5. 2ND REGIMENS for VF ON INITIAL ART AND MDR HIV
1/26
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
27 Terms
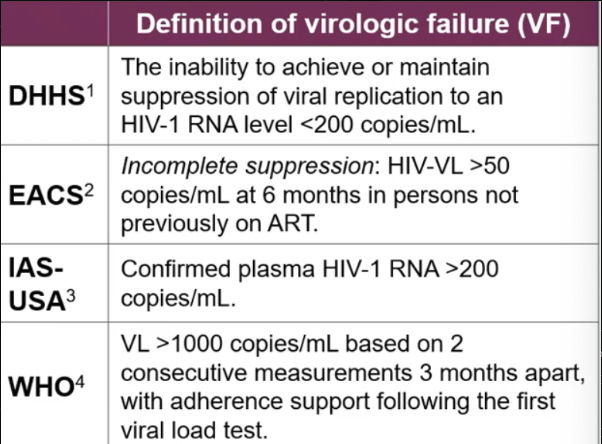
Definition of virologic failure?
HIV RNA >200 copies/ml per US DHHS and IAS-USA
WHO says >1000 copies measured at least twice
EACS says VL >50 6 months after starting ART in naive patients
EACS also defines rebound: confirmed HIV VL >50 copies/ml in persons previously undetectable
When virologic failure occurs, when should resistance testing occur?
PERFORM RESISTANCE TESTING AS SOON AS PWH HIV RNA IS >200 COPIES/ML
Perform resistance testing while STILL on failing regimen or within 4 weeks of DCing it. But treatment interruption is NOT recommend.
In setting of VF, is genotypic or phenotypic resistance testing usually preferred?
Generally Genotypic testing is all that you will need, especially when a patient is on a first or second regimen and resistance patters are not expected to be complex
phenotypic testing may be added as adjunct if there are known or suspected complex drug-resistance mutations
Under what circumstances might it be difficult to obtain drug resistance testing on someone who is experiencing virologic failure (VF)?
If their HIV RNA copies are <500-1000/ml, resistance testing might not work.
You may need to get proviral DNA deep sequencing instead
In an HIV infection that is actively suppressed with ART, how many T cells out of 100K would likely contain HIV DNA in their genomes?
Approximately 10-100 cells per 100K T cells
The number of cells with Replication-competent virus is much lower, typically 1-10 cells in a million cells. (these are the cells that would cause rebound if ART is stopped)
Describe HIV DNA Proviral Assay AKA Deep sequencing vs. Standard plasma HIV RNA testing
Proviral DNA deep sequencing identifies historical/archival drug resistance mutations (DRM) in Tcells, even during complete viral suppression or low level viremia.
Highly sensitive techniques which amplify minute amounts of genetic material from a large population of CD4 T cells and can detect as few as 1 copy of integrated HIV DNA in 40K-100K CD4 T cells.
Standard plasma RNA testing detects only actively expressed mutations from freely circulating virions (both replication-competent and defective virions) in the bloodstream. (these virions may have a fewer number of mutations than what certain Tcells “knows” how to produce.)
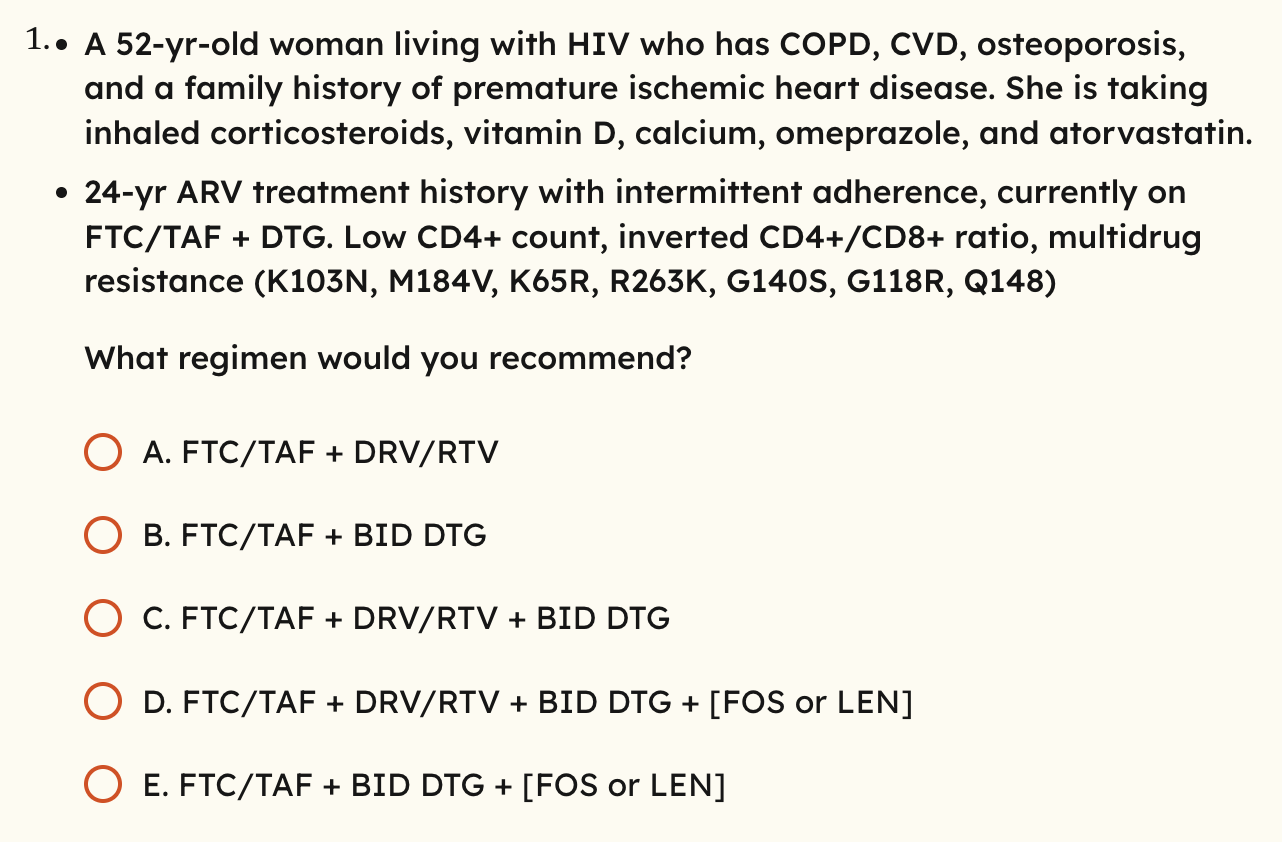
What do you consider when re-constructing a new regimen for someone with virologic failure?
All Current and ALL PRIOR Resistance testing results
AND
Previous ART exposure (full history of drugs taken and drugs failed)
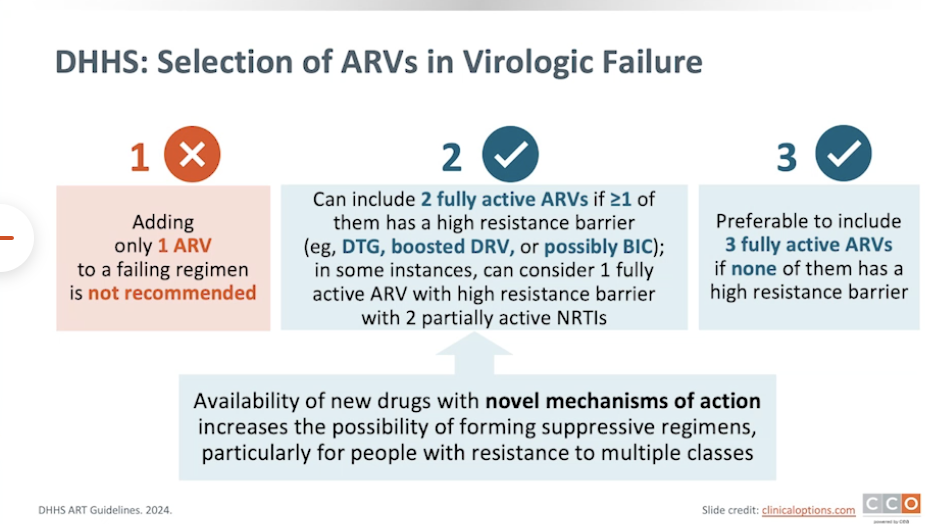
Basic principle is to include ideally 3 fully active agents in the new regimen, even if none has a high resistance barrier.
If it is not possible to select 3 fully active drugs in someone in virologic failure, what is the next best type of regimen?
TWO fully active drugs are OK as long as one of them has a high resistance barrier (DTG, BIC or boosted DRV). + 3rd partial or inactive drug.
In some instances, can consider 1 fully active agent with a high resistance barrier + 2 partially active NRTIs
What did the NADIA study show in regards to NRTIs?
NRTIs have persistent activity even in the setting of partial resistance, specifically when combined with DTG and DRV/r.
NRTIs contributed to full virologic suppression, even in the setting of resistance mutations. i.e. DTG and DRV/r when used as monotherapy did not result in full suppression vs. when they were used to two partially active NRTIs.
If NO fully active drug with a high resistance barrier is available (DTG, BIC, or DRV) as part of an only-TWO fully active drug regimen + 3rd inactive (in the context of 3 fully active drugs not available), whats the next best type of regimen to use?
Do NOT use an “only-TWO” active drug regimen + 3rd inactive
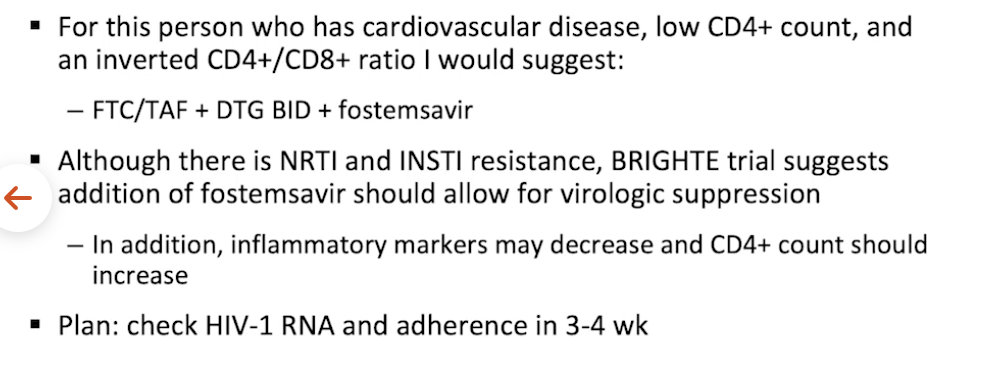
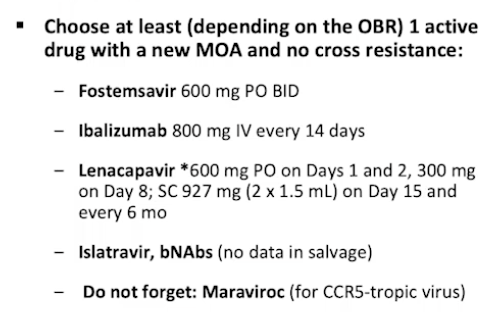
INSTEAD, every effort should be made to include 3 fully active drugs, even if from newer/salvage drug classes. E.g. lenacapravir, miraviroc, fostemsavir, etc.
Another way to think about choosing a regimen in the setting of VF, is that if you do not have full activity of either DTG or DRV, you must consider what?
An agent with a novel MOA and no cross resistance, such as the entry inhibitors.
IM ELF
In the case of MDR HIV resistance, and no possible way to have 2 or 3 fully active drugs, even with newer/salvage classes, what should you do?
Continue ART that minimizes toxicity, preserves CD4 count and delays clinical progression. Even if it cannot fully suppress the virus. Consider clinical trials. Treatment interruption is NOT recommended.
