8) Rumination and Metacognition - Anmol Guest Lec
1/10
Earn XP
Description and Tags
The role of metacognitive beliefs regarding rumination in the depressive experience - for Test 3
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
11 Terms
why is Depression often referred to as a remitting,
recurring disorder?
50% of people remit within one year without treatment
inter-episode remissions = an individual experiences periods between major depressive episodes where their symptoms significantly decrease or disappear entirely, allowing them to return to a normal or near-normal level of functionin- but then depressive episode can come back
Most episodes of depression are characterized by periods of stasis punctuated by sudden changes (“sudden gains”, “spikes”) in depressive symptom

Sudden Gains and Depressive Spikes
what causes sudden gains
what happens after a gain
Depression typically shows:
Long periods of stasis
Sharp “sudden gains” or “spikes” (large, rapid changes)
Supporting studies:
looked at depressed ppl before and after doing CBT sessions (2/wk), n=61
Defined a sudden gain as:
≥ 7-point drop
≥ 25% decrease from prior score
what causes gains
Improvements in therapeutic alliance (we see gain between pregain session and after gain session)
Cognitive change, specifically:
Insights into beliefs relevant to the depressive episode
Patients who experience sudden gains often show:
Patients showing rapid early response + later spike → lower eventual depression symptoms
The spike was associated with:
↑ processing
↑ insight
Lack of spike was associated with:
Avoidance
Implication: Cognitive work during gains leads to long-term improvement.
