IBD
1/86
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
87 Terms
What is Inflammatory Bowel Disease (IBD)?
A spectrum of remitting and relapsing, chronic, inflammatory intestinal conditions causing significant GI symptoms.
What are the two major subtypes of IBD?
Ulcerative Colitis (UC) and Crohn's Disease (CD).
Where is Ulcerative Colitis (UC) primarily located?
Mostly limited to the colon and rectum (95%).
Where is Crohns Disease primarily located?
any portion of the GI tract
almost always affects the terminal ileum and cecum
ileocecal valve
What is the first-line treatment for mild-to-moderate Ulcerative Colitis?
Mesalamine-based therapy.
Is Mesalamine generally used in Crohn's Disease?
No
What is Sulfasalazine?
A prodrug that contains 5-ASA linked to sulfapyridine by an azo bond
What is the function of the azo bond in Sulfasalazine?
It prevents absorption in the stomach or small intestine, releasing active 5-ASA in the colon after colonic bacterial azoreductase cleave the bond
Name two second generation prodrug 5-ASA compounds.
Olsalazine and Balsalazide.
Role of coated mesalamine
delayed release, releases drug throughout the GI tract
Role of PH sensitive mesalamine
◦Releases drug in the small intestine and colon
A mesalamine suppository works where?
rectum
A mesalamine enema works where?
distal colon
what is canasa?
mesalamine suppository
what is asacol?
delayed release resin tablet
what is pentasa?
microgranule controlled-release capsule
what is lialda?
MMX formulated pH-dependent polymer film coated tablet
what is aspriso?
enteric coated granules in polyermatrix
where do apriso, balsalazide, lialda, olsalazine, and delzicol work>
proximal colon
where does asacol HD work?
all the way to terminal ileum
where does pentase work?
all the way to jejunum
What are the adverse effects associated with Sulfasalazine?
Nausea, GI upset, headaches, arthralgias, myalgias, bone marrow suppression, malaise, impaired folate absorption, and hypersensitivity to sulfapyridine.
What percentage of patients discontinue Sulfasalazine due to adverse effects?
Up to 40%.
What patients have higher risk of ADEs with sulfasalazine?
◦Slow acetylators have a higher incidence of adverse effects than fast acetylators
How do corticosteroids function in the treatment of IBD?
They suppress acute inflammation and modulate the immune system by inhibiting cytokine production.
How can corticosteroids be administered for IBD?
Parenterally, orally, or rectally.
What is unclear about the effects of corticosteroids in IBD?
Whether the most important effects are systemic or local (mucosal).
corticosteroids role in IBD
Used for the treatment of active UC or CD to induce remission
◦Should not be used chronically to maintain disease remission
Corticosteroids MOA
modulates immune system and inhibits production of cytokines and mediators
corticosteroids used for sevre vs mild IBD
severe disease: burst and taper 1-2 weeks
◦Oral- Prednisone and prednisolone
◦IV- methylprednisolone
Mild to Moderate: topical hydrocortisone, budenoside, oral/topical enteric coated budenoside
enteric coated budenoside ADME
◦Undergoes extensive first pass metabolism that reduces systemic absorption
◦Drug is delivered primarily at the ileocecal junction
can be used for up to 8 weeks
name the synethic glucocorticoid used for retaining UC/Crohns remission
budenoside
*not preferred to be used for maintenance
budenoside ADEs
HA, acnea, nausea, CYP3A4
What are the immunomodulators used in IBD?
Azathioprine, 6-mercaptopurine (6-MP), and methotrexate.
What is the purpose of immunomodulators in IBD treatment?
Monotherapy or adjunctive therapy for patients not responding to mesalamine-based therapy, can help maintain remission achieved with corticosteroids (steroid-sparing effect)
Adjunct to biologics and anti-integrin therapies to add efficacy and reduce risk of antibody formation
immunomodulators
Are immunomodulators used for induction therapy?
no - takes 6 months
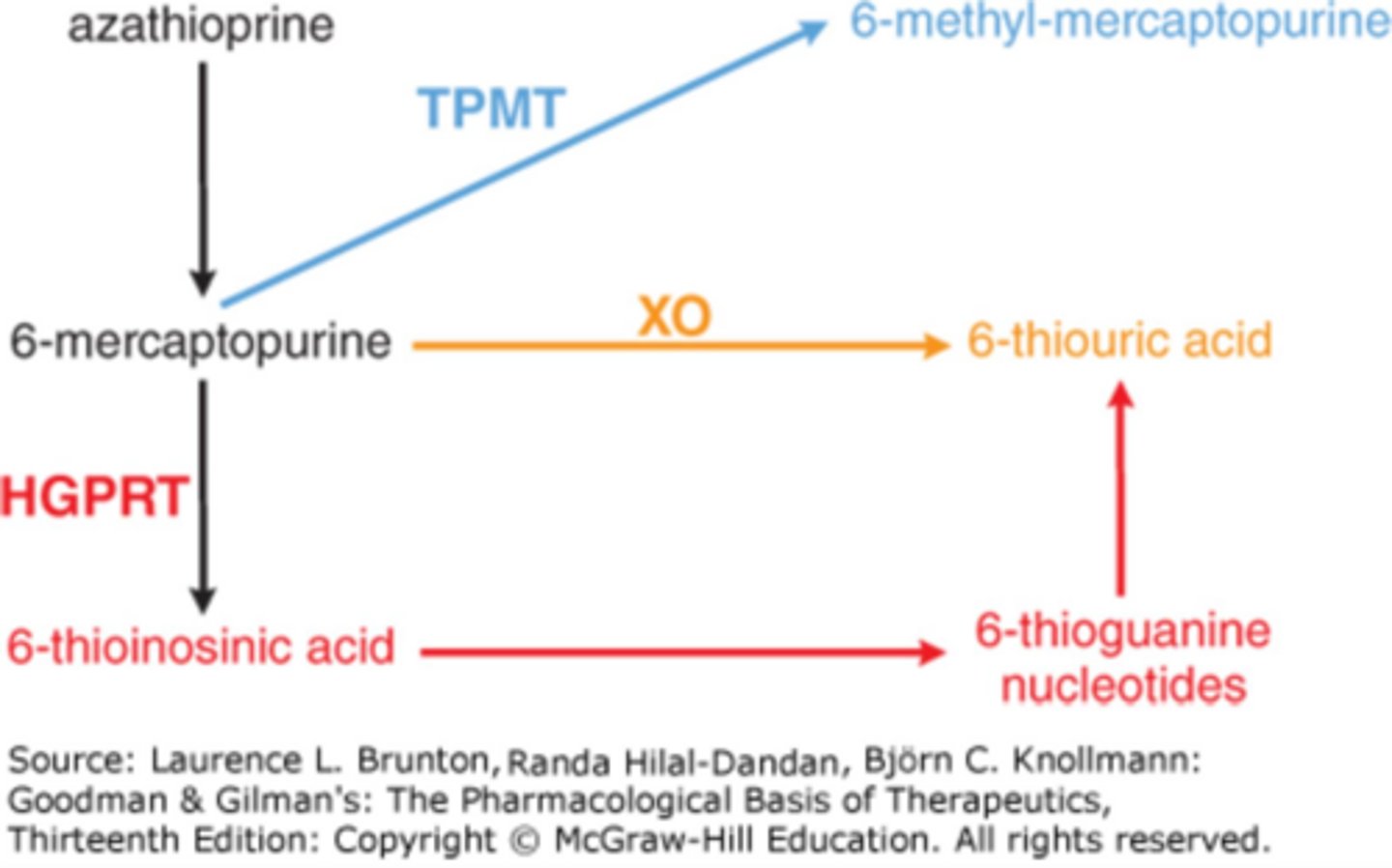
What is the MOA of azathioprine and 6-MP?
Purine antimetabolites with immunosuppressive properties
Impair purine biosynthesis and inhibit cell proliferation
What should be tested before initiating azathioprine treatment?
TPMT activity to assess risk of bone marrow suppression
azathioprine DDI caution
xanthine oxidase inhibitors
azathioprine ADE
◦Idiosyncratic
◦Pancreatitis (5%)
◦N/V, fever, rash arthralgias
- bone marrow suppression
What is the MOA of methotrexate?
Inhibition of dihydrofolate reductase, reducing thymidine and purines production.
◦Used in many chronic inflammatory conditions as maintenance therapy
Methotrexate onset of action
8 weeks
Methotrexate administration
PO, IM, or SubQ once weekly
What are common adverse effects of methotrexate at higher doses?
Bone marrow suppression, megaloblastic anemia, alopecia, mucositis.
*folate supplentation reduces risk
cyclosporine MOA
Calcineurin inhibitor
What is the primary role of cyclosporine in IBD?
Limited to treating specific problems like fistulous complications or severe UC failing corticosteroids over short term
What are the significant adverse effects of cyclosporine?
Renal toxicity, cardiovascular risks, hyperglycemia, gum hyperplasia, hepatotoxicity, hyperuricemia, hirsuitism, hyperlipidemia, hypertension.
*CYP3A4
Name the classes of biologic agents used in IBD.
TNF-α inhibitors
leukocyte adhesion inhibitors
anti- IL23
Anti-IL12/IL23
Which TNF-a inhibitors are used fro both UC and Crohn's
◦Infliximab:
Adalimumab
Which TNF-a inhibitors are used for only Crohn's?
Certolizumab
Which TNF-a inhibitors are used for only UC?
Golimumab
What is the therapeutic effect of TNF-α inhibitors in Crohn's disease?
They lead to improvement in 60% and disease remission in 30% of patients with moderate to severe crohns disease
*Median time to clinical response is 2 weeks
What are the 'big four' things to worry about with TNF-alpha therapy?
Infection risk, malignancy, heart failure, and hypersensitivity disorders.
What should be tested prior to initiating TNF-alpha therapy?
Screening for tuberculosis (TB) and hepatitis B.
name the leukocyte adhesion inhibitors (anti-integrins)
natalizumab
vedolizumab
natalizumab MOA
◦Anti- α4 integrin that binds to CNS-tropic and gut-tropic T cells
Vedolizumab MOA
◦Anti- α4 integrin that binds to only gut-tropic T cells
What is the role of leukocyte adhesion inhibitors (anti-integrins) in IBD?
◦In patients who have failed or cannot tolerate TNF inhibitors
ADEs of anti-integrin therapy
◦Infusion-related reactions
◦Hypersensitivity
What is a serious risk associated with Natalizumab?
Risk of Progressive Multifocal Leukoencephalopathy (PML).
What are the common adverse effects of Vedolizumab?
Headache and nasopharyngitis.
screening specification for anti-integrin therapy
Do not need to screen for TB or Hepatitis with these agents
* Risk of lymphoma is much less than with the TNF inhibitors
Name three IL-23 agents.
Risankizumab, Mirikizumab, and Guselkumab.
*Mike, Gus, and Ris are all 23
Name the IL-12/IL-23 agent
ustekinumab
IL-inhibitors MOA
monoclonal antibody that binds to the p40 subunits preventing activation of interlukin 23 +/-12 which are pro-inflammatory cytokines on lymphocytes
What are IL-23 agents used for in Crohn's disease?
They are used as second-line therapy crohns disease
What are common adverse effects of IL-inhibitor therapy?
Hypersensitivity, infusion-related reactions, TB (test prior), HA, fatigue, injection site reaction, and herpes infections.
What antibiotics are commonly used in Crohn's disease?
Metronidazole and Ciprofloxacin.
What is the mechanism of action of antibiotics in crohns disease?
It may interrupt the inflammatory process directed at the endogenous flora.
when are antibiotics often added to crohns therapy?
◦Often used in patients when fistulas or abscesses are present
What is a potential complication of ileal pouch anal anastomosis (IPAA) in UC?
Pouchitis.
What are common adverse effects of Ciprofloxacin?
Nausea, vomiting, diarrhea, headache, dizziness, and phototoxicity, QT prolongation, increases levels of warfarin and theophylline
Ciprofloxacin BBW
Tendonitis and tendon rupture.
What are common adverse effects of Metronidazole?
Gastrointestinal upset, metallic taste, dark urine, vertigo, ataxia, disulfiram-like reaction, incteractions with warfarin, phenytoin, phenobarbitol
What is the initial treatment for distal mild to moderate active UC?
Oral/topical 5-ASA agents.
Consider reducing ASA to lowest possible effective dose
What is the initial treatment for extensive mild to moderate active UC?
oral mesalamine or budesonide
What is the treatment for moderate to severe active UC?
Budesonide or high-dose prednisone, possibly combined with infliximab or vedolizumab +/- AZA
*need to quickly suppress inflamation
If taking budesonide, try to stop after _ weeks after remission achieved
8
What is the treatment for acute severe or fulminant UC?
Hospitalization with methylprednisolone or hydrocortisone.
What is the treatment for acute severe or fulminant UC with no response to steroids?
infliximab or cyclosporine
What is the treatment for mild to moderate active Crohn's disease - extensive?
Sulfasalazine
What is the treatment for mild to moderate active Crohn's disease - perianal?
metronidazole +/- infliximab
What is the treatment for mild to moderate active Crohn's disease - small bowel?
budesonide
Treatment for Moderate to Severe Active Crohn's Disease
◦Prednisone + infliximab
◦Adalimumab
◦Vedolizumab +/- MTX
◦AZA/6-MP
* off 2-4 weeks after response achieved
Treatment for Moderate to Severe to fulminant
◦Hospitalization
◦Steroids
◦Infliximab prior to surgery as last option
What is the last option for severe Crohn's disease treatment?
Ustekinumab.