Exam 3 - Aphasia Classifications + Assess./Remediation
1/87
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
88 Terms
Arousal
Continuum in state of consciousness/awareness
Attention
Continuum in ability to focus consciousness/awareness
Perception
Recog. of relevant dimension of sensory stimuli
Memory
Ability to store/retrieve info over varying time periods
Reasoning
Ability to draw conclusions through logical thinking
Neurological basis of Speech, Lg, Cog.
Arousal
Attention
Perception
Memory
Reasoning
Listening/Aud comprehension
Area #40, 49; Hearing + understanding message
Speaking/Expressive lg.
Retrieve concept idea + aud. image/word
Connect circuit
Program message + word
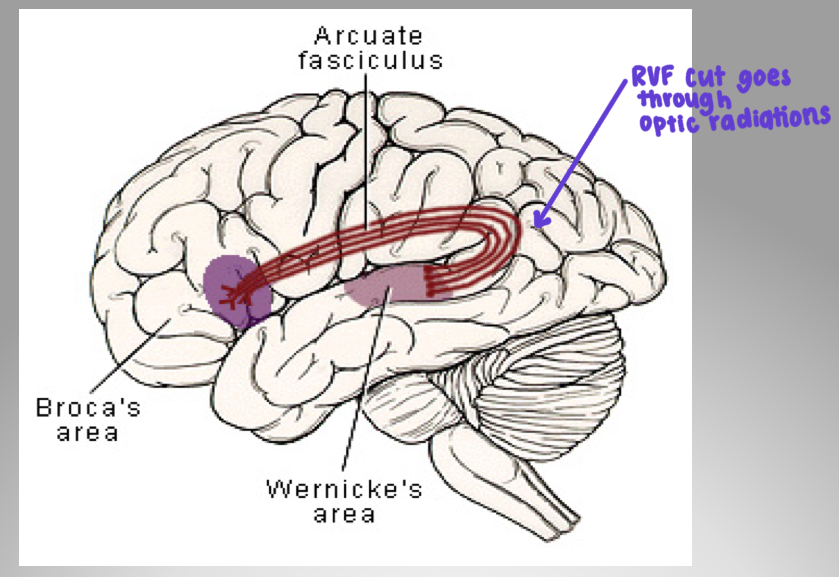
Neuro-Ling. Model
Listening/Aud comprehension
Speaking/expressive lg.
Speech circuit
Aphasia
Verbal comm + multi-modal disorder caused by cerebral damage
2 Major Aphasia approaches
Unidimensional
Multidimensional
Unidimensional Approach
1 lg. component
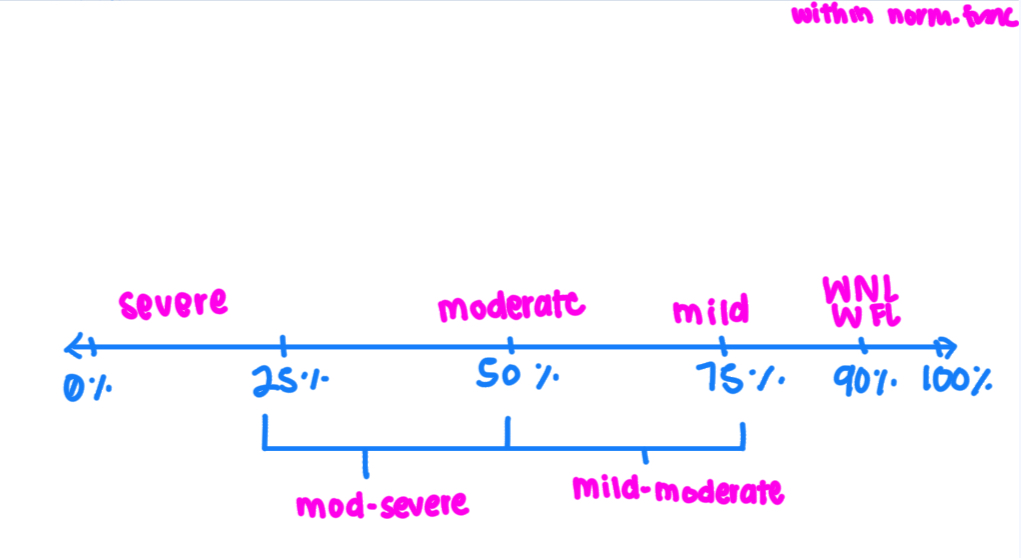
Degree of severity
1 therapy type
Multidimensional Approach
Multiple lg. components
Dependent on lesion’s size + location
Diff methods required for diff aphasia types
Alt. Approaches
Holistic
Localizationist
Connectionistic
Expressive aphasia
Damage anteriorly (#44) / Broca’s
Non fluent
Verbal difficultly
Struggles + hesitancies
Receptive aphasia
Posterior lesions / Wernicke’s
Fluent
String of words
Comprehension problems
Broca’s aphasia #44: Comprehension
Better reception, but not normal
Predominantly expressive
Upper ½ of comprehension
Broca’s aphasia #44: Nonfluent
Slower programming
Affected, effortful stop + start
Short sentences
Broca’s aphasia #44: AOS
Slow initiation
Slow rate
Phoneme selection problems
Poor transitions
Broca’s aphasia #44: Agrammatism
Telegraphic speech
Economy of effort
Broca’s aphasia #44: Reading/Writing
Mirrors oral lg./speech
Writing least used lg. modalities (and developed last)
Reading is a translation from visual to aud modality
Broca’s aphasia #44: Poor repetition
Better imitative behavior
Apraxia shows with command + imitations
Real objects improve naming
Broca’s aphasia: Associated problems
Emotions - depression
Motor - #4 unilateral lesion, arm paralysis
No visual problems
Oral apraxia #44
Limb apraxia #6
Wernicke’s aphasia #22: Description
Secondary association area
Linked more to sensory
Incoming aud stimuli linked to other brain areas
Wernicke’s aphasia: Funcs.