depressive symptoms spike up as they relaize something, but then drops down to lower than before as the realization helps them
patients with no gain = do not improve in symptoms
Hypothesized liner and circular model of spontaneous remission
which one has more robust support
Key concepts:
RCA (Root Cause Analysis) – identifying causal factors that could have prevented the problem
PSA (Problem-Solving Analysis) – using causal understanding to design solutions
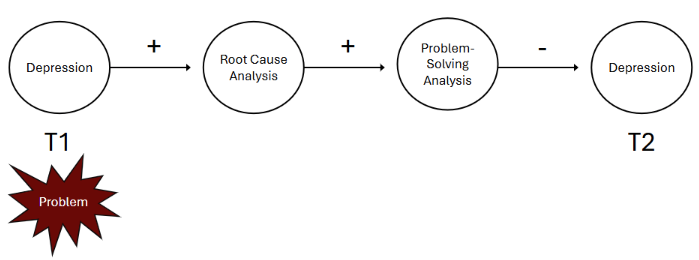
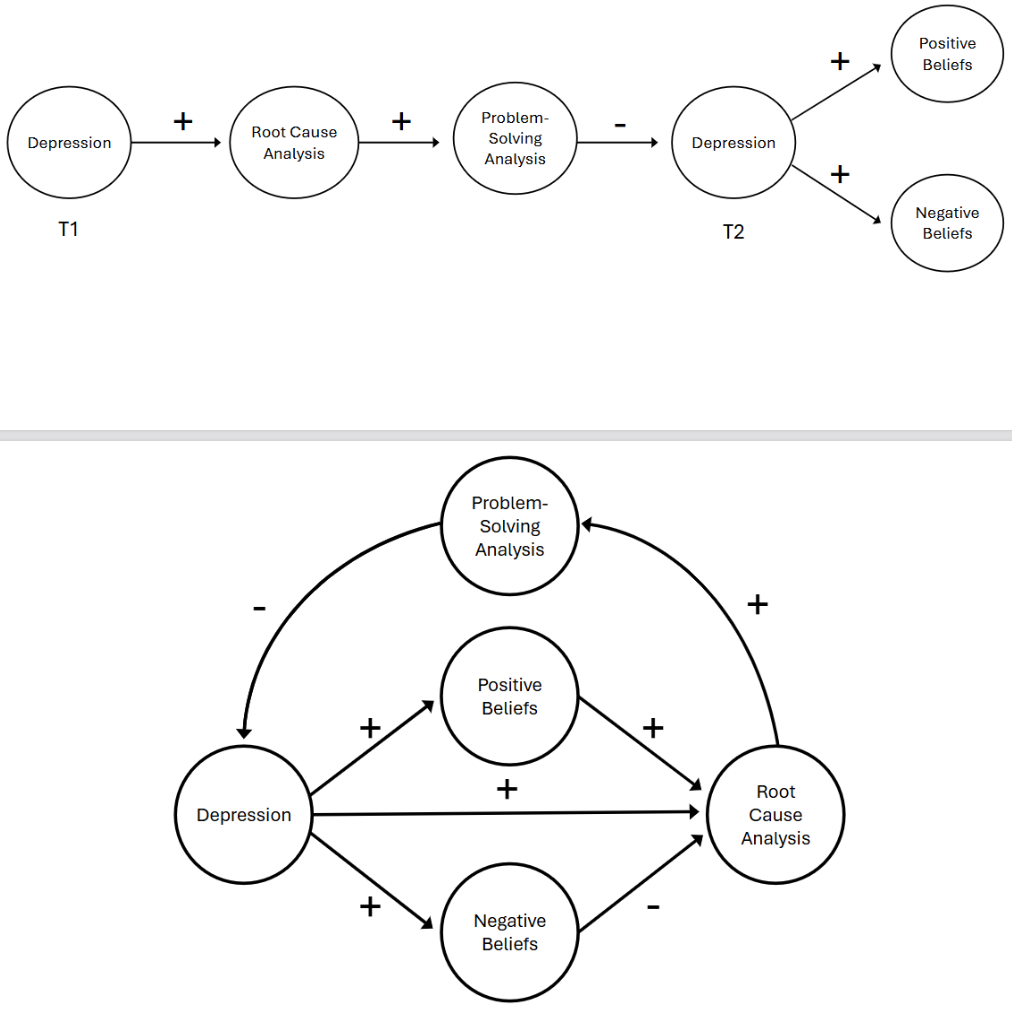
linear Hypothesized Model:
Depression → Root Cause Analysis → Problem-Solving Analysis → less depression (note spike in depression)
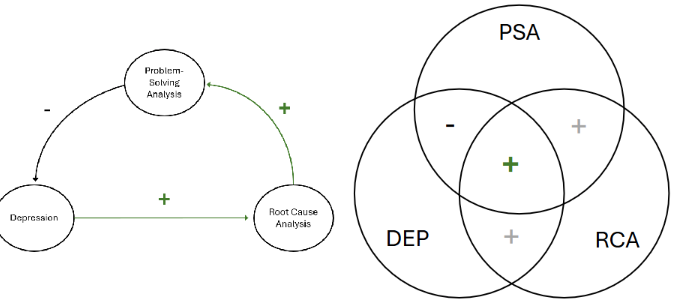
circular hypothesis model: MORE ROBUST SUPPORT
Reciprocal process → circular system.
Depression → (+) → RCA
RCA → (+) → PSA
PSA → (–) → Depression
in the middel circle its overall positive bc Bivariate correlations (simple correlations) between:
Depression (DEP)
RCA
PSA
→ hover around 0 to 0.2
This occurs because:
The circular model includes opposing effects that cancel out in simple correlations.
Modeling Spontaneous Remission - longitudial vs cross sectional data
Longitudinal:
Captures dynamic changes → sudden gains, spikes
Linear model works (variables not in equilibrium)
Cross-sectional:
Represents a snapshot during a stable period
Depression, RCA, and PSA are in temporal equilibrium
→ Use a circular model
does depression promote problem- solving
depression does not promote general problem solving
it promotes problem solveing analysis - founded in a causal understanding of the problems.
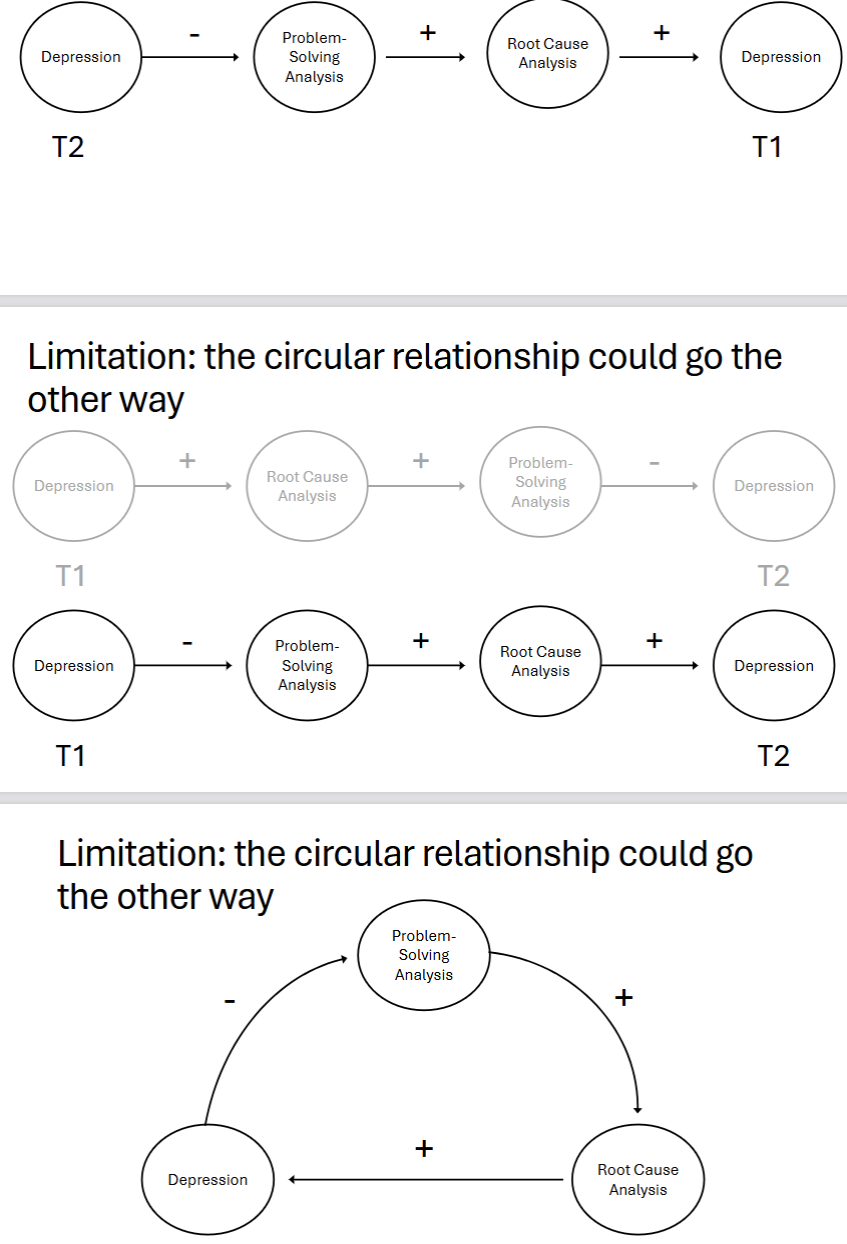
Limitations for circular model of depression
Could the circular relationship go the other way?
Reverse model proposed:
Depression inhibits PSA
RCA increases depression
PSA increases RCA (harder to justify)
Reason against reverse model:
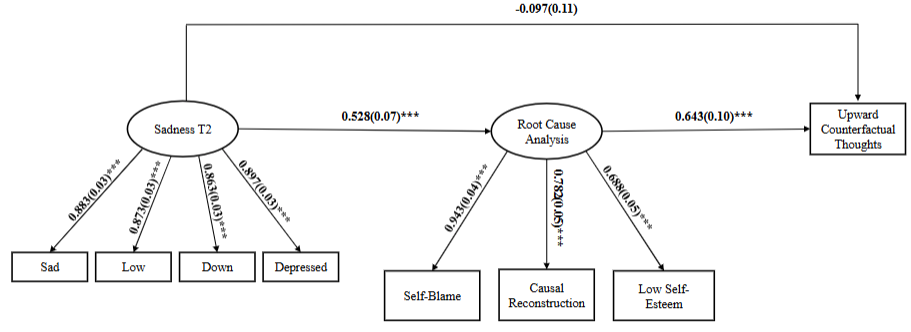
Evidence (e.g., Cyberball writing studies) shows:
RCA precedes PSA
RCA → upward counterfactual thoughts (a PSA component)
Thus RCA → PSA order more plausible.
Sequential Model of Rumination
FMR shifts the perspective of rumination from a simply repetitive thinking style to a breakdown in the natural, smooth progression of thoughts and experiences in conscious awareness.
metacognition
def
2 types of metacognitive beliefs abotu rumination
role in rumination and depressive experience
Metacognition = higher-order thinking that monitors, controls, and regulates cognition.
2 types
Positive metacognitive beliefs about rumination (PMBR) = engage in rumination intentionally, for learning/problem-solving
“I need to ruminate to find answers.”
“Rumination helps me understand/control my depression.”
“Thinking about past mistakes helps prevent future ones.”
“Rumination means I care.”
Negative metacognitive beliefs about rumination (NMBR) = view rumination as uncontrollable, harmful, unproductive
“Rumination is uncontrollable.”
“Rumination makes me more depressed.”
“When I ruminate, I can’t do anything else.”
“Rumination is harmful.”
why did the conventional clinical model of depression believe both PMBR and NMBR worsen depressive symptoms?
why is this wrong?
bc:
PMBR encourage rumination, which is clinically believed to be an “unhelpful” and “passive” cognition that worsens depression.
NMBR are thought to cause “emotional disturbances” in response to the “negative consequences” of rumination itself.
class version of a metacognitive model of depression:
Depressive rumination is necessary for problem-solving
Problem-solving is adaptive
Therefore:
PMBR = beneficial because they encourage productive rumination
NMBR = reduce rumination engagement → may slow remission
Integrated in the linear model:
Depression
→ RCA
→ PSA
→ reduction in depression
↑ PMBR facilitate this process
↓ NMBR may hinder it
PMBR → positively linked to RCA and PSA pathways
NMBR → expected negative effect on RCA was not significant
→ suggests more complexity
key takeaways
Depression promotes RCA-based problem-solving through rumination
This explains why depression looks unproductive clinically but may be productive long-term
Sudden gains/spikes reflect insight and processing increases
PMBR appear to support natural remission processes
NMBR did not significantly disrupt RCA
Circular model explains spontaneous remission
Rumination plays a functional role in resolving depressive episodes
what is better - CBT or ACT?
CBT → treats rumination as harmful; tries to suppress/interrupt
ACT / Mindfulness-Based CBT → don’t suppress; encourage nonjudgmental observation
Class model suggests:
Rumination is instrumental in recovery
It promotes causal understanding + problem-solving
PMBR may be beneficial
Therapy could help patients understand that:
Rumination is not always harmful
It may help resolve depressive episodes
Encouraging structured, reflective rumination might improve outcomes