Defer changing their regimen from one fully active to another one-fully active regimen, unless they have CD4 count <100 or with high risk of clinical deterioration
Consider continuing FTC or 3TC, even in documented M184V/I so that you reduce overall viral fitness.
what is the definition of “fully active”?
no predicted resistance based on tx history or resistance testing
novel mechanism of action
may include newer members of existing drug classes that remain fully active against isolates that are resistant to older drugs in the same class
e.g. ETR, DOR, DRV, DTG, BIC
In patients with Multi-class HIV resistance, inlcuding to some INSTIs such as RAL / EVG, what dosing strategy of DTG might overcome that resistance?
DTG 50mg BID.
Or use Bictegravir
What does M184V/I mutation do?
It’s a mutation in RT selected by 3TC and FTC (both NRTIs). It reduces viral fitness, slows HIV progression, and increases susceptibility to other drugs like tenofovir and zidovudine. You can encourage expression of M184V by keeping a patient on 3TC and FTC even after development of M184V/I in the case of multi-class resistance when 3 fully active drugs are not available.
HIV guidelines recommend that when 3 fully active drugs cannot be used due to resistance, it is acceptable to use a regimen with only 2 fully active drugs + 1 partial or inactive drug, IF one of the 2 fully active drugs have a high resistance barrier i.e. _____________
Either:
BIC
DTG
DRV/r
What needs to happen ANY time you are switching regimens in HIV/HBV coinfection?
Make sure you continue an ART against HBV. Even if not active against HIV.
Structured ART Interruption has been a considered strategy in PWH with MDR HIV resistance. However it is NOT recommended. WHY?
greater virologic progression
accelerate CD4 decline
does NOT improve resistance profile
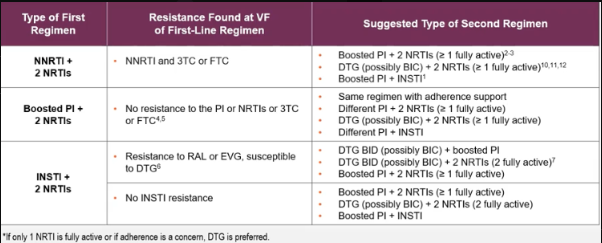
Pts who have failed their INITIAL NNRTI-based initial regimen (NNRTI + 2 NRTIs), often have RAMs to the NNRTI class. plus or minus additional resistance to FTC or 3TC. (for example, if they were on Atripla EFV/TDF/FTC, Complera RPV/TDF/FTC, or Delstrigo DOR/TDF/3TC). What does DHHS recommend as their second regimen?
DO NOT USE ANY NNRTIs
DTG or BIC + 2 NRTIs (at least 1 NRTI fully active. E.g. TDF or TAF + FTC or 3TC in the presence of M184V/I is OKAY)
Boosted PI + 2 NRTIs (at least 1 NRTI fully active. E.g. TDF or TAF + FTC or 3TC in the presence of M184V/I is OKAY)
Boosted PI + INSTI (2-drug) such as DRV/r/RAL (Only if VL <100K and CD4 >200)
Question: Why not TDF/TAF + PI + INSTI?
Why are NRTI + PI + INSTI regimens or NNRTI + PI + INSTI regimens (e.g. regimens with 3 drug classes), not usually recommended in either Naive or VF Patients or mostly even in fully suppressed patients?
The DHHS does not discuss these 3-class regimen types as options for either Naive or VF patients at all. In both cases there is circulating virus.
It seems like the thought is that when there is circulating virus, you cannot risk giving someone all 3 drug classes. In the case they experienced failure to this type of regimen, it would be much more catastrophic since they may have resistance across 3 classes, leaving them with very limited options.
Note that ALL of the DHHS INITIAL regimens AND VF regimens ONLY contain two drug classes.
There is one instance where DHHS guidelines discuss a 3 class regimen, but even so, it’s NOT 1 NRTI + 1 INSTI + 1 PI regimen. What IS the regimen type and In what context is it discussed?
DHHS discusses a 2 NRTI + INSTI + PI regimen and it’s only discussed in the setting of SIMPLIFICATION STRATEGY for VIRALLY SUPPRESSED patients (i.e. protected from resistance d/t low circulating virus) who have resistance to at least 2 ART classes and NO INSTI resistance. The specific regimen discussed is:
EVG/c/TAF/FTC + DRV [GENVOYA + DRV]
Remember, it is RISKY to give patients a regimen with 3 drug classes, lest they fail the regimen and have resistance to all 3.
There was also the ANRS 139 TRIO Trial (not endorsed by guidelines?) showing that a salvage regimen containing raltegravir, etravirine, and darunavir/ritonavir is highly effective for treatment-experienced patients with multidrug-resistant HIV-1. In this study of 103 patients, 86% achieved viral loads <50 copies/mL at 48 weeks
When a PWH fails their initial PI + 2 NRTI regimen type (e.g. DRV/c/TAF/FTC [SYMTUZA]), they usually will still not have any resistance to the PI. Resistance is typically limited to 3TC or FTC. What then, does DHHS recommend as their next regimen?
Continue same regimen with adherence support, as often failure of a PI based regimen is due to lack of adherence, DDIs, or food/drug interactions. Obviously, always obtain resistance testing any time VL >200 copies/ml (VF).
Different PI + 2NRTIs (at least 1 NRTI fully active. E.g. TDF or TAF + FTC or 3TC in the presence of M184V/I is OKAY)
DTG or BIC + 2NRTIs (at least 1 NRTI fully active. E.g. TDF or TAF + FTC or 3TC in the presence of M184V/I is OKAY)
Different PI + INSTI (2-drug) such as DRV/r/RAL (Only if VL <100K and CD4 >200)
When a PWH fails their initial INSTI + 2 NRTI regimen type it is typically because they were taking a non-DTG or BIC containing regimen. E.g. a RAL or EVG regimen such as EVG/c/FTC/TAF [Genvoya], EVG/c/FTC/TDF [STRIBILD], OR RAL + TDF/FTC (truvada), RAL + TAF/FTC (descovy), RAL + ABC/3TC (epzicom). In this case of VF, they typically have resistance to RAL or EVG ± additional resistance to FTC/3TC. They typically maintain use of DTG and likely BIC. What then, does DHHS recommend as their next regimen?
Boosted PI + 2 NRTIs (at least 1 NRTI fully active. E.g. TDF or TAF + FTC or 3TC in the presence of M184V/I is OKAY)
DTG BID or BIC + 2 NRTIs (TWO FULLY ACTIVE!)
DTG BID or BIC + Boosted PI
In the case that they remained unscathed without any INSTI resistance at all, you can use the following:
Boosted PI + 2 NRTIs (at least 1 NRTI fully active. E.g. TDF or TAF + FTC or 3TC in the presence of M184V/I is OKAY)
DTG (QD) or BIC + 2 NRTIs (TWO FULLY ACTIVE!)
Boosted PI + INSTI (2-drug) such as DRV/r/RAL (Only if VL <100K and CD4 >200)
In contrast to a PWH experiencing VF on EVG or RAL + 2 NNRTIs, PWH in VF from DTG or BIC + 2 NRTIs have not been shown to have phenotypic DTG resistance (likely BIC as well). (e.g. BIC/TAF/FTC [BIKTARVY], DTG/ABC/3TC [TRIUMEQ], DTG [TIVICAY] + DESCOVY or DTG [TIVICAY] + TRUVADA). In this case, virologic failure is often due to adherence. What is the recommendation in this case?
The original DTG regimen can be continued with adherence counseling (likely BIC as well),
as long as there is no INSTI resistance detected.
VF of Initial Regimen Table (how to pick second regimens)
What is the utility of the EVG/c/TAF/FTC + DRV [GENVOYA + DRV] regimen?
DHHS discusses a 2 NRTI + INSTI + PI regimen and it’s only discussed in the setting of SIMPLIFICATION STRATEGY for VIRALLY SUPPRESSED patients (i.e. protected from resistance d/t low circulating virus) who have resistance to at least 2 ART classes and NO INSTI resistance.
The specific regimen discussed is: EVG/c/TAF/FTC + DRV [GENVOYA + DRV]
Remember, it is generally considered RISKY to give patients a regimen with 3 drug classes, lest they fail the regimen and have resistance to all 3.