Fluent, not normal
Poor comprehension
Poor reading, writing
60+ yrs old
Area #22: Aud. Verbal Comprehension
Integrated activity of many brain areas
Semantic problem - can’t attach meaning to what they hear (not a perception problem)
Area #22: Aud. Image Retrieval
Aka word retrieval problem
Normal motor skills; fluent sentence length
Inability to recall previous aud. experience (object/person name)
Aud. pattern
When they can’t think of a word, they tell about it
Word/Aud. Image retrieval problems
Circumlocution
Empty speech
Semantic paraphasia
Phonemic paraphasia
Neologism
Jargon(ism)
Circumlocution
Talking about/around a word; Legitimate words used, but never gets to the point
Empty speech
General words that don’t comm. info
Semantic paraphasia
Substituting word in same semantic category
Phonemic paraphasia
Substituting word that resembles target word but not part of our lg.
Neologism
Random/made-up word that doesn’t resemble target word
Jargon(ism)
Continuous sentences/stretches of neologisms
Area #22: Aud. Guidance/Self-monitoring
Compromise area = speech cannot be regulated
Unable to self-correct
Wernicke’s aphasia #22: Associated Issues
No hemiplegia
Unrealistically happy/euphoric (unaware they don’t make sense)
Become belligerent, can tell things are wrong as they progress
Conduction aphasia
Arcuate fasciculus + forwarding aud. image damage
Less severe Wernicke’s, intact comprehension
Problem: organizing output
Conduction aphasia: Funcs.
Good comprehension
Fluent
No AOSS
Difficult repetition
Conduction aphasia: Associated symptoms
No hemiplegia
Some bilateral limb apraxia (no hemiplegia to mask it)
RVF deficit in both eyes
Optic radiations run deep into cortext
Global aphasia
Deep lesion in MCA
Damage to Wernicke’s, Broca’s, AF
Impairment across all modalities
Global aphasia: Funcs.
Poor comprehension
Severely non-fluent
Poor repetition
Poor reading, writing
Concept of what they want to say
Good non-verbal pragmatics
Transcortical motor aphasia
Broca’s area cut off at prefrontal cortex
Ok motor programming, but cut off from motivation/desire to talk
No AOS
Nonfluent
Intact comprehension
Perfect repetition
Transcortical sensory aphasia
Wernicke’s area cut off from cortex except speech circuit
Lesion borders region supplied by MCA + PCA
Speech fluent, similar to Wernicke’s
Poor comprehension
Excellent repetition
Transcortical mixed aphasia
Nonfluent (limited verbalizations, paraphasia, anomic)
Poor comprehension
Good repetition (Echolalic, but not perfect)
Primary progressive aphasia (PPA)
Not specific diagnosed trauma
Associated w progressive illness/dementia
Gradual loss of ability to name objects
Anomic aphasia #39: Funcs.
Good comprehension
Fluent
No neologisms
Few paraphasias
Circumlocutions mostly
No AOS
Good repetition
Poor naming word finding in isolation
Poor cross modal funcs (reading + writing)
Nonfluent aphasias
Broca’s
Global
Transcortical motor
Transcortical mixed
Fluent aphasias
Wernicke’s
Conduction
Anomic
Transcortical sensory
Nonfluent, Good Comp.
Broca’s
Transcortical motor
Nonfluent, Bad Comp.
Global
Transcortical mixed
Nonfluent, Good Comp., +Rep
Transcortical motor
Nonfluent, Good Comp., -Rep
Broca’s
Nonfluent, Bad Comp., +Rep
Transcortical mixed
Nonfluent, Bad Comp., -Rep
Global
Fluent, Good Comp.
Conduction
Anomic
Fluent, Good Comp., +Rep
Anomic
Fluent, Good Comp., -Rep
Conduction
Fluent, Bad Comp.
Wernicke’s
Transcortical sensory
Fluent, Bad Comp., +Rep
Transcortical sensory
Fluent, Bad Comp., -Rep
Wernicke’s
Basic skills in assessment
Fluency
Aud. Comprehension
Repetition
Naming
Basic skills in assessment: Fluency
Spontaneous, pic description
Speech rate
Utter length
Artic. ease
Basic skills in assessment: Aud. Comprehension
Single words
Commands
Paragraph length info
Basic skills in assessment: Repetition
Word
Sentence
Basic skills in assessment: Naming
Confrontation
Responsive
Prognosis depends on…
Age of onset (the younger the better)
Location/lesion size
Time post onset
Overall health
Single vs mult. lesions (mult. strokes = poorer)
Emotional well-being
Undetermined factors
Purpose of assessment
Diagnosis of presence/syndrome
Determine performance level + change
Assess assets/liabilities
Assessment areas
Receptive lg.
Expressive lg.
Reading
Writing
Cog.
Assessment areas: Receptive lg.
Isolated words (pointing tasks)
Connected lg. (commands, y/n q’s, complex)
Assessment areas: Expressive lg.
Naming
Obj., confrontational w time, sentence completion
Repetition
Phon., words, phrases, sentences
Fluency
Convo speech, story retell, pic description, procedural discourse
Assessment areas: Reading/Writing
Testing a patient’s:
Letters
Words, phrases, sentences
Simple + complex paragraphs
Functional
Assessment areas: Cognition
Testing patient’s:
LTM - personal q’s, y/n tasks, delayed recall
STM - digit/sentence/word repetition, commands
Executive func. - generate/plan/monitor goals, problem solving
Attention - focused, divided?
Western Aphasia Battery
Tests:
*Reading/writing on separate test
Spontaneous speech - convo, pic description
Aud. Verbal comp. - y/n q’s, aud word recog., sequential commands
Repetition
Name/word finding - obj naming, word fluency, sentence completion, responsive
Boston Diagnostic Aphasia Examination (BDAE)
Created by Goodglass + Kaplan; 3 goals:
Diagnosis of presence/syndrome
Measurement of performance level for baseline
Assets/liabilities as therapy guide
BDAE 5 major sections
Tests:
Convo speech
Aud. Comp.
Oral expression
Understanding written lg.
Writing (includes reading/writing, not separate)
BDAE interpretations
Severity rating scale analysis
Rating scale profile of speech characteristics
Subtest/modalities performance patterns
BDAE strengths
Comprehensive
Includes reading, writing, oral apraxia as main body of test
Standardized
Scales for measuring qual. speech output
For neuropsych/neurologists
Other formal assessments
Boston Naming test
CADL
MTDDA
Burns Right Hemisphere
Apraxia Battery
MIT
AAC
Cog. Ling. Quick test
Informal assessments
Lg. Sample
Vocabulary
Topic maintenance (prag.)
Fluency
Suprasegmentals (intonation, prosody)
Paraphasias, neologisms
Voice qual.
Breath support
O/M func.
Hearing
Key Remediation Principles
Direct to person’s (dis)abilities
Struct. therapy programs
Provide feedback
Show progress
Direct therapy to “key” deficit areas
Direct treatment approach
Stimulus-Response-Consequence; Focused on specific lg. process
Indirect treatment approach
Unstructured, conversational (prag., word-finding)
Treatment hierarchies
Length + complexity
Cuing levels
Items
Treatment hierarchies: Length + complexity
Simple → complex
Concrete (literal) → Ideas (abstract)
Treatment hierarchies: Cuing levels
Verbal, visual, tactile
Treatment hierarchies: Items
Expressive + receptive
Struct. Evidence Based Treatment Protocols
Semantic Feature Analysis
Verbal Network Strengthening Treatment for Aphasia
Phonomotor therapy
Rosenbeck’s 8 Step Continuum of Apraxia
MIT
Setting for Assessment/Remediation
Functional
3-5 sessions/wk depending on severity + needs
30-60min sessions
Warm up, introduce new tasks, cool down
Timing (find good time for therapy)
Plan for progression (where do I want them to be before discharge?)