Inflammation, OA/RA/SLE, Osteoporosis
1/88
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
89 Terms
Describe inflammation
Inflammation is a nonspecific, generalized response to stress/harmful stimuli to dilute or neutralize the inflammatory agent, remove damaged tissue, and set up a suitable environment for healing and repair
Think about inflammation like broad-spectrum abx (it kills both good and bad bacteria; inflamnmation can be harmful or helpful)
Does infection alway have inflammation?
Yes, but inflammation does not always mean there is an infection.
Someone can come in with increased WBC, but no infection (inflammation causes leukocytosis)
Chronic, progressive, metabolic bone disease marked by:
Low bone mass
Deterioration of bone tissue
This leads to increased bone fragility and instability to withstand normal mechanical stress
Osteoporosis
4 main things in diet to maintain bone health
Vitamin D
Calcium
Phosphorus
Protein
Factors that increase risk for osteoporosis
Hormone imbalances (hyperthyroidism/hyperparathyroidism, low estrogen/menopause)
Inadequate dietary intake (CPPD)
Medications (steroids, antiseizure/psych meds, Rolaids)
SAD
Complications of chronic inflammation
Tissue damage
Endothelial damage
Increased r/o clots
Immunocompromised
Exhausted metabolism
Pathophysiology of osteoporosis
Bone resportion exceeds bone formation
Decreased osteoclast apoptosis
Increased osteoclast development
Osteopenia (reduced bone density) comes before osteoporosis
S&S of osteoporosis
“Silent disease”; can progress and deteriorate bone thoroughly before a fracture occurs
Spontaneous fractures (fracture when you sit down, or just walking)
Increased r/o fractures
Back pain
Generalized body pain
Kyphosis (inward curvature/humpback)
Loss of height
Modifiable and nonmodifiable risk factors for osteoporosis
Modifiable
Diet (CPPD)
Sunlight, food
Activity level (weightbearing)
Swimming and cycling are NOT weightbearing
SAD
Meds (Tums are good, Rolaids bad)
Low body weight
Nonmodifiable
Age 65+ (post menopausal for women (low estrogen);
Caucasian or Asian identiy
Family hx
Female
Estrogen deficiency/low testosterone (post-menopausal)
Malabsorption diseases)
Hysterectomy
Why are females more at risk for osteoporosis than male patients?
Pregnancy and/or breastfeeding (decreases calcium levels)
Have lower bone density
Bone resorption is more rapid after menopause (decreased estrogen protection)
Why is estrogen important for preventing osteoporosis?
Estrogen inhibits bone resorption
Diagnostics for osteoporosis
Bone mineral density (BMD) → DEXA
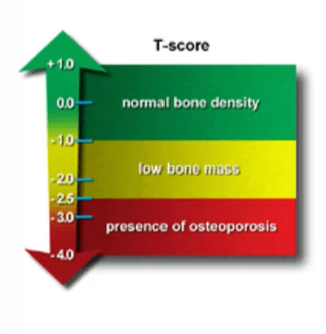
T-scores (higher T score = increased r/o osteoporosis or active condition)
X-rays (if you can see osteoporosis on X-ray, condition is already late stage w/ 25-40% bone density loss)
Nutrition assessment (calcium and vitamin D)
T-scores (osteoporosis)
1 to -0.99 = normal bone density
-1 to -2.4 = Low bone density
>-2.5 = osteoporosis
Drug therapy for osteoporosis
Biphosphonates (the -nates)
Alendronate, risedronate, pamidronate)
Calcium supplements
Vitamin D supplements
MOA of biphosphonates
Diminishes and interferes with osteoclast activity (reduce bone resorption)
Patient education:
Take w/ full glass of water and sit up for at least 30 min to an hr after taking
Why take biphosphonates w/ full glass of water (30 mins before other meds and food) and sit up for at least 30 min to an hr after taking
Biphosphonates cause significant esophageal irritation (if you lay down, you will have acid reflux)
Nursing implications for biphosphonates
Take w/ full glass of water and sit up for 30 min to an hr (med causes severe esophageal irritation)
Take 30 mins before other meds and food
Lockjaw necrosis = educate patient to alert nurse if they feel jaw tenderness, clicking, S&S of inection
Key sources of calcium
Dairy (milk, yogurt, cheese)
Leafy greens (spinach, collards, kale)
Legumes
OJ + fortified cereal
Key sources of vitamin D
Fatty fish (cod, salmon, carp, seal, mackerel, trout, tuna)
Fortified dairy
Eggs
OJ and cereal
Osteoporosis is a normal part of aging. True or false?
