Operative 4 midterm
1/76
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
77 Terms
glass ionomer
Which of the following materials has the closest coefficient of thermal expansion to tooth?
glass ionomer
amalgam
composite
utility wax
resin modified glass ionomers
Which restorative materials show higher amount of fluoride release after placement?
1,2,3,4,5
Which of the following are expected in rampant caries control by interim restoration?
1) Increase in patient's self-confidence and motivation
2) Improved prognosis accuracy
3) Improved periodontal health
4) Increased chance for saving pulp vitality
5) Establishing a medical model for the dental treatment
6) Decreased overall cost-effectiveness of care to the patient
improved depth of cure in the abcense of light
Addition of resin to conventional glass ionomer to create RMGI aimed to do the following EXCEPT
Improved mechanical properties
Improved esthetics
Improved depth of cure in the absence of light (self curing)
Improved surface characteristics and polishability
true
T/F Fluoride release from restoratives slows down but does not completely inhibit formation of new caries
true
T/F The acid-base reaction in resin-modified glass ionomer limits the working time after capsule activation, even if ambient light is controlled.
true
Composites in general have a clear advantage over RMGIs (resin modified class ionomer) in terms of esthetics, surface smoothness and luster.
false
T/F Dry finishing and polishing using rotary instruments is recommended for RMGIs to improve their final surface properties.
false
T/F RMGI have high fracture strength and therefore are recommended as very thin layers on beveled enamel margins.
Fuji IX GP Powder-liquid (conventional GI hand mixed)
You are picking up supplies to provide atraumatic restorative technique (ART) by placing material without deep decay removal in a dental mission in a remote area, where there is no electricity available. Which of the following materials is the best choice?
Fuji II LC Capsule (RMGI)
Fuji IX GP Powder-Liquid (conventional GI hand mixed)
Self-cured Composite Resin
Fuji II LC Powder-Liquid (RMGI)
false
T/F After PAA (poly acrylic acid) etching, the dentin surface must be fully desiccated and dried for insertion of the RMGI, since RMGI needs a completely dried surface.
SDF (38%)> Varnish> Rx Toothpaste
what is the correct order of fluoride concentration in common professionally applied or prescription based fluoride products? (SDF, Rx toothpaste, and varnish)
b
Which statement applies to modified class II (slot) preparations for direct
restoration?
A) The saucer-shaped interproximal preparations present a similar retention form to that of traditional class II restorations
B) Slot preparations preserve significant amount of occlusal tooth structure compared to traditional preparations
C) Saucer-shape preparation is suitable for both composite and amalgam
D) Slot preparations are indicated for advanced occlusal caries
box-shaped
Internal line angles and walls are typically defined for ___________ slot
preparations.
false
T/F Literature typically reports significantly better longevity for traditional composite preparations than slot preparations when indicated.
C
Which of the following is a good indication for a slot preparation on a premolar?
A) Interproximal advanced caries and occlusal moderate caries
B) Interproximal moderate caries and occlusal moderate caries
C) Interproximal moderate caries and occlusal sound structure
D) Interproximal initial arrested caries and occlusal initial caries
RGMI restorative (fuji II LC)
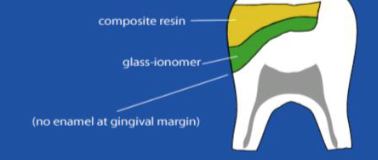
Which of the following materials is more suitable as the "base" on the gingival margin in an opensandwich technique restoration?
GI liner (e.g. Fuji Liner)
RMGI restorative (e.g. Fuji II LC)
RMGI luting cement (e.g Relyx Luting)
All of the above
amalgam preps usually have retentive groove
One of the main differences between composite and amalgam slot preparation is:
Amalgam preps usually have a pulpal floor
Composite preps usually have a pulpal floor
Amalgam preps usually have a retentive groove
Composite preps usually have a retentive groove
B
The following clinical situations is more likely to result in the development of "seconadary caries":
A) Open occlusal margins of composite in a low caries risk patient
B) Composite with defective interproximal gingival margin in a high caries risk patient
C) Biofilm accumulation over the occlusal surface of an unrestored tooth
D) All of the above
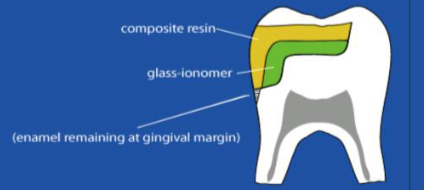
closed sandwhich technique
An interproximal advanced carious lesion with thin layer of affected dentin left to prevent pulpal exposure has a good quality sound gingival enamel at the proximal box. Which of the following restorativetechniques would be more suitable?
Open sandwich technique
Closed sandwich technique
Bulkfill composite technique
Direct pulp capping with SDF
C
The saucer-shaped slot preparations:
A) have sharp internal line angles
B) are indicated for both amalgam and composites
C) do not have well-defined internal line angles and are indicated for composites only
D) have increased retention form of the preparation compared to box-shaped slot preparations
occlusal enamel and tooth resistance preserved
The main advantage of slot preparations over traditional class II procedure is:
all of the above
The etiology of non-carious cervical lesions (NCCLs) has been attributed
to _____ .
Abrasion
Abfraction
Erosion
Endogenous mechanical stress
All of the above
all of the above
Which of the following should be considered when making a decision to
restore the abfraction lesions (NCCL)?
The cervical margin position
The integrity of the tooth as a result of tissue loss
Proximity of the defect to the pulp
Esthetic demands by the patient
All of the above
true
T/F The literature supports composite restoration of NCCLs with self-etch
adhesive and selective enamel etching as a viable and durable treatment
option.
black, green, red, yellow
Which order is correct for diamond burs band colors from coarser to finer?
true
T/F Microfractures in enamel as a result of a rough finish can result in white
lines around composite restorations.
all of the above
Which of the following are risks associated with procedures involved with
subgingival restorations?
periodontal issues as a result of restoration overhangs or open margins
soft tissue damage during finishing and polishing
periodontal tissue damage due to aggressive cord packing procedures
all of the above
false
T/F At the time of removal from gingival crest the cord should be as dry as
possible.
true
T/F It may become necessary to pack a second cord for various procedures
related to subgingival margins.
true
T/F The use of a modified matrix for proximal deep margin elevation can improve the gingival emergence profile and contour compared to no matrix use.
all of the above
Which of the following are clinical approaches suggested for adhesive restorations with deep proximal margins?
Local isolation with a retraction cord
Clinical crown lengthening (apical displacement of supporting tissues)
Rubber dam isolation and a modified matrix
All of the above or a combination of the approaches
1,2,3,4,5
What are the challenges associated with the use of conventional
techniques for adhesive restoration of a deep proximal margin?
1- Bonding may be difficult due to subgingival location and isolation
issues
2- If rubber dam is used, the rubber edge may cover the gingival margin
unless the septum is cut
3- Removal of the excess of restorative material or overhangs after setting
may be difficult
4- A conventional tofflemire matrix may not be able to establish sufficient
seal and/or anatomy
5- Vision may be limited due to margin location
6-The use of flowable composite is contraindicated for deep proximal
margins
primer, air dry, bond, air thin, light cure
What is the correct sequence of a two-step self-etching adhesive application (brand examples: (Optibond XTR or Clearfil SE Bond)?
1, 2, 4, 5, 6
An unfavorable proximal (too light or too tight) contact in a newly placed
MOD composite restoration could result from
1- Incorrect shaping or wedging of the matrix
2- Insufficient manipulation of the composite before curing
3- The choice of all-in-one (universal) or two-step self-etching bonding
systems
4- Over finishing or over polishing of the contact with burs, soflex discs or
polishing strips
5- Incorrect choice of matrix and wedge
6-Incorrect anatomy; a marginal ridge built too high during placement and
excessively reduced during occlusal adjustment
7-Sharp internal line angles of the preparation
true
T/F The use of a modified Dixieland Band matrix for proximal deep margin
elevation can improve the gingival emergence profile and contour
compared to no matrix use or regular tofflemire .
1,2,3,4
Which of the following principles apply in cavity preparation for amalgam
restorations?
1- Caries removal
2- Enamel finish
3- Retention form
4- Cleaning the cavity before insertion
D
Which statement is false about self-threading parapulpal retention pins
(TMS pins)?
A) Pins may result in dentinal micro fractures or crazing that can develop into catastrophic fractures
B) Pins have little or no contribution to fracture resistance
C) Micro leakage may increase around pins.
D) The reference literature recommends routine pin placement when the
retention form can not be established for composites
wedge should normally be placed fron lingual/palatal
The Toffelmire retainer is placed with the holder in the buccal of a Class II
MO preparation on an upper first molar. Which of the following statements
apply?
wedge should normally be placed from the buccal.
wedge should normally be placed from the lingual/palatal.
gingival edge of the matrix should be coronal to the gingival
cavosurface.
All of the above
0.5, 2,2, 0.5
The TMS self threading pins should typically be placed at least ____ mm
away from DEJ _____ into dentin, have ____ mm into amalgam and ____
mm clearance from adjacent walls
to relocate deep subgingival margins supragingival/equigingival
What is the primary purpose of the deep margin elevation technique in restorative dentistry?
flowable composite
which material is most commonly used for deep magin elevation?
better isolation, control and margin quality
What is a key advantages of the deep margin elevation technique?
in a thin layer cured separately
In the deep margin elevation technique, the flowable composite is typically applied:
In a single bulk layer to fill the whole preparation
In a thin layer cured separately
Only on the buccal aspect of the tooth
Without light curing
c
Which of the following statements about deep margin elevation is correct?
A) It is only suitable for anterior teeth
B) It eliminates the need for periodontal surgery in all cases
C) It can facilitate restoration procedures by improving margin accessibility
D) It is contraindicated in cases with periodontal recession
1,2,3,4,5
The following factors need to be considered in treatment planning for a
fractured cusp.
1) Occlusion
2) Additional cracks in the tooth
3) Pulpal status of the tooth
4) Periodontal status of the tooth
5) Patient preferences and resources
false
T/F Finite element analysis and experimental data confirm that cuspal strain
under occlusal stress in a maxillary premolar with a standard MOD
preparation significantly improves with insertion of amalgam because of
high strength of the alloy.
true
T/F Finite element analysis and experimental data confirm that fracture
resistance of a posterior tooth with a standard MOD preparation improves
with a bonded composite restoration.
phosphoric acid etch, rinse, primer, bond, light cure
In a 3-step bonding system known as the 4th generation bonding,
what are the main steps?
1,2, 3,6
The treatment plan for the fractured first premolar is to remove the
amalgam and restore with direct composite. Patient has normal symmetric
occlusion Reduction of the remaining cusp in this case ______ .
1) could enhance the fracture resistance of the restored tooth
2) could distribute the stresses more evenly on the restored structure
3) is recommended to follow cusp anatomy to create 2.5 - 3.0 mm thick
composite
4) is contraindicated in the most recent literature
5) is recommended as a thin 0.5 mm flat surface from the cusp tip
6) could improve retention by increasing the bonded surface area

secondary caries
what is the main reason dentist give for replacing fillings?
true
T/F Ditching and staining around amalgams and staining around
composites are all POOR predictors of active secondary caries.
gingival margins of class II-class V restorations
where is the most common location for recurrent caries
marginal sealing
best solution for preventing secondary caries
closed sandwhich
what is this technique called
open sandwhich
what is this techniwue called
true
T/F A slot preparation does NOT have a pulpal floor in its internal form
abrasion
Cause: Mechanical wear (toothbrush habit)
Affects: Teeth in groups (often unilateral)
Treatment: Composite (hybrid or flowable)
abfraction
Cause: Stress corrosion (occlusion related)
Affects: Single teeth (often upper premolars first)
Treatment: Composite (hybrid or flowable), Light-cured GIC
erosion
Cause: Chemical erosion (gastric causes)
Affects: Teeth in groups (lingual upper/buccal lowers)
Treatment: Composite (hybrid or flowable)
basic erosive wear examinaton (BEWE)
simple, quick index for screening a patient’s erosion status. The mouth is divided into six distinct areas to evaluate, using the criteria for sextant scores from 0 to 3, and the surface with the highest score is recorded for each sextant
1
BEWE score for initial loss of surface texture
2 (dentin)
BEWE score for distinct defect; hard tissue loss involving <50% of surface arrrea
3 (dentin)
BEWE score for hard tissue loss involving ≥50% of surface area
≥14
what would be considered a HIGH BEWE score
BEWE score ≥14
when would restorations requiring tissue removal be considered for non carious lesions
true
T/F a magin elevation matrix WILL give you the best gingival adaption and contour for the deep margin areas
all of the above
which of the following are reasons why ANTERIOR COMPOSITES might be done instead of crown/veneer?
patient acceptance/cost
immediate results and patient satisfaction
lack of tooth removal
easy to repair and maintain
all of the above
clean and dry surface
what should be done PRIOR to checking for carious lesions?
glass ionomer and resin modified glass ionomer
release fluoride, physically and chemically bond to tooth structure with NO NEED for etch and prime
true
T/F fluoride released by GI has tangible benifits against acid attack in adjacent enamel
true
T/F ADHESIVE restorative materials (ex: resin or bonded ceramic inlays) promote REDUCTION in STRAIN values in comparison to amalgam restorations
5000 ppm fluoride toothpaste/gel
what has the strongest evidence of effectiveness in nonsurgical treatment of carious lesion
once a year
how often should SDF be applied to be effective
glass particle (base)
what is responsible for fluoride release from resin modified GI
true
T/F Amalgam does NOT reinforce an MOD restoration against fracture
2.5mm
what is the minimum REDUCTION THICKNESS of a adhesive cusp coverage restoration