Somatic Symptoms Disorders
1/10
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
11 Terms
somatoform disorders
Physical symptoms that suggest a medical illness, but have no identifiable physical basis
Diagnosis is very difficult, and requires ruling out multiple medical causes (MS, lupus, Lyme’s disease), conscious production of the symptoms (factitious disorder and malingering), and other mental illnesses (borderline personality disorder, obsessive compulsive disorder)
Problems are often described vividly, but with little factual or concrete information
general etiology of somatoform disorders
Cognitive factors such as appraisal of body sensations, attentional focus, and catastrophizing
Somatic amplification
Learning through experience or vicariously about
disease
Psychoanalytic explanation:
Individuals with a tendency to suppress emotions may
express psychological pain physically
Less likely to seek treatment than other disorders, although CBT has been shown to be fairly effective
Gate control theory of pain
All parts of the body send sensory signals to the brain, but few enter consciousness
A system in the dorsal horn of the spinal cord acts as a “gate,”, by inhibiting the pain sensations from being transmitted to the brain
Physical and psychological factors can open or close the gate
Ascending pathways: other sensations (touch, vibration)
Descending pathways: thoughts, beliefs, emotions, expectations
somatic symptom disorder diagnostic criteria
A. One or more somatic symptoms that are distressing or result in significant disruption of daily life
B. Excessive thoughts, feelings, or behaviours related to the symptoms or health concerns shown by one of:
Disproportionate and persistent thoughts about the seriousness of the symptoms
Persistently high level of anxiety about health or symptoms
Excessive time and energy devoted to these symptoms or
health concerns
C. Usually at least six months duration
somatic symptom disorder
Specifier: With predominant pain
The primary symptom is pain
Must be diagnosed by excluding purely medical causes, and psychologists are not equipped to do this on our own
Even if there are medical reasons, a patient might still be diagnosed with somatic symptom disorder if the distress or impairment are considerably more severe than expected
Numerous brain pathways affected in chronic pain
High levels of excitatory neurotransmitter activity (glutamate)
Greater activity in areas involved in interoception (posterior cingulate)
Neurotransmitter abnormalities are correlated with catastrophizing
Point prevalence of around 1%, but varies greatly depending on strictness of criteria used (eg: prevalence of “medically unexplained” symptoms is much much higher)
conversion disorder diagnostic criteria and specifiers
A. One or more symptoms of altered voluntary motor or sensory function
B. Clinical findings provide evidence of incompatibility between the symptom and recognized neurological or medical conditions
C. The symptom or deficit is not better explained by another medical condition or mental disorder
Specifiers:
With weakness or paralysis
With abnormal movement
With swallowing symptoms
With speech symptoms
With attacks or seizures (psychogenic non-epileptic seizures)
With anesthesia or sensory loss
With special sensory symptom
With mixed presentation
conversion disorder
Transient symptoms are common, persistent problems are very rare
One year incidence <0.005%
About 5% of referrals to specialized neurology clinics
Relative lack of concern over the symptoms; rare, but historically was considered a major feature of conversion
Certain types of conversion are particularly common in medical professionals
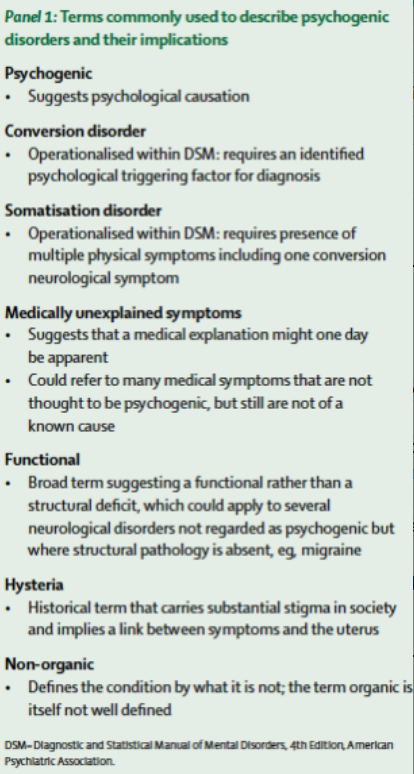
Historically (as far back as the ancient Greeks), this condition was considered to only affect women and to be somehow related to reproductive functioning, hence the former term “Hysteria”
Freud: Unconscious conflicts are repressed but need to be expressed somehow
“The body expresses what the mind cannot”
CBT explanation: abnormal motor/sensory behaviour is an escape behaviour (negatively reinforced)
Extreme variation of normal behaviour, where awareness
or control of motor/sensory are occasionally “switched off”
in order to avoid something (usually anxiety)
Patients with conversion tremor were compared to themselves when voluntarily reproducing the tremor (Voon et al, 2010)
Activity in areas relating to deliberate movement (motor cortex) did not differ between conditions
Less activity in the temporal parietal junction (TPJ), and fewer connections to brain areas involved in deliberate
motor movement
TPJ compares predictions with actual results, in terms of body movement and sensation
In other words, the movements were indistinguishable from voluntary, except for a brain abnormality that resulted in conversion tremors being perceived as involuntary
illness anxiety disorder (formerly hypochondriasis) diagnostic criteria and specifiers
A. Preoccupation with having or acquiring a serious disease
B. Somatic symptoms are not present or, if present, are only mild in intensity
C. High level of anxiety about health and easily alarmed about personal health status
D. Performs excessive health-related behaviours or maladaptive avoidance
E. Illness preoccupation for over 6 months, thought the specific illness feared can change
Specifiers:
Care-seeking type
Care-avoidant type
illness anxiety disorder
Health concern may become a part of the patient's identity
Prevalence estimates vary wildly, but probably around 1-5%
Roughly equal numbers of men and women
Often consider minor physical signs to be symptoms of catastrophic illness (heart disease, stroke, AIDS)
In illness anxiety disorder, the anxiety is due to belief that the person has the disease, even despite reassurances (which only very briefly reduce anxiety, if at all)
In specific phobia of illness, anxiety is about the possibility of contracting illness
In OCD there are excessive and stereotyped rituals, and usually worries about contamination of others
factitious disorder diagnosis criteria
A. Falsification of physical or psychological signs or symptoms, or
induction of injury or disease, with identified deceptionB. The individual presents himself to others as ill, impaired, or injured
C. The deceptive behaviour is evident even in the absence of obvious external rewards
Factitious disorder imposed on another (previously factitious disorder by proxy, previous Munchausen-by-proxy)
A. Falsification of physical or psychological signs or symptoms, or induction of injury or disease, in another, with identified deception
B. The individual presents another individual (victim) to others as ill, impaired, or injured
C. The deceptive behaviour is evident even in the absence of obvious external rewards
factitious disorder
Previously “Munchausen Syndrome”
Pseudologia fantastica: pathological lying about symptoms/history
Patients are not just acting sick, they actively make themselves sick
Anti-coagulants, poison, psychoactive medication
Iatrogenic (caused by treatment) symptoms such as
opioid addiction or scar tissue from surgery
Prevalence very low in the general population, and even in hospital settings only about 1%
factitious disorder imposed on another
Victim is usually a child, but could be anyone under the care of the patient
Can occur by Internet (recognized as early as 1998)
There are many cases of parents being arrested for child abuse, in which Munchausen-by-proxy is raised as a possible
explanation
malingering
V-code (not a mental illness, but may be the focus of clinical attention)
Intentionally faking illness, psychological problems, or cognitive difficulties for material gain
Insurance, disability, legal proceedings, military service, jail, abuse, athletes playing contact sports
Diagnosis is based on reports of highly unlikely symptoms, inconsistency between behaviour and reports, and abnormal performance on tests
Patients generally do not have expert knowledge of psychopathology
Mild traumatic brain injury is associated with worse cognitive performance of neuropsychological tests than moderate traumatic brain injury
Self report and cognitive tests