False. It’s normal to have some bone loss, but osteoporosis is porous bones, which is abnormal.
The different types of arthritis
OA
RA
Fibromyalgia (FMS)
SLE
Gout
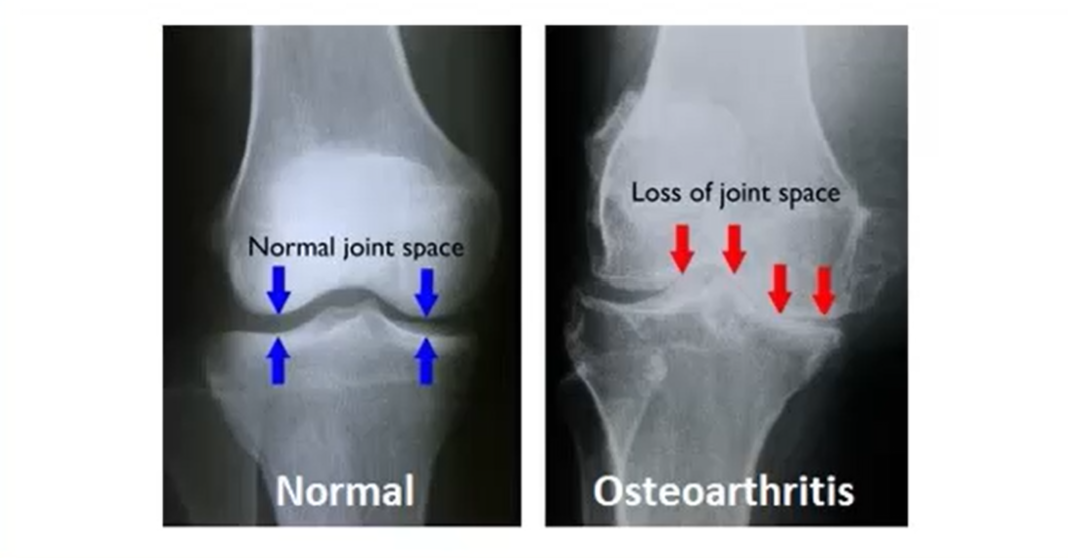
Gradual loss and integrity of articular cartilage (padding that covers bones and joints)
OA
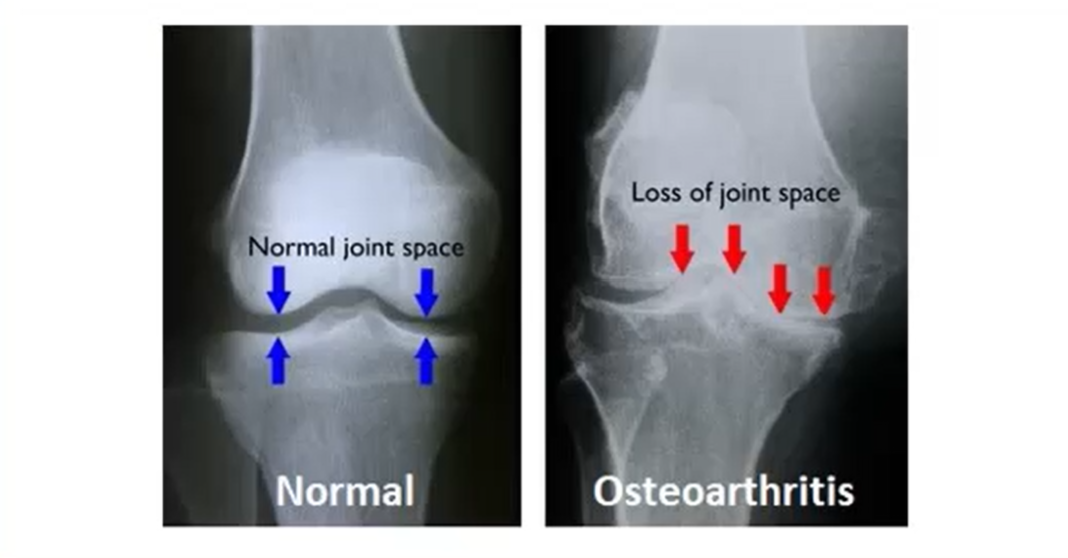
Pathophysiology of OA
1) Loss or damage of articular cartilage (e.g. mechanical stress/injury)
2) New bone formation in joint margins (remodeled bone is more cracked and not as smooth)
3) Narrowing of joint margins & bone spurs (articular cartilage flakes off from frictuion, may leave completely exposed bone; bones rubbing against each other causes uneven grooves and bone spurs)
4) Mild synovitis (bone spurs enter synovial fluid causing inflammation)
5) Thickening of joint capsule (decreased ROM)
Secondary osteoporosis is caused by
Hormone imbalances (hyperparathyroidism, hyperthyroidism, diabetes), medications (heparin, steroids, phenytoin, barbiturates, lithium, aluminum, steroids, phenytoin, barbiturates, lithium, aluminum, antacids [Rolaids], SAD
Degeneration, eventual loss, and then disordered repair of recartilage. Increased remodeling = not as smooth or frictionless; loses glistening appearance and yellows.
OA
Areas at high r/o suffering from OA
Hips
Knees
Shoulders
Hands
S&S of OA
Joint stiffness
More common after periods of disuse
Joint pain
Pain worsens with joint use
Swelling (depends on stage)
Joint effusion
Crepitus
Bouchard nodes/Herberden nodes
Modifiable risk factors
Obesity
Repetitive movement/mechanical stress
Injury
Medications
Non-modifiable risk factors
Increased age
Female
Decreased estrogen
Drug therapy for OA
NSAIDs
Topical agents
Celebrex
Steroid injections for flare-ups
Alternative medicine
Acupuncture
Massage
Yoga
Anti-inflammatory supplements
Heat therapy vs cold therapy in OA (heat vs cold compress)
Do whatever makes patient happy
Heat for muscle pain and joint stiffness (vasodilation)
Cold for inflammation and associated swelling (vasoconstriction)
Chronic, systemic, autoimmune disease characterized by inflammation of connective tissue in the synovial joints
Characterized by periods of remission and exacerbation
RA
Autoimmune diseases are characterized by inflammation, which leads to
Generalized fatigue, lethargy
Pathophysiology of RA
1) Antigen (whatever it may be) triggers IgG and autoantibodies (AKA rheumatoid factor (RF))
2) IgG and autoantibodies combine to create immune complexes
3) Complexes deposit in synovial areas of the body resulting in inflammatory reaction (body attacks joints)
4) Inflammation keeps going on and, on cytokines and enzymes destroy healthy tissue long-term
S&S of rheumatoid arthritis
Nonspecific manifestations
Fatigue, lethargy, body ache
Joint stiffness (typically smally joints of hands and feet)
Pain, stiffness, limited ROM
Occur systemically (small joints of hands, PIP, MCP, and feet MTP)
Joint stiffness after inactivity
Ulnar drift and swan-neck deformity
RA nodes
Morning stiffness last 60 min+
Bilateral/symmetrical (if RA on one hand, there will be RA on other hand)
As it progresses, inflammation and fibrosis cause deformity
Nonspecific manifestations
Fatigue, lethargy, body ache
Joint stiffness (typically smally joints of hands and feet)
Pain, stiffness, limited ROM
Occur systemically (small joints of hands, PIP, MCP, and feet MTP)
Joint stiffness after inactivity
Ulnar drift and swan-neck deformity
RA nodes
Morning stiffness last 60 min+
Bilateral/symmetrical (if RA on one hand, there will be RA on other hand)
As it progresses, inflammation and fibrosis cause deformity
These clinical manifestations appear in what condition?
RA
Extra-articular symptoms of RA
Cardiac: artherosclerosis, MI, stroke, vascular lesions (rheumatoid nodules), pericarditis, myocarditis, Raynaud’s, peripheral edema
Respiratory: rheumatoid nodules, fibrosis, pleuritis
HEENT: Sjorgren’s syndrome, conjunctivitis
Skin: rheumatoid nodules, butterfly rash (but it’s mostly lupus)
Immunology: immunocomprimised, Felty syndrome
Modifiable risk factors for RA
Smoking
Obesity
Non-modifiable risk factors for RA
Age 30-60
Female
Family hx/genetics
Cardiac symptoms of RA
Artherosclerosis, MI, stroke, vascular lesions (rheumatoid nodules), pericarditis, myocarditis, Raynaud’s, peripheral edema
Respiratory symptoms of RA
Rheumatoid nodules, fibrosis, pleuritis
HEENT symptoms of RA
Sjorgren’s syndrome, conjunctivitis
Skin symptoms of RA
Rheumatoid nodules, butterfly rash (butterfly rash mostly SLE)
Immunologic symptoms of RA
Immunocomprimised, Felty syndrome
A common autoimmune disease that targets moisture-producing exocrine gland (leads to symptoms such as dry eyes and dry mouth)
Xerostomia and keratoconjunctivitis sicca
Other glands in the stomach, pancreas, intestines
Increase risk for non-Hodgkin’s lymphoma
Usually diagnosed in ages 40s to 50s
Most patients are women
Sjogren’s syndrome
Primary Sjogren’s syndrome
No other rheumatic disease
Occurs in combination with another rheumatic disease (e.g. RA, SLE, scleroderma)
Autoimmune thyroid disorders are common
Etiology: genetic and evironmental
Genes: Whites, Japanese, Chinese, African Americans
Trigger: viral or bacterial infection adversely stimualtes immune system
Secondary Sjogren’s syndrome
Diagnostics for RA
H&P
RF (not found in all cases of RA)
Citrullinated peptide (anti-CCP)
C-reactive protein
Synovial fluid analysis
Drug therapy for RA
Disease-modifying antirheumatic drugs (DMARDs) → slow disease progression
Methotrexate
Antimalarial drugs
Hydroxychloroquine
Biologic response modifiers (BRMs)
Slow disease progession and 2nd-line after DMARDs)
NSAIDs
Steroid injections
Major AEs of methotrexate
Bone marrow suppression (monitor CBCs)
Nephrotoxicity and stomatitis (monitor kidney function and mouth)
Nursing management for RA
Pain (NSAIDs & steroids)
Mental health
R/o infection (immunocompromised)
R/o multiorgan involvement
ADLs
Modifiable risk factors for osteoporosis
Diet (CPPD)
Sunlight, food
Activity level (weightbearing)
Swimming and cycling are NOT weightbearing
SAD
Meds (Tums are good, Rolaids bad)
Low body weight
Nonmodifiable risk factors for osteoporosis
Age 65+ (post menopausal for women (low estrogen);
Caucasian or Asian identiy
Family hx
Female
Estrogen deficiency/low testosterone (post-menopausal)
Malabsorption diseases)
Hysterectomy
RA vs OA
RA = symmetric, morning stiffness > 30 min.
Patho: joints in hands more PIP, NOT DIP; expected course of worsening (delay progession but incurable). General symptoms like fever, malaise.
Inflammaiton around joint capsule; swollen inflammed synovial membrane
OA = asymmetric, morning stiffness < 30 min.
Patho = joints in hands (DIP & PIP); random exacerbations.
Bone on bone violence
What can exacerbate/cause flares of RA?
Triggers such as stress or other precipitating events
Multisystem inflammatory autoimmune disease
Chronic, unpredicatble course with alternating periods of remission and exacerbation
Stress (e.g. puberty, pregnancy) can precipitate this disease
Sunlight can also cause this disease to flare
SLE
Pathophysiology of SLE
Trigger
Autoantibodies are created against nucleic acids and erythrocytes, coagulation proteins, phospholipids, lymphocytes, platelets, and more
Has periods of remission and exacerbation
Deposition of circulating immune complexes (esp in organs); body attacks itself with inflammation
These complexes have a tendency to deposit in glomerular basement membrane (cause kidney damage)
Complementary and inflammatory activation that is never-ending
What to monitor for SLE
Triggers (e.g. sun exposure)
Kidney function, hydration, urine output, I/Os
Immunocomprimised → CBC
Integumentary symptoms of SLE
Alopecia
Photosensitivity
Butterfly rash
Discoid erythema
Palmar erythema
Mucosal ulcers
Cardiopulmonary symptoms of SLE
Endocarditis
Myocarditis
Pericarditis
Pleural effusion
Pneumonitis
Raynaud’s
Urinary symptoms of SLE
GN (Good Pasture’s syndrome)
Hematuria
Proteinuria
Neurologic symptoms of SLE
Stroke
Seizures
Peripheral neuropathy
Psychosis
Cognitive impairment
Hematologic symptoms of SLE
Anemia
Leukopenia
Lymphadoenopathy
Splenomegaly
Thrombocytopenia
GI symptoms of SLE
Abd pain
NVD
Dysphagia
Musculoskeletal symptoms of SLE
Arthritis
Myositis
Synovitis
Reproductive symptoms
Menstrual abnormalities
Very difficult to get pregnant
General symptoms of SLE
Respiratory
CV:
Raynuad’s, pericarditis, vascular inflammation
General:
Weight loss
Fatigue
Fever/immuncomprimised
Emotional lability
Hematologic disorders (anemia)
Neurologic disorders (seizure/stroke)
Photosensitivty + butterfly rash on cheeks
Erythematous rash to areas exposed to sunlight
Kidneys:
Lupus nephritis
Proteinuria and hematuria
Modifiable risk factors for SLE
Smoking
Stress
Medicaitons
Environmental factors
Air pollution, pesticides, heavy metal exposure
Non-modifiable risk factors for SLE
Female
Family hx/genetics
15-45 y/o
Ethnicity (everyone gets affected more except caucasians)
Diagnostic tests for SLE
No specific test
Anti-smith antibody (gold-standard)
Anti-nuclear antibody (ANA)
H&P
Inflammatory markers
Gold-standard test for SLE
Presencen of anti-smith antibody
Nursing management of SLE
Assess for flare-ups and triggers
Manage pain
Assess mental status
ADLs
Assess multiorgan involvement (especially kidneys)
Assess for clotting and bleeding (systemic inflammation can precipitate clots and bleeding_
Risk for infection
Drug therapy for SLE
Combination NSAIDs
Steroids (corticosteroids)
Immunosuppressants
Antimalarial drugs
Hydroxychloroquine and chloroquine
Methotrexate
AE of this drug toxicity is stomatitis; high doses (toxic effect/OD) can injure kidneys/nephrotoxicity; high doses cause bone marrow suppression
Methotrexate (used to treat RA)
Gold standard diagnostic test for osteoporosis
Dexa scan (measures bone density)
Dual energy x-ray absorptiometry
Home safety for osteoporosis and reducing r/o falls
Remove/tape down rugs
Grab bars
Assistive devices (cane)
Adherence to meds, exercise plan, supplements/diet
Nonslip socks or slippers
A person is classified as having SLE if 4 or more of the criteria are present, serially or simultaneously, during any interval of observation:
Antinuclear antibody (ANA): abnormal titer
Anti-smith
Discoid rash: raised patches with scaling follicular plugging; scarring in older lesions
Hematologic disorder: hemolytic anemia, leukopenia, lymphopenia, or thrombocytopenia
Immunologic disorder: anti-DNA antibody or antibody to Sm (Smith) nuclear antigen or positive antiphospholipid antibodies
Malar rash: fixed redness, flat or raised (butterfly rash)
Oral ulcers: usually painless
Neurologic disorder: seizures or psychosis (in the absence of causative drugs or known metabolic disorders)
Nonerosive arthritis: 2 or more peripheral joints with tenderness, swelling, effusion
Pleuritis or pericarditis
Photosensitivity
Renal disorder: persistent proteinuria, cellular casts in urine
Antinuclear antibody (ANA): abnormal titer
Anti-smith
Discoid rash: raised patches with scaling follicular plugging; scarring in older lesions
Hematologic disorder: hemolytic anemia, leukopenia, lymphopenia, or thrombocytopenia
Immunologic disorder: anti-DNA antibody or antibody to Sm (Smith) nuclear antigen or positive antiphospholipid antibodies
Malar rash: fixed redness, flat or raised (butterfly rash)
Oral ulcers: usually painless
Neurologic disorder: seizures or psychosis (in the absence of causative drugs or known metabolic disorders)
Nonerosive arthritis: 2 or more peripheral joints with tenderness, swelling, effusion
Pleuritis or pericarditis
Photosensitivity
Renal disorder: persistent proteinuria, cellular casts in urine
Diagnostic criteria for SLE (present serially or simultaneously during any interval of observation)
Nursing management for SLE
Infection prevention (drugs e.g. corticosteroids makes immune system weaker)
Rest/activity balance
Sun protection
Avoid triggers (stress, sun exposure, meds, infections)
Medication teaching
Manage pain
Control inflammation and protect organs
Pregnancy (some SLE meds are safe, but some like methotrexate have to be stopped)
Emotional support + positive coping
Metabolic arthritis caused by uric acid crystal deposition. Involves hyperuricemia from overproduction or underexcretion
Monosodium urate crystals form in joints
Crystals trigger inflammatory response → pain, swelling & redness
Gout
Clinical manifestations of gout
Sudden, severe joint pain that occurs at night
Redness, swelling, warmth on affected joints
Very sensitive to touch (guarding; don’t touch it)
Tophi (chronic gout); hard visible lumps of uric acid deposits
Commonly only affects one joint at a time (typically big toe)
Diagnostic tests for gout
Symptoms
Serum uric acid levels
Synovial fluid aspiration → gold standard
Renal function (kidney issues worsen gout)
Medications (e.g. HCTZ)
Gout drugs
Colchecine → acute gout attacks
Allupurinol/Febuxostat → long-term uric acid control (chronic gout; not used for acute attacks)
Nursing implications for xanthine oxidase inhibitors (allupurinol/febuxostat)
Take with meals
Stay well hydrated (3L of fluid/day)
Monitor kidney function and la
Agranulocytosis/aplastic anemia (bone marrow dysfunction)
Serious skin conditions (exfoliative dermatitis, SJS)
N/V
Dizziness, drowsiness
Kidney stones
Adverse effects of xanthine oxidase inhibitors
Foods high in purines (avoid in gout)
Shellfish
Red meat
Alcohol
Organ meats
Nursing management of gout
Drug therapy
Dietary changes (limit purine-rich foods)
Shellfish, red meat, organ meat, alcohol
Hydrate (esp if taking XOIs → 2-3 L/day)
Weight control
Nursing focus for gout
Hydrate (2-3 water L/day) → flush uric acid
Avoid (Avoid purine → ETOh, red meat, organ meat, shellfish)
Relieve (take long-term meds consistently e.g. XOIs allupurinol/feboxustat; take colchicine for acute attacks)