NUTR 202: Module 3
1/68
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
69 Terms
What is the general function of vitamins and minerals (as compared to macronutrients)?
Not energy yielding
Involved in metabolic processes
Assist in providing energy
Vitamins: Organic
Minerals: Inorganic
Be able to identify fat soluble vs. water soluble vitamins.
Fat soluble vitamins:
Storage in body
Longer periods of time
Larger amounts
Found in liver and fat cells
INCREASE likelihood of adverse effects or toxicity
Water soluble vitamins:
Storage in body
Short period of time
not generally stored in large quantities
DECREASED likelihood of toxicity, BUT INCREASED risk of deficiency
fat soluble vitamins
Vitamin A
Vitamin D
Vitamin E
Vitamin K
water soluble vitamins
Vitamin C
Thiamin
Riboflavin
Niacin
Biotin
Folate
What are the functions of Vitamin A?
Integrity of epithelial cells
Bone growth
Cell membrane stability
Gene Regulation
CELL DIFFERENTIATiON
Vision
Crucial to normal vision
Immune function
Disease resistance, particularly for children
Production of white blood cells
Occurs in 3 different forms:
Retinol (most active form)—> stored in liver
Retinal
Retinoic acid
Vitamins may be added to foods, but are not naturally present in food
Fortified
Vitamins may be lost during processing and added back to meet needs
Enrichment
What are the differences between preformed vitamin A and provitamin A?
Preformed vitamin A:
Ready to use
Found in animal-based or fortified foods
Provitamin A:
Converted to active form as needed
Ex: beta-carotene
Found in plant-based foods
Identify dietary sources of preformed vitamin A and provitamin A.
Preformed Vitamin A:
Fortified milk, cheese, cream, butter, eggs, liver
Provitamin A:
Green leafy vegetables, Orange and red produce, apricots, cantaloupe, carrots, sweet potatoes, and pumpkins
Describe deficiency and toxicity symptoms associated with vitamin A.
Early stages of deficiency:
Night blindness
Reversible
Short-term vitamin A deficiency:
The cornea becomes dry and damaged
Long-term vitamin A deficiency:
Xerophthalmia— which prevents the eyes from producing necessary tears, causing extreme dryness, damage to the cornea, and potential blindness.
Permanent loss of vision
Toxicity: (if stored in body for long periods of time)
Liver damage
Birth defect
Iron and Vitamin A deficiency may coexist
What is the role of vitamin D in calcium metabolism?
Stimulates cells of small intestine to produce calbindin
A calcium binding protein
INCREASES calcium absorption
Stimulates kidneys to conserve calcium
DECREASES urinary calcium excretion
Stimulates calcium release from bone to help maintain blood calcium levels
What are potential reasons for increased vitamin D needs in older adults?
Ability to convert Vitamin D into is active form DECREASES
Likelihood of adequate exposure to sunlight DECREASES
Identify dietary and non-dietary sources of vitamin D.
Dietary sources of vitamin D:
Cod liver oil
Sardines, salmon, shrimp
Liver
Mushrooms exposed to UV light
FORTIFIED foods provide MAJORITY of dietary vitamin D
Milk or margarine
Cereals
Juices
******NOT CHEESE AND YOGURT
Non-dietary sources:
Human body makes vitamin D w/ adequate exposure to sunlight through a series of steps
Cholesterol in skin combines w/ UV rays
Converted into precursor of vitamin D
Eventually makes its way to the kidneys
Converted to active form of D3
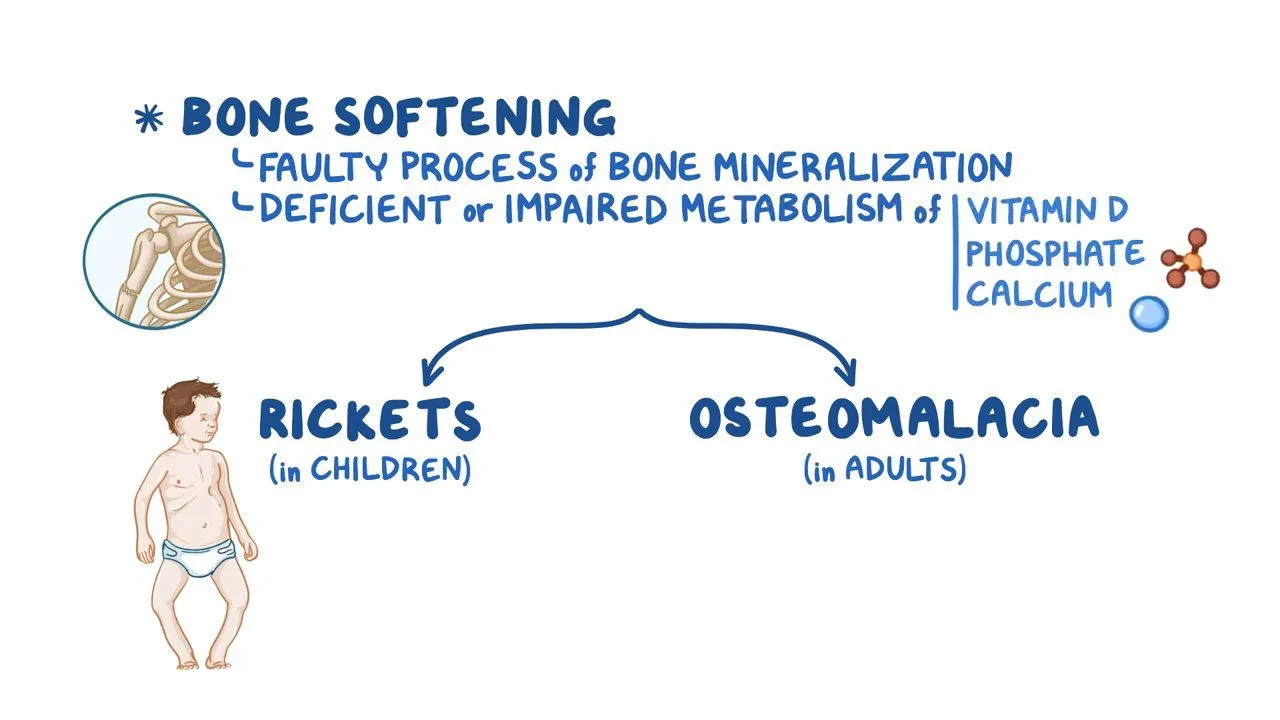
What chronic condition(s) is/are associated with insufficient vitamin D levels?
Children:
**Rickets
Disease characterized by softening and deformity of long bones
Inability to deposit calcium in newly formed bone
Malformation of the skull, ribcage, and ends of long bones
Adults:
**Osteomalacia
Softening of bone caused by decalcification
What population(s) is/are at risk of Vitamin D insufficiency?
Ethnic populations w/ dark skin
Land caucasian population
What are the primary functions of Vitamin E?
Acts as an **antioxidant
Neutralize free radicals that can damage cell membranes, DNA, proteins
Unstable compounds w/ unpaired electron that attack other molecules
Vitamin E donates electron to neutralize free radicals!!
Enhances immune function
Required for nerve cell development
What population is at greatest risk for Vitamin E deficiency
Premature infants
Insufficient stores
Can result in Anemia**:
Due to red blood cell fragility and subsequent rupture
What are the primary functions of vitamin K?
Blood clotting
Activates proteins required to make:
Fibrin
Forms blood clots
Also required for synthesis of bone protein
Osteocalcin
What population is at greatest risk for K deficiency?
Newborns
Relatively sterile GI tract at birth (bacteria is a non-food source and is the most significant source of Vitamin K in humans)
Breast milk is a poor source of vitamin K
Single dose of vitamin K given at birth!
Prolonged use of antibiotics
List the functions of vitamin C.
Acts as an antioxidant
Immune system health
Synthesis of collagen
Protein that forms connective tissue of tendons, bone, teeth, and skin
Functions of collagen:
Wound healing
Maintenance of blood vessel structure
Facilitates iron absorption in GI
What condition is caused by Vitamin C deficiency?
Scurvy
Severe deficiency
Improper formation of collagen
Anemia
Due to poor iron absorption
Signs of deficiency include:
Bleeding gums, loss of appetite, small hemorrages on skin, weakness
What are 3 dietary sources of Vitamin C?
Orange juice (best source)
Limes, lemons
Kiwis
Red bell peppers
Strawberries
Sweet potatoes, brussel sprouts
Describe the primary deficiency conditions associated with thiamin
(B1), niacin (B3), folate (B9) and vitamin B12.
Thiamin Deficiency:
Occurs in malnourished individuals and alcoholics
Beriber**
Heart becomes enlarged, fluid accumulates in skin and muscