Perio Ch. 13: Host inflammatory response to dental biofilm
1/90
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
91 Terms
The presence of periodontal pathogens alone are
not sufficient enough to cause the destruction seen in periodontitis
What is the inflammatory response?
activated by the immune system system in response to injury or offending agent, traps them and starts to heal tissue, not meant to be activated for a long time
When tissue does not go through resolution phase the result is
chronic inflammation
What is the host immunoinflammatory response triggered by?
the presence of microbial biofilm and its response causes nearly all the destruction seen in perio disease
What is the cause of nearly al the destruction seen in periodontitis?
the body's response to the periodontal pathogens
Immunoinflammatory response
activation of leukocytes and release of pro and anti-inflammatory mediators
The way the body responds to periodontal pathogens is known as the
host response
the prime purpose of the human immune system is to
defend the life of the host
The body's defenses are employed to save the
life of the host, not to preserve the tooth or its supporting periodontal tissues
What are factors enhancing microbial challenges?
virulence factors
Virulence factor
all the mechanisms that enable biofilm bacteria to colonize and damage tissues
Virulence factors may be either:
structural characteristics of bacteria or substances produced by bacteria
Examples of virulence factors
presence of lipopolysaccarides, ability to invade tissues, ability to produce enzymes
Virulence factors: lipopolysaccaride
mature biofilm contains gram negative bacteria which have LPS on their outer membrane and LPS initiatives inflammation in periodontal tissues
host response to microbes involves cells including:
neutrophils, antigen presenting cells, T and B lymphocytes, fibroblasts, epithelial cells
Acute inflammation
has host protective effect, first line of defense, replaces host cells and removes harmful stimuli, created favorable environment for tissue repair
Resolution of Acute Inflammation Following Removal of Microbial Challenge
acute inflammation and resolution most work together and effectiveness of acute inflammation determines whether inflammation is favorable or detrimental
What is catabasis?
return to homeostasis after inflammatory process - complicated process
pro inflammation mediators in periodontitis:
prostaglandins, thromboxanes, prostacyclins and leukotrienes
periodontitis lipid mediators are associated with
recruitment of neutrophils, destruction of connective tissue matrix and resorption of alveolar bone
Over-recruitment or overactivity of PMNs can amplify the
inflammatory process
In catabasis, pro-resolving lipid mediators work in programmed systemic process to
terminate neutrophils to the site, stimulate macrophages to remove dead cells, promote antibacterial activities, promote tissue repair and regeneration
Chronic inflammation
Acute inflammation progresses to uncontrolled, unresolved chronic inflammation - can lead to permanent tissue damage
What is the most numerous perio pathogen that we see?
P. gingivalis
Virulence factor: ability to invade tissue
penetration of bacteria into host tissues allows bacteria to escape host defense mechanisms
Which pathogens can invade most tissues?
P. gingivalis and A.A (both have LPS on cell membrane)
gram negative bacteria tend to be
anaerobic (no oxygen)
Virulence factors: ability to produce enzymes
several bacteria produce enzymes such as collagenases and proteases that can directly degrade host structures in the periodontium
what do collagenases do?
break down collagen
What do proteases break down?
proteins
Certain factors can modulate the hosts susceptibly to periodontal disease such as
genetic factors, environmental factor and acquired factors
genetic factors
age sex etc - non modifiable
environmental factors
smoking - modifiable
acquired factors
diabetes (can be modifiable if uncontrolled and non modifiable if controlled)
Mediators =
the middlemen
What are the mediators?
biochemical sent by host cells to activate the inflammatory response
Inflammatory mediators of importance
cytokines, prostaglandins, matrix mallatoproteinases (MMP's)
First response are
neutrophils which then recruit leukocytes and phagocytes
Biochemical mediator: cytokine
allows cells to talk, many of body cells release cytokines in response to tissue injury or bacteria, signal the immune system to send more phagocytes
Cytokines that are important in periodontitis include:
IL-1 IL-6 IL-8 and TNF -alpha
Cytokines are produced by
neutrophils, macrophages, B cells, epithelial cells, gingival fibroblasts and osteoblasts
What is the function of cytokines?
bind to specific cell surface receptors on target cells and increases vascular permeability, can initiate and perpetuate irreversible tissue destruction in chronic inflammation
Biochemical mediatory: prostaglandins
powerful inflammatory mediators derived from fatty acids that have a large role in initiation of bone destruction in periodontitis which triggers osteoclasts, increase permeability and dilation of blood vessels to promotion increased movement of immune cells to infection site, causes overproduction of destructive MMP enzymes
Important prostaglandins include
D E F G H and I - prostaglandins PGE2 play important role in destruction in perio
What are a major source of PGE's?
macrophage
metalloproteinases role in chronic bacterial infections
without collagen the tissues of the gingiva, pal and alveolar bone degrade which results in gingival recession, pockets and mobility
Biochemical mediators: matrix metalloproteinases
12 different enzymes that break down the connective tissue matrix ; in health they facilitate normal turnover of connective tissue matrix
Overacitvity of MMP's are tightly regulated by
tissue inhibitors of matrix metalloproteinases (TIMP) - helps maintain balance and health of connective tissue
MMPs effects in chronic infection and inflammation:
cytokines and prostaglandins stimulate leukocytes and fibroblasts to release MMPs and releases excessive amounts with intense inflammation
What can inhibit MMP activity?
periostat - 20mg doxycycline
What are a major source of MMP's in periodontitis ?
PMN's and gingival fibroblasts
What is our best response to removal of biofilm ?
mechanical removal NOT antibiotics
some people with abundant biofilm exhibit only
mild disease
others with light biofilm
suffer severe disease
untreated gingivitis does not always
progress to periodontitis ; everyone infected with pathogens will not get periodontal disease
The bone remodeling cycle
osteoclasts - bone resorbing
osteoblasts - bone building
4 phases of bone homeostasis:
resorption, reversal, formation, resting
resorption
break down the bone creating an erosion cavity
reversal
attraction of osteoblasts to build bone
formation
new mineralized bone develops
resting
lengthy, waiting period until next cycle
What is RANKL?
cytokine that activates osteoclasts and promotes bone resorption that is produced and released on the membrane of an osteoblast
Full name of RANKL
receptor activator of nuclear factor kappa - b ligand
Ligand is a
receptor
When does bone resorption occur?
RANKL binds to RANK expressed on the cells surface of osteoclastic precursor cells which then stimulates the precursor cells to differentiate into mature osteoclasts
What is osteoprotegerin (OPG) ?
another protein signaling molecule produced by osteoblasts but unlike RANKL it protects bone from excessive resorption by binding to RANKL which blocks the binding of RANKL to RANK this preserves bone and stablizes the bone remodeling process
Bone metabolism
homeostatic condition occurs when the body can stabilize levels of alveolar bone only when RANKL and OPG are in balance
osteoprotegerin
produced by osteoblasts
bone resorption occurs when
osteoclasts are stimulated to resorb alveolar bone
when the OPG to RANKL levels are out of balance what happens?
osteoclasts resorb alveolar bone
Homeostatic conditions exist when
levels OPG and RANKL are in balance in periodontal tissues and alveolar bone levels stay stable
What are the 4 phases of microscopic changes in periodontal disease?
1. initial lesion - bacterial accumulation
2. early lesion - early gingivitis
3. established lesion - established gingivitis
4. advanced lesion - periodontitis
current theory of pathogenesis: Gingival health is associated with __________ biofilm
symbiotic
current theory of pathogenesis: traditional pathogenic bacteria accumulate when bacterial biofilm is
not disturbed
current theory of pathogenesis: in susceptible individuals what happens?
dysbiotic biofilm activates host response to produce excessive cytokines, MMPs, which lead to collagen breakdown, bone resorption and tissue damage
Risk factors are associated with dysbiotic dental biofilm communities and can:
alter host immunoinflammatory response and impact individuals susceptibility
which prostaglandin is most responsible for alveolar bone destruction?
PGE2
What activates osteoclasts?
RANKL
Who created the histologic stages of development in periodontal disease?
page and Schroeder 1976
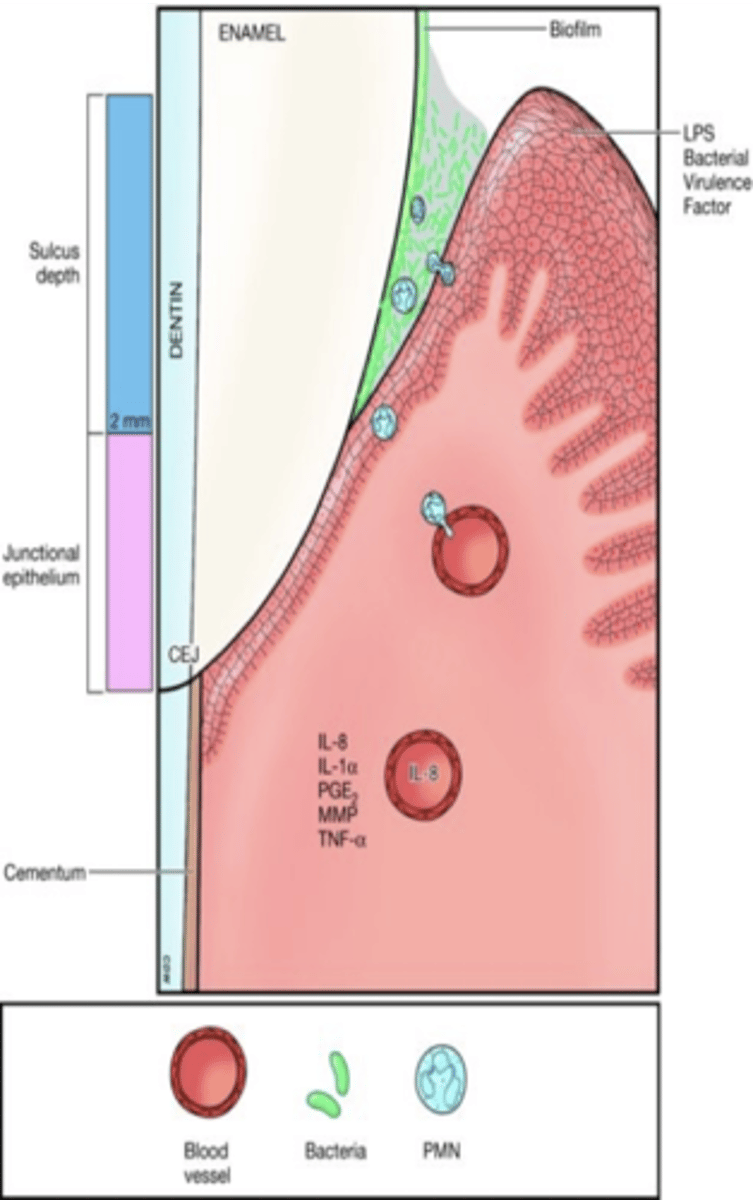
Initial lesion/bacterial accumulation
bacteria colonization near gingival margin, increased vascular dilation and crevicular fluid, neutrophils migrate to the sulcus and at this stage gingiva looks healthy and changes that are occurring are microscopic, initial biofilm accumulation is supra gingival, gram negative bacteria activate complement system
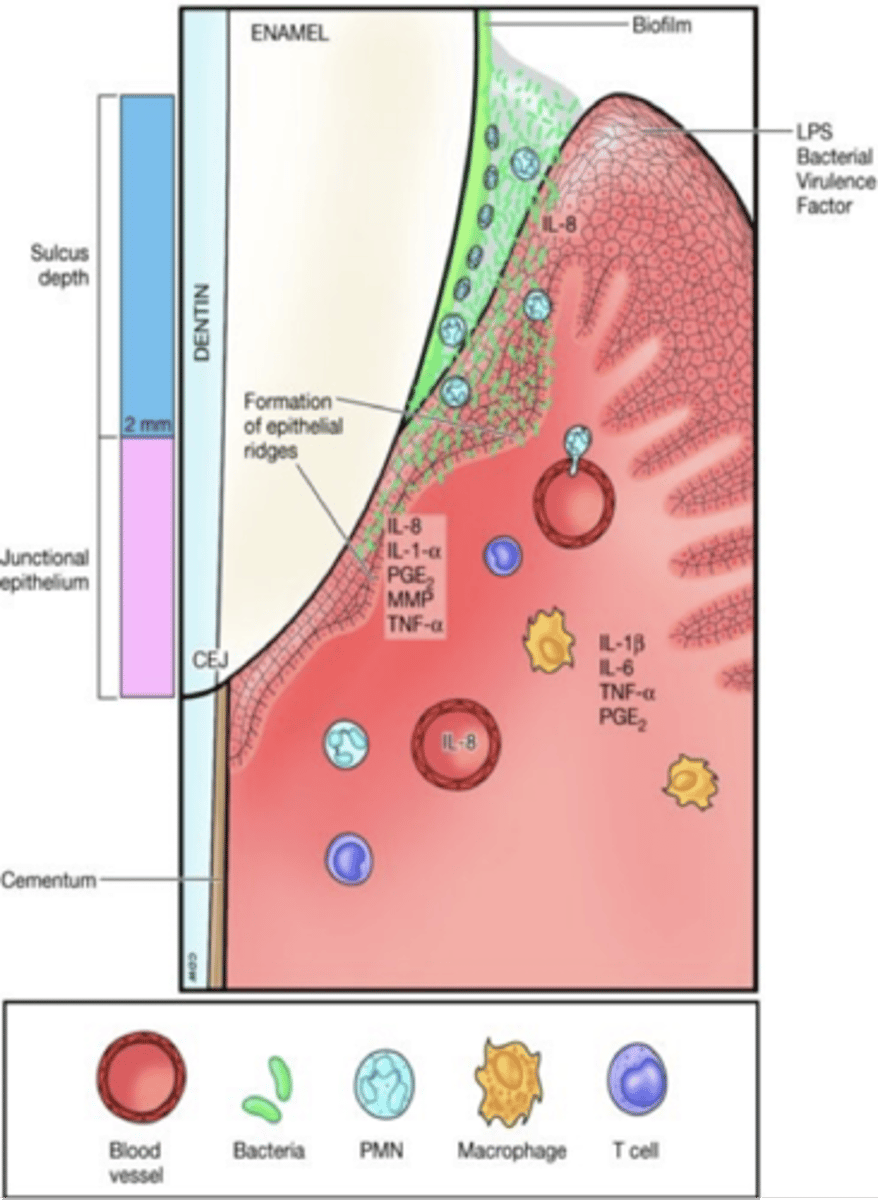
Early gingivitis gingivitis/early lesion
biofilm overgrowth phase, bacteria penetrate connective tissue, more neutrophils attracted to the site and release more cytokines causing more destruction of connective tissue, can see erythema and swelling clinically, good self care can return to health, sucular epithelium and connective tissue most affected and starting forming epithelial ridges and junctional epithelial cells start to proliferate , can return to health w good self care
Initial lesion develops ________ days after accumulation
2 to 4
increased gingival crevicular fluid can cause a
pseudopocket
Early lesion develops ______ days after the accumulation of biofilm.
4-7
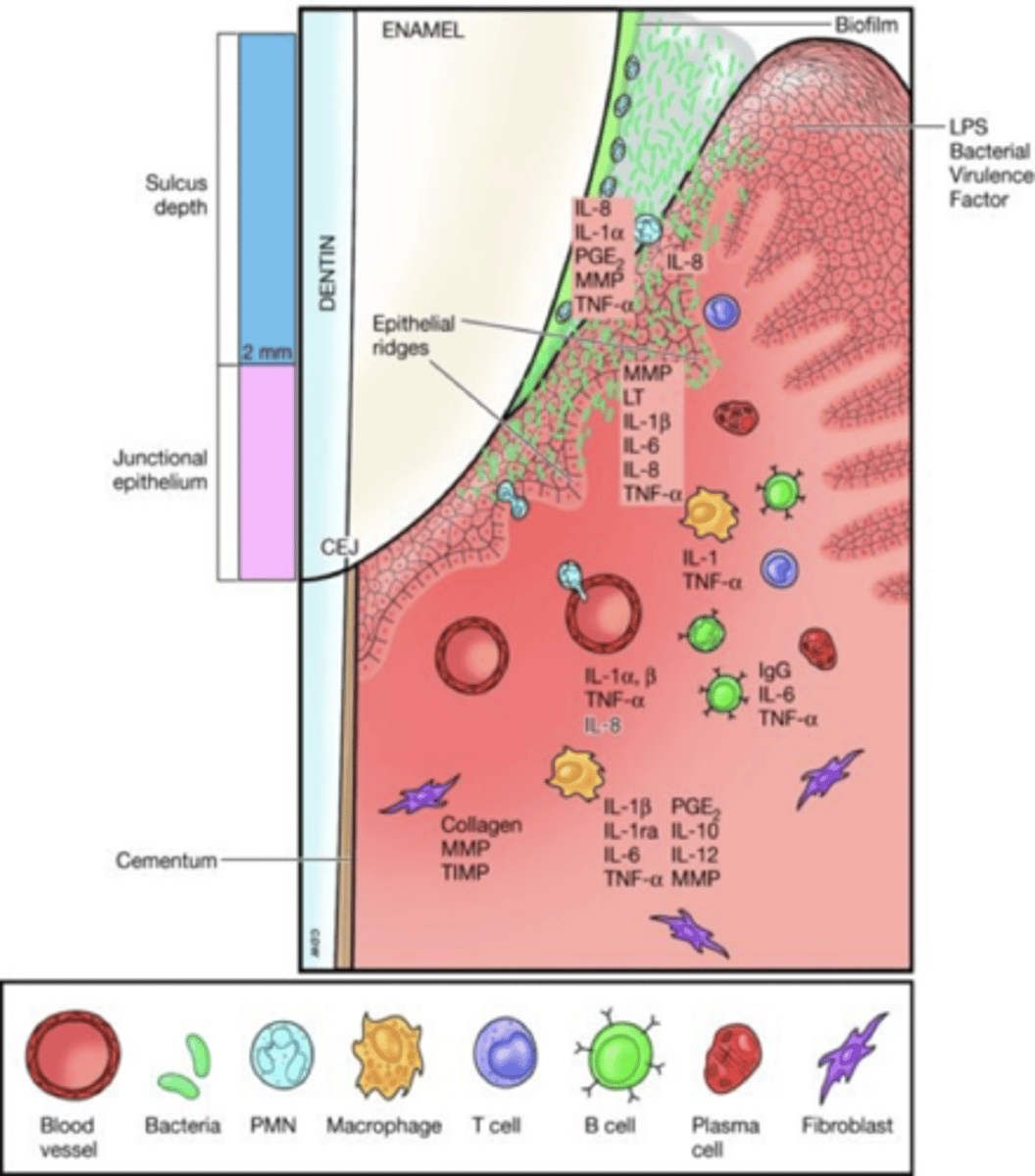
Established gingivitis/established lesion
subgingival plaque phase, biofilm extends subgingival and disrupts attachment of the coronal most portion of the JE, macrophages and lymphocytes are most numerous in the connective tissue and neutrophils continue to fight in the sulcus, host cells produce more toxic chemicals - cytokines, pge2 and mmp's, transforms into deeper pocket, collagen lost, deeper epithelial ridges
It is impossible to know when established gingivitis
will progress to periodontitis bc it is still histologic
Established gingivitis appears ______ days after bacterial accumulation
21
established gingivitis can be reversed with
periodontal instrumentation and pt education and home-care
Advanced lesion/periodontitis
tissue destruction phase ; irreversible damage to the periodontium which is the hallmark of periodontitis, Tissue destruction becomes the main outcome of the immune system response.
The immune response becomes chronic; intense inflammation begins to harm the periodontium.
Cytokines, PGE2, and MMPs destroy the connective tissue, PDL fibers & bone - pocket, biofilm growing laterally and apical on root surface
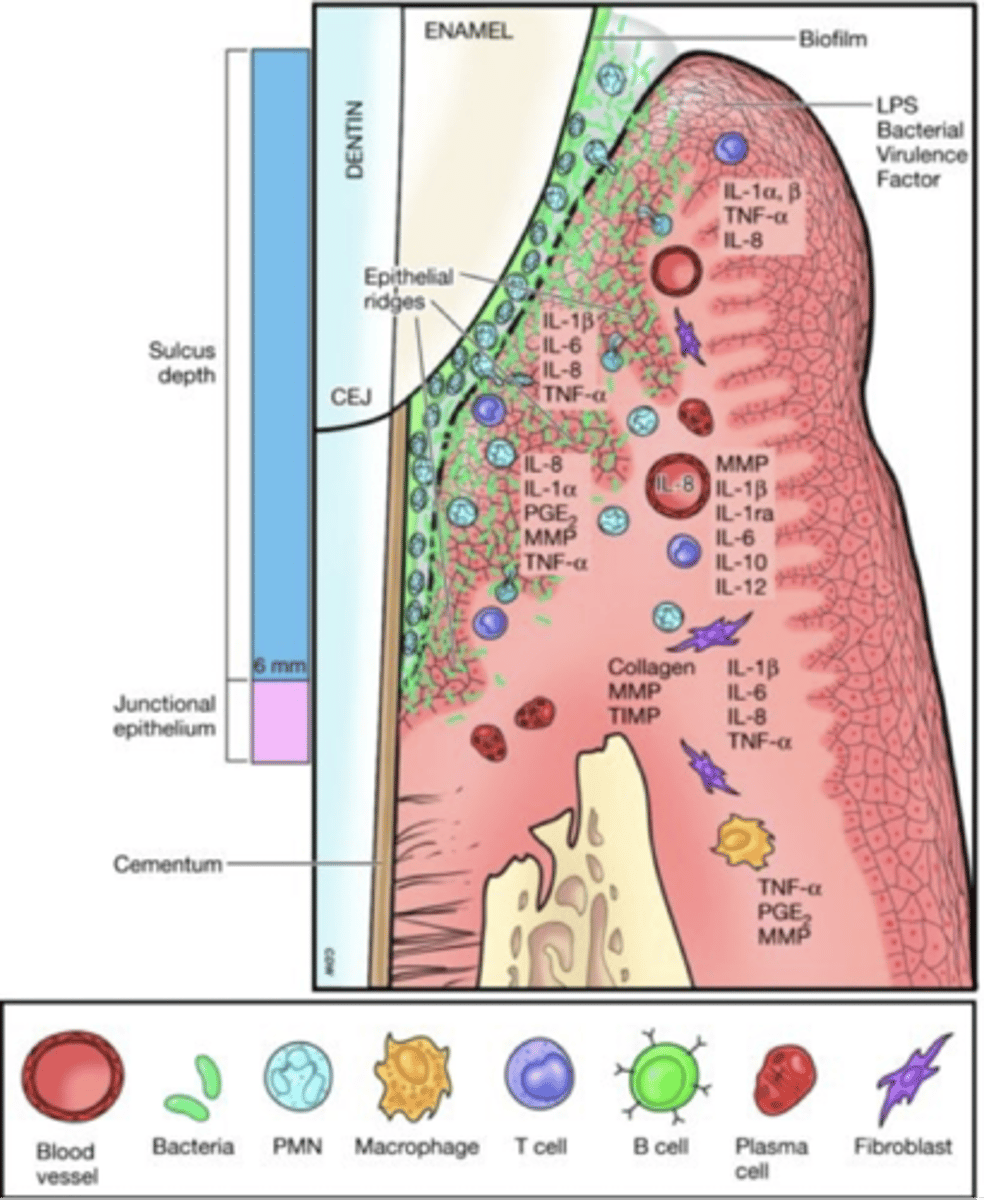
Advanced lesion phase characterized by:
BOP, pockets, destroyed PDL, been loss, furcation and mobility
Factors influencing host's failure to control bacterial challenge:
abnormal PMN function (HIV), acquired, environmental and systemic factors, virulence of bacteria in biofilm