BPK 241 Week 1
1/79
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
80 Terms
Injury Prevention
Reduction of Force
Strengthening of Body Parts
Screening of Participants
Goal of Preventative Medicine
To promote health and well-being and prevent disease, disability and death
Preventative Medicine
Primary prevention
Secondary Prevention
Tertiary Prevention
Primary Prevention
Things we do to prevent injury/ illness
Warm-up
Stretching
Training
Secondary Prevention
Once and injury or illness has occurred
Anitbiotics/ antiinflammators
Rehab to return to original function
Braces/ Taping on return to sport
Tertiary Prevention
Things we do when original function cannot be restored
Reduce long-term impairment
Improve quality of life
Importance of Preparation
Decrease incidence of injuries
Decrease severity of injuries
Forms of Preparation for Physical Activity
General Conditioning (Endurance, Strength, Power, Flexibility)
Specific Training (Sport specific, Individual specific, Skills)
Protective Measures (Equipment, Nutrition, Hydration)
General Conditioning
C.O. = H.R. x S.V.
Fitness is proportional to your resting H.R. over 1 minute
20 to 60 minute exercise, HR > 150 bpm, at least 3 times per week
Strength and Power Training
Resistance (weight) training (PRE)
Isometric (muscle contract but no length moved) vs Isotonic (eccentric, concentric)
Plyometrics
Who, when, why, how
Flexibility Training
who, what, where, how
Sport Specific
Skating, Batting, Pitching, Shooting, Golf swing, Swim stroke
Individual Specific
Foot Speed, Strength, Power, Flexibility
Skills
Gross vs fine motor skills
Open vs closed skills
Equipment
Absorbs energy
Disperses energy
Deflects a blow
Limit excess movement
Nutrition Six Classes
Protein
Carbohydrates
Fats
Vitamins (ADEK vs BC)
Minerals
Water/ Electrolytes
Nutrition Role
Growth, repair, and maintenance of all tissues
Regulate body processes
Provide Energy
Protein (20-25%)
Protein on own does not increase muscle mass
Complex process, related to hormones
Protein necessary, but not primary source of fuel
Extra protein consumed is burned as energy or stored as fat
Carbohydrates (55-60%)
The most efficiently broken down and metabolized form energy (glucose) for the body
Broken down and stored as glycogen in the liver and muscles
Average 150 lbs athletes carries 1500-2000 calories in form of carbs
Fats (15-20%)
Types: Saturated & unsaturated
Not the enemy and the primary fuel for light to moderate intensity exercise
More likely to burn fat than carbs for athletes that maintain low to mod intensity
Avg 150 lbs athletes carries up to 80,000 calories in fat
Consume more unsaturated than saturated fat (eliminates unnecessary calories, but not nutrients)
Vitamins and Minerals
Play key roles in the metabolism of carbs and fats which are your primary muscle fuels during exercise
Involved in the repair and building of muscle protein in response to training
Vitamins ADEK
Fat soluble, excess is stored in body fat, increased risk of toxicity, need to be careful
Vitamins BC
Water soluble, excess is excreted in urine, therefore needs to be replenished
Minerals
Dietary elements found naturally in the earth’s crust, has 20 different types in the body, mostly stored in liver and bones
Some are essential to our health and can only be obtained from what you eat and drink
Major minerals like Na, K, Cl, C, P, Mg, S need 100 mg or more daily
Trace minerals like Fe, Z, I, Cu, Ma, F, Se are needed in smaller amounts, usually less than 20 mg daily
Anemia
Iron deficiency
Water/ Hydration
Essential for survival - used for digestion, temperature control, eliminating waste products, prevent dehydration
Approx 60% of body weight
Dehydration
Not enough water
Amount of blood pumped with each heartbeat decreases
Exercising muscle do not receive enough oxygen
By-products of exercise are not flushed out of the body as regularly as they should be
Exhaustion sets in and the athlete’s performance suffers
Hyper hydration (hyponatremia)
Too much water
Signs of dehydration
Early Symptoms include: Thirst, Headache, Fatigue, Weakness, Dry mouth, Loss of appetite, Muscle cramps
Late Symptoms include: Nausea, Hot to touch, Dizziness, Lack of coordination, Confusion, Fainting
Water loss of > 10 to 20% body weight may = death
Electrolyte Minerals & Hydration
Ingestion of sodium during exercise may help with maintaining or restoring plasma volume during exercise and recovery
Consumption of sports drink helps retain water in the body and aids in hydration by increasing the absorption of fluid from the intestines into the muscles
Researchers suggest 6-8% carb sport drink with at least 110 mg of sodium per 8 ounce serve as a fuel of energy that water can’t provide
Cramping
Excessive sweating with sodium/mineral loss, muscle twitching & cramps
Heat exhaustion
Prolonged period of fluid loss via activity in high temperatures
Heat stroke
Failure of thermoregulatory system
Sudden collapse, loss of consciousness, flushed, hot skin, shallow breathing and rapid pulse, core temp of 106 F or higher
Heat stroke prevention
Fluid and electrolyte replacement
Gradual acclimization
monitor temp and humidity
identify susceptible individuals
weight records
uniforms
ABCDs
Airway
Breathing
Circulation
Disability
Emergency Care General Points
Keep head and neck stable
Keep warm
N.P.O nil per os (nothing by mouth)
Get help
Serial repetition of ABCDs- record status
Shock Definition
The state of insufficient blood flow to the tissues of the body as a result of problems with the circulatory system
Neurogenic Shock
General dilation of blood vessels
Psychologic Shock
Temporary dilation of blood vessels to brain
Cardiogenic Shock
Reduced C.O leads to reduced B.P
Septic Shock
System vasodilation - dilated veins leads to reduced B.P
Hypovolemic
Reduced blood volume leads to reduced C.O./ B. P.
Anaphylactic
System Vasodilation - leads to reduced B.P.
Shock Signs and Symptoms
Result of decreased amount of blood for the circulatory system
Reduced B.P
Hypoxia
Reflexive increase HR (tachycardia, rapid pulse)
Skin cool and clammy (warm and dry if septic shock)
Anxiety, thirst, impaired consciousness
Shock Treatment
N.P.O
ABCDs
Maintain body temp ,elevate legs
Transport to medical center ASAP
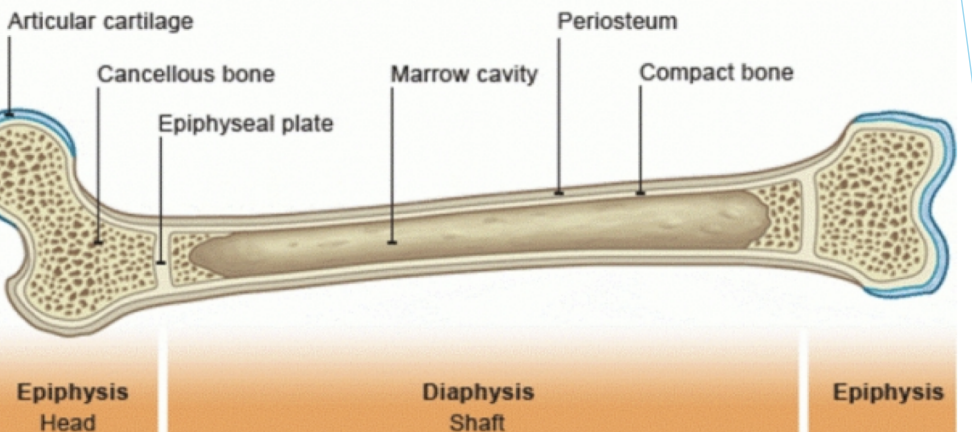
Bone structue
Diaphysis (Shaft)
Metaphysis
Epiphysis
Epiphyseal plate
Periosteum
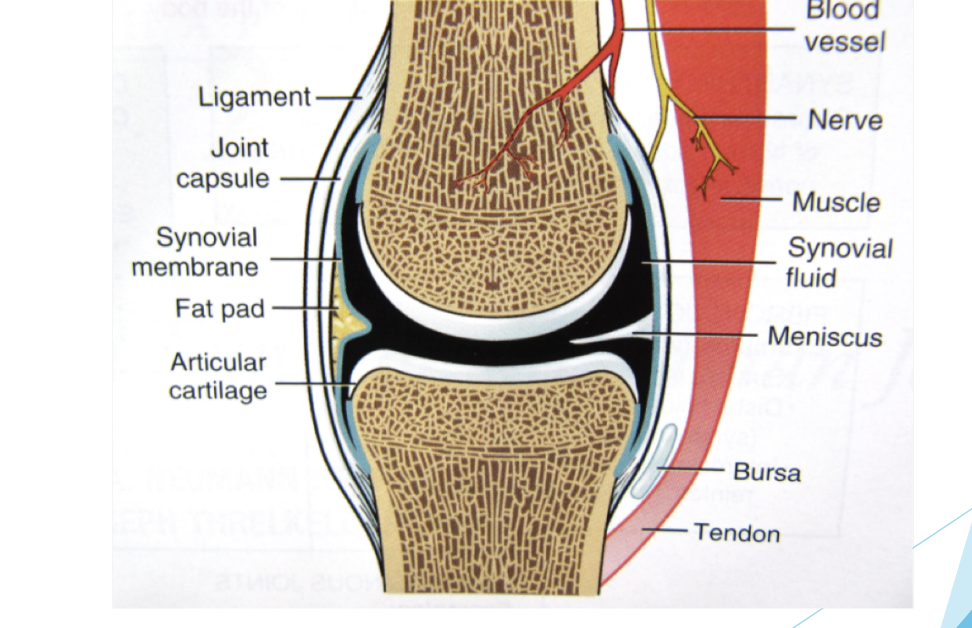
Joint Structure
Bones (which articulate)
Joint capsule/ connective tissue
Synovial membrane and fluid
Cartilage (hyaline vs fibrocartilage)
Bursae
Nerves, blood vessels
Ligaments
Muscle tendons
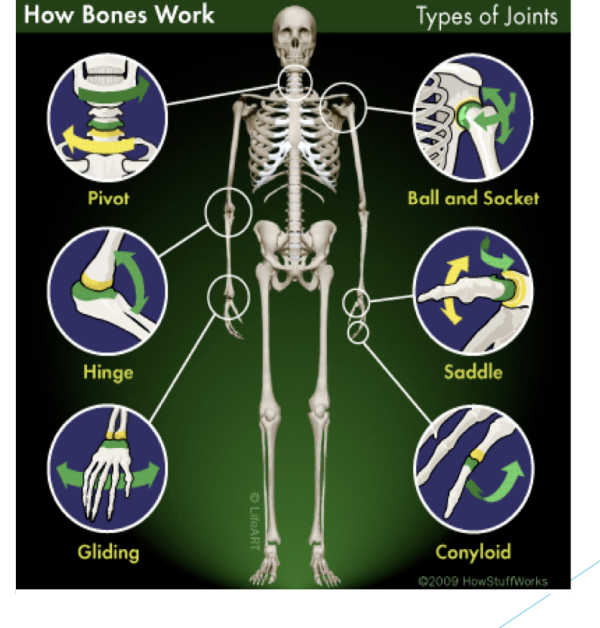
Joint Types
Hinge (elbow)
Saddle (thumb)
Facet (spine)
Pivot (upper C1)
Gliding (wrist carpal)
Ball-and-Socket (hip)
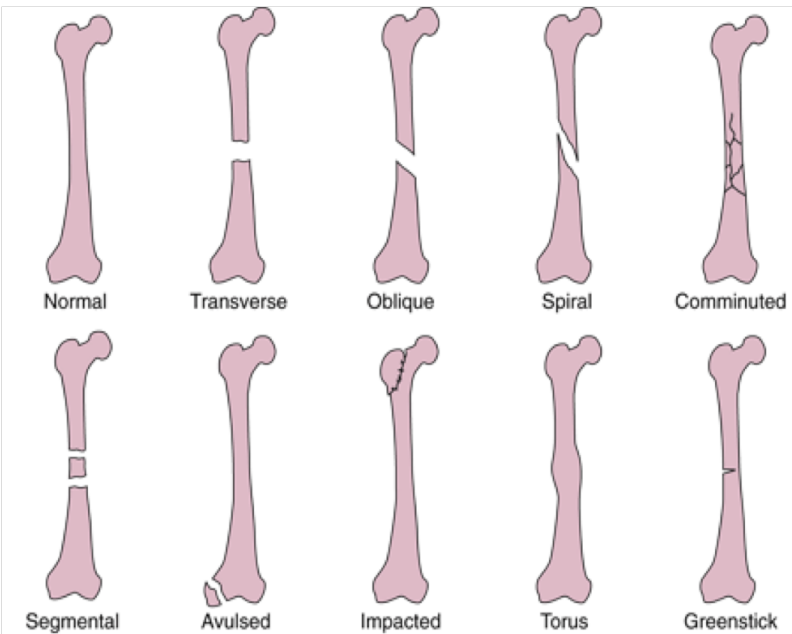
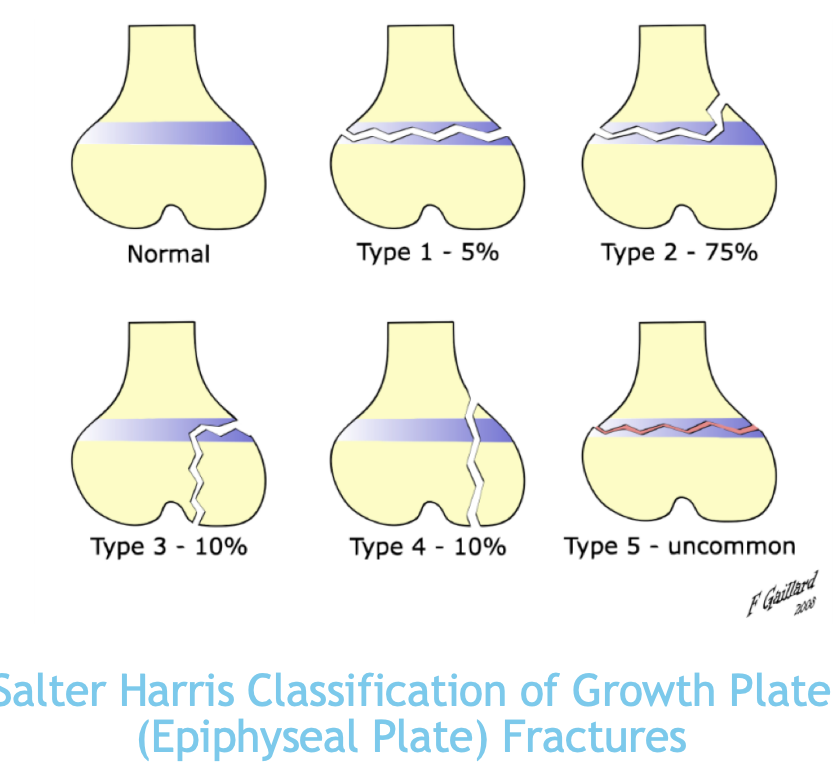
Fracture types
Open (compound) vs Closed (simple)
Varieties (Transverse, Oblique, Comminuted, Spiral, Greenstick, Epiphyseal plate, Segmental, Avulsed, Impacted, Torus)
Acute vs Stress (elastic vs plastic range)
Bone Fracture Continuum
Normal Bone → Stress reaction → Stress Fracture → Full (Acute) Fracture
Osteoclastic activity > Osteoblastic activity
Decreased bone mass perpetuates the problem
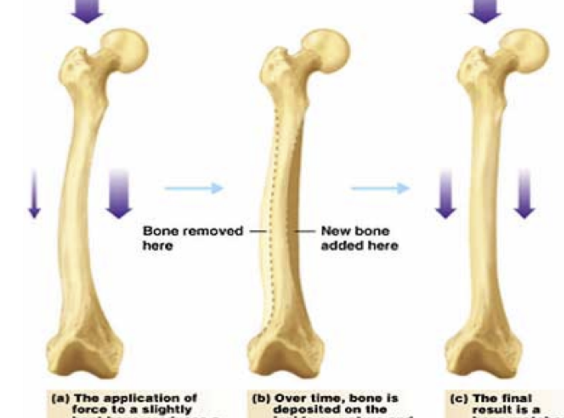
Response of bone to stress
Structure (strength and stiffness)
Load (magnitude, duration, direction, repetitions)
Support (muscle activation, equipment)
Past history
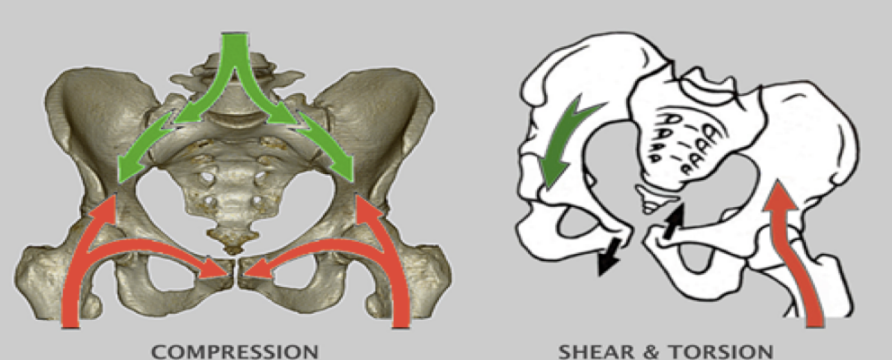
Response of joints to stress
Structure (bone stability, flexibility, capsule, ligaments)
Load (magnitude, duration, direction, repetitions)
Support (muscle activity, braces, tape)
Past history
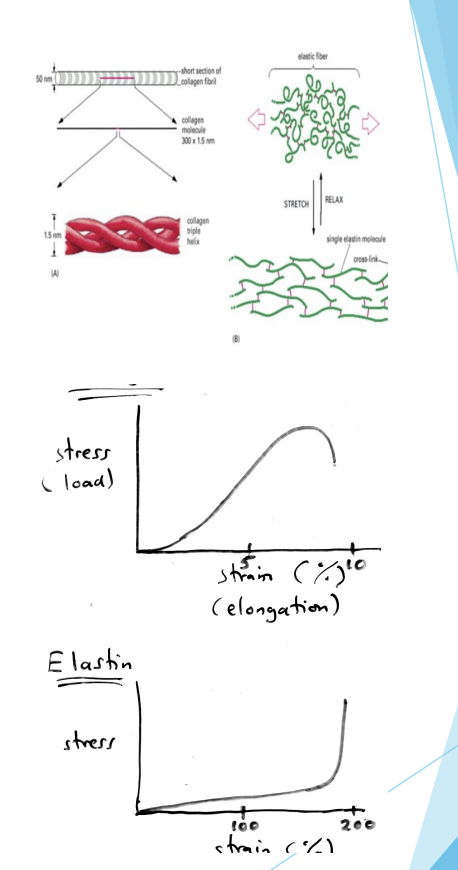
Response of Tissues to Stress
The stronger the tissue, the greater magnitude of load it can withstand:
Load = outside or internal forces acting on body
Mechanical stress = tissue responses to forces
Viscoelastic properties = amount of resistance to stress
Yield Point = elasticity of tissue can no longer hold back stress = mechanical strain (strain or sprain)
Soft Tissue Injury Repair
Acute Inflammatory Phase (0-72 hours)
Proliferation/ Repair Phase (2 days- 6 weeks)
Remodelling/ Maturation Phase (4 weeks - 6 months, longer?)
Inflammation
Protective tissue reaction
“Clinical” if causes pain or disability
Usually a localized, beneficial response to tissue injury
Cardinal Signs of Inflammation
Rubor: increased blood flow
Calor: Increased blood flow
Tumor: fluid accumulation
Dolor: local tissue pressure
Functio laesa: swelling and tenderness
Acute Inflammatory Phase
Consists of two primary events:
Vascular evnets
Cellular events
Vascular and cellular reactions are mediated by chemical mediators, derived from plasma proteins or cells (cytokines) and are produced in response to OR activated by stimuli
Vascular events (minutes to several hours)
Changes in vascular flow (Vasoconstriction and Stasis)
Tissue damage activates the coagulation cascade: Thromboplastin → prothrombin → thrombin → Fibrinogen → Insoluble clot (Quickly followed by Vasodilation → increased blood flow AND increased vascular permeability)
Increased Vascular permeability - Hallmark of acute inflammation and protein and fluid leakage from artery
Vasoconstriction
Blood vessels constrict for a brief period
Stasis
Increased blood viscosity
Cellular Events
Initiated by chemical mediators:
Release from invading organism, damaged tissue, WBC’s involved in inflammatory response
Margination
Rolling
Adhesion
Migration (diapedesis/extravasation
Migration → chemotaxis
Inflammation Benefits
Supplies things to injury site
Clotting factors
Anti-infection materials & processes:
Leukocytes
Phagocytes (macrophages) - eat damaged/destroyed cells
Antibodies
Stick micro-organisms to phagocytes
Attack foreign cells (e.g., put holes in their membranes)
Nutrients (O2, amino acids, glucose)
Stimulates proliferation of endothelial cells (neovascularization) & fibroblasts (cells that synthesize collagen and extracellular matrix)
Edema
Restrict blood flow if no room for swelling
Produce pain, which can limit movement
Excessive or chronic inflammation may → tissue destruction, fibrosis, and necrosis (death)
Acute vs Chronic inflammation
Acute: immediate, few days and resolution, abscess formation
Chronic: delayed, up to many months or years, tissue destruction, fibrosis, necrosis
Systemic Manifestations
Fever
Leukocytosis
Myalgia
Arthralgia
Malaise
Chills
Inflammation Treatment
Remove underlying cause
Incise and drain abscess
Antibiotics
Remove foreign body
Remove Mechanical stress
Treat local effects
POLICE, then heat
NSAID drugs
Physio, Chiro, RMT, Acupuncture, Naturopath
Treat systemic effects
Antipyretics (ASA, acetaminophen)
Analgesics (NSAIDS, narcotics)
Antibiotics
Inflammation types
Myositis
Arthritis
Tendonitis
Bursitis
Vasculitis
Dermatitis
Proliferation/Repair Phase (2 days- 6 weeks)
Characterized by proliferation of capillaries (neovascularization) and fibroblasts which synthesize granulation tissue aka scar tissue (a collagen and extracellular matrix with cross-linking)
Collagen initially is laid down in random fashion and is predominantly Type III collagen
As the quantity of collagen at the injury site increases, the number of fibroblasts decrease
More Type III, less Type I collagen. Weak (H-bonds), rather than covalent bonds, between collagen fibres) and susceptible to re-injury
Poorly vascularized and Disorganized
Remodelling/Maturation Phase (4 weeks - 12-24 months)
Starts 1 to 2 weeks post injury
Long term process that involves realignment & maturation of collagen fibres that make up scar tissue
Myofibroblasts re-orient collagen fibrils in the direction of loading
Increased stress and strain causes collagen fibres to realign to position of maximum efficiency
Parallel to lines of tension
Gradually assumes more normal appearance and function
Lasts 10-12 months, total maturation phase may take years to be fully complete
Remodelling/ Maturation Phase Movement
Increases synthesis
Increases lysis
Reorganizes - decrease in weaker type III collagen, increase in stronger type I collagen
Importance of this stage overlooked since patients stop doing rehab exercises once acute pain and disability are gone
Rehab isn’t done for a year or more; stopping before complete increases risk of re-injury
Phases of Soft Tissue Injury Repair
Inflammation (days to several weeks)
Proliferation (several weeks to month)
Remodelling aka Maturation (a year+)
Wound Healing Mechanisms
Scar tissue formation and Regeneration
Wound Healing Tissue Types
Labile
Stable (smooth muscle, glands, connective tissue)
Permanent (cardiac and skeletal muscle, neurons)
Primary Union
Clean incision
Edges well - approximated
Smaller scar, rapid healing
Secondary union
Large, irregular wound
Contamination
Larger scar, slower healing, dysfunction
Factors that influence Healing
Local:
Location of wound, Extent of Injury, Edema, Hemorrhage, Poor Vascular Supply, Separation of Tissue, Muscle Spasm, Atrophy, Infection
Systemic:
Blood Supply
Corticosteroids
Health/Age/Nutrition
Ice
Vasoconstriction (Hunting Response)
Decreased bleeding into injured tissue
Decrease in inflammatory response
Decreased swelling
Decrease pain - decreases excitability of free nerve endings (nociceptors)
Decreased muscle spasm
Decreased cellular damage - low secondary tissue hypoxia
Implications of Cold on Performance
Decreased pain sensation
Golgi Tendon organs less sensitive
Muscle spindles less sensitive
Increase stiffness at myotendinous junction
Muscle more susceptible to fatigue if cooled below 25 C
Heat
Vasodilation - increased blood flow
Increase in inflammatory response
Increased swelling
Decreased pain
Decreased muscle spasm
Decreased stiffness of soft tissues
Increased metabolism within cells that are warned
Critical temp threshold for beneficial effects is 39 C
Can be achieved by 15 min of general exercise
Types of vascular events
Vasoconstriction (seconds)
Vasodilation (minutes)
Permeability Increase - oedema formation