will provide multiple nutrients
* It may help to choose a protein source that is rapidly digested, i.e. whey protein (from foods and drinks).
* Protein powders or liquid meal replacements can be suitable for convenient options
62
New cards
RED-S
relative energy deficiency in sport
63
New cards
what is an eating disorder
* Clinically diagnosable conditions (American Psychiatric Association DSM-V, 2013)
* Eating disorders are illnesses
* Severe disturbances in their eating behaviors and related thoughts and emotions. People with eating disorders typically become pre-occupied with food and their body weight.
* Anorexia nervosa, bulimia nervosa, binge eating etc
* Eating disorders are illnesses
* Severe disturbances in their eating behaviors and related thoughts and emotions. People with eating disorders typically become pre-occupied with food and their body weight.
* Anorexia nervosa, bulimia nervosa, binge eating etc
64
New cards
eating disorder amongst athletes
Varies by sport higher in
* weight classes (such as rowing), aesthetic sports (such as gymnastics or figure skating)
* sports where having a low body mass is seen as advantageous (such as cross-country or cycling).
* Rates = 25% to 42%,
* Other sports (team sports) 12% to 17%
* weight classes (such as rowing), aesthetic sports (such as gymnastics or figure skating)
* sports where having a low body mass is seen as advantageous (such as cross-country or cycling).
* Rates = 25% to 42%,
* Other sports (team sports) 12% to 17%
65
New cards
Common Comorbidities (eating disorders)
individuals affected by eating disorders commonly suffer from other mental health conditions
* depression
* anxiety
* ODC
* and substance use disorder
* depression
* anxiety
* ODC
* and substance use disorder
66
New cards
health consequences of eating disorders
* one of the highest mortality rates of any mental health condition
* death is most often caused by suicide or cardiac arrhythmia - suicide accounts for 20% of deaths among patients with anorexia nervosa and 23% of deaths among patients with bulimia nervosa
* death is most often caused by suicide or cardiac arrhythmia - suicide accounts for 20% of deaths among patients with anorexia nervosa and 23% of deaths among patients with bulimia nervosa
67
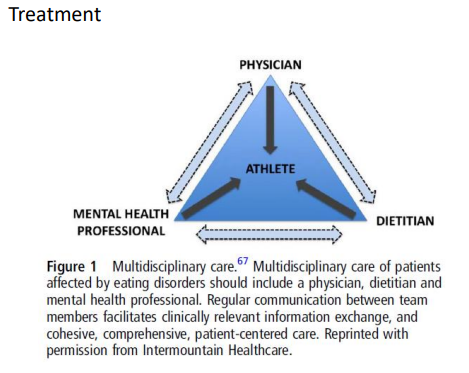
New cards
treatment for eating disorders
68
New cards
RED-S timeline
1960s
* delayed menarche in undernourished rural girls
* Guula Erdelyi observed changes in menstrual patterns during sport
1970s
* delayed menarche in some athletes
* title IX of the education amendments of 1972
1980s
* first female athlete triad position statement published
* link between amenorrhea and bone mineral density
* links between training volume and thyroid hormones
* delayed menarche in undernourished rural girls
* Guula Erdelyi observed changes in menstrual patterns during sport
1970s
* delayed menarche in some athletes
* title IX of the education amendments of 1972
1980s
* first female athlete triad position statement published
* link between amenorrhea and bone mineral density
* links between training volume and thyroid hormones
69
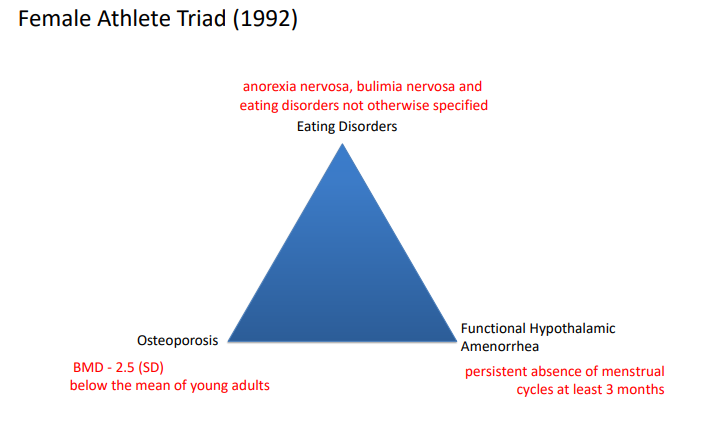
New cards
Female athlete triad (1992)
disordered eating, functional hypothalamic amenorrhea (persistent absence of menstrual cycles at least 3 months), osteoporosis BMD (2.5 SD)
70
New cards
Energy availability
amount of energy available following the energy used for exercise for normal physiological functions per kg of fat free mass
* anything 30 kcal/kg FFM/d is an energy deficiency
* anything 30 kcal/kg FFM/d is an energy deficiency
71
New cards
Low energy Availability (LEA)
Mismatch between an athlete’s energy intake (diet) and energy expended in exercise, leaving inadequate energy to support the functions required by the body to maintain optimal health and performance.
72
New cards
What happens with LEA → RED-S
* there is insufficient energy available for normal physiological functioning
* the body starts to act as if it were in a state of starvation
* non-essential processes are slowed or halted
* the body starts to act as if it were in a state of starvation
* non-essential processes are slowed or halted
73
New cards
symptoms of relative energy deficiency in females
* impaired menstrual cycle
* impaired immune system
* impaired bone density
* reduced female hormones
* impaired immune system
* impaired bone density
* reduced female hormones
74
New cards
Relative energy deficiency in male athletes
* decrease in hormone levels
* decrease in protein synthesis - response to resistance training
* direct impact on bone metabolism
* decrease in protein synthesis - response to resistance training
* direct impact on bone metabolism
75
New cards
Prevalence of LEA/RED-S , NZ survey
* 109 female recreational athletes
* mean age 23.8 years
* 45% at risk for LEA
* every added hour of exercise per week >1.3x risk
* mean age 23.8 years
* 45% at risk for LEA
* every added hour of exercise per week >1.3x risk
76
New cards
Prevalence of LEA/RED-S
* Oligomenorrhea/amenorrhea had been diagnosed in only 12% of athletes
* 50% of athletes not on hormonal contraception who reported symptoms consistent with this diagnosis
* Irregular periods were associated with history of stress fracture
* 73% felt elite sport participation was associated with pressure to have a specific physical appearance, that may be damaging to their overall health
* Barriers to communicating female health issues included male coaches and support staff, and lack of quality health education information.
* 50% of athletes not on hormonal contraception who reported symptoms consistent with this diagnosis
* Irregular periods were associated with history of stress fracture
* 73% felt elite sport participation was associated with pressure to have a specific physical appearance, that may be damaging to their overall health
* Barriers to communicating female health issues included male coaches and support staff, and lack of quality health education information.
77
New cards
Reasons for LEA/RED-S (intentional or unintentional)
* clinical eating disorder
* disordered eating
* inadvertent undereating
* intentional weight loss without disordered eating
* disordered eating
* inadvertent undereating
* intentional weight loss without disordered eating
78
New cards
threats to athletes energy intakes
* complete confusion
* diet gurus (nutrient demonization)
* Quick fixes and pyramid marketing
* diet gurus (nutrient demonization)
* Quick fixes and pyramid marketing
79
New cards
Orthorexia
an obsession with healthy eating
80
New cards
Why measure body composition
* identify physical characteristics of elite performers
* assess and monitor growth
* monitor training programs/dietary interventions
* determine optimal BC for weight category sports
* monitor the relationship for health and performance
* assess and monitor growth
* monitor training programs/dietary interventions
* determine optimal BC for weight category sports
* monitor the relationship for health and performance
81
New cards
Solutions/considerations for LEA/RED-S
* be aware of vulnerable athletes and have coaches on board and be clear on metrics reported
* focus on performance
* treat data confidentially
* longitudinal monitoring for at risk athletes
* de-emphasise the importance of body composition
* educate on body composition methods and metrics
* let senior athletes with good habits be role models
* focus on performance
* treat data confidentially
* longitudinal monitoring for at risk athletes
* de-emphasise the importance of body composition
* educate on body composition methods and metrics
* let senior athletes with good habits be role models
82
New cards
Recovery of Bone mineral density
Process: years
outcomes:
* increased estrogen continues to inhibit bone resorption
* increased energy status will stimulate anabolic hormones (IGF-1) and bone formation
outcomes:
* increased estrogen continues to inhibit bone resorption
* increased energy status will stimulate anabolic hormones (IGF-1) and bone formation
83
New cards
Recovery of menstrual status
Process: months
Outcomes:
* increased reproductive hormones
* increased estrogen exerts and anti-resorptive effect on bone
Outcomes:
* increased reproductive hormones
* increased estrogen exerts and anti-resorptive effect on bone
84
New cards
Recovery of Energy status
Process: days or weeks
Outcomes:
* increased energy status will stimulate anabolic hormones (IGF-1) and bone formation
* increased energy status will reverse energy conservation adaptations
Outcomes:
* increased energy status will stimulate anabolic hormones (IGF-1) and bone formation
* increased energy status will reverse energy conservation adaptations
85
New cards
Advice for clients who may be at risk for RED-S
1. ensure you fuel well around training: cereal, sandwich or porridge before training and sandwiches, pasta and veggies after training are ideal
2. if you are hungry eat
3. Regularly eating throughout the day should help reduce hunger, and also keep you adequately fueled
4. Take at least one rest/recovery day a week
86
New cards
Why do a dietary assessment?
* Nutrition assessment is the basis for a nutritional diagnosis and evaluation
* identify nutritional related problems and their probable causes
* the foundation for nutritional strategies and interventions
* evaluate short and long term health and disease risk
Assessment is not only what someone eats and drinks it may also be
* social, medical and psychological influences on food choices
* may also get energy expenditure data -training and competition
* anthropometrical data (body composition)
* biochemical data
* identify nutritional related problems and their probable causes
* the foundation for nutritional strategies and interventions
* evaluate short and long term health and disease risk
Assessment is not only what someone eats and drinks it may also be
* social, medical and psychological influences on food choices
* may also get energy expenditure data -training and competition
* anthropometrical data (body composition)
* biochemical data
87
New cards
What are you trying to capture? why are you doing it?
* do you need to further communicate with health professionals
* are you going to then create a plan or more information for them?
* when you see them next, summary of what you previously went over with them
* write complete notes for your situation to avoid double handling
* are you going to then create a plan or more information for them?
* when you see them next, summary of what you previously went over with them
* write complete notes for your situation to avoid double handling
88
New cards
Different type of clients? - Under reporter
* wants to lose weight
* everything sounds like its going great
* how can this be happening?
Ask Questions like
* what happens on a bad day
* what does a typical day look like
* what happens when things go wrong
* everything sounds like its going great
* how can this be happening?
Ask Questions like
* what happens on a bad day
* what does a typical day look like
* what happens when things go wrong
89
New cards
Different type of clients? - Over-reporter
* usually more associated with low energy / disordered eating
* expect it to be over-reported
* intake will sound good but ideally have some form of images to back up portions
\
* expect it to be over-reported
* intake will sound good but ideally have some form of images to back up portions
\
90
New cards
Different type of clients? - the informed/heavily influenced
* clean rater, paleo, vegan etc. May want performance nutrition or potentially weight loss
* may have some meals in a certain way but may still indulge in high calorie foods
* may have poor recovery nutrition
* interested in nutrition - highly motivated
* may have some meals in a certain way but may still indulge in high calorie foods
* may have poor recovery nutrition
* interested in nutrition - highly motivated
91
New cards
Different type of clients? - the athlete
* can often paint a picture of what they have been told in presentations or what they think you want to know/hear
* context is important, they are being told to see you or have approached you / paying for it?
* try to gain context into their lifestyle - eg body comp history, convos with coaches/trainers etc
* context is important, they are being told to see you or have approached you / paying for it?
* try to gain context into their lifestyle - eg body comp history, convos with coaches/trainers etc
92
New cards
Stages of dietrary assessment
stage 1: determine food intake
stage 2: convert food intake into nutrient intake
Stage 3: interpret nutrient and food intake data
stage 2: convert food intake into nutrient intake
Stage 3: interpret nutrient and food intake data
93
New cards
Dietary assessment methods - Direct - Retrospective
* dietary history
* 24 hour recall
* food frequency questionnaire
* indicators of dietary quality
* screening
* 24 hour recall
* food frequency questionnaire
* indicators of dietary quality
* screening
94
New cards
Dietary assessment methods - Direct - innovative technologies
* personal digital assistant
* image-assisted dietary assessment method
* mobile-based technologies
* interactive computer and web-based technologies
* scan - and - sensor - based technologies
* image-assisted dietary assessment method
* mobile-based technologies
* interactive computer and web-based technologies
* scan - and - sensor - based technologies
95
New cards
Dietary assessment methods - Direct - prospective
* estimated food record
* weighed food record
* duplicate diet model
* weighed food record
* duplicate diet model
96
New cards
Food frequency Questionnaire method
Answers questions about how often they consume particular foods/drinks
Use: large scale studies
important that is has been validated and it relates to the population you are looking at
Use: large scale studies
important that is has been validated and it relates to the population you are looking at
97
New cards
Pros of Food frequency Questionnaire method
* low respondent burden/high compliance
* relatively inexpensive
* high response rate
* usual intakes
* relatively inexpensive
* high response rate
* usual intakes
98
New cards
Cons of Food frequency Questionnaire method
* must be literate/numerate
* questionnaire design crucial
* relies on memory
* over-reporting is common
* not suitable for individual intakes
* questionnaire design crucial
* relies on memory
* over-reporting is common
* not suitable for individual intakes
99
New cards
Diet recall method
Recall all foods and drinks eaten in the last 24 hours
Use: large studies and clinical setting
application to athletes:
* minimal subject burden
* interview can be scheduled around other daily activities
* multiple recalls to reflect different days
* can be used to study a large number of athletes
Use: large studies and clinical setting
application to athletes:
* minimal subject burden
* interview can be scheduled around other daily activities
* multiple recalls to reflect different days
* can be used to study a large number of athletes
100
New cards
Diet recall method - Pros
* collects info on actual intake
* low respondent burden/high compliance
* low cost
* ease and speed of use
* element of surprise
* low respondent burden/high compliance
* low cost
* ease and speed of use
* element of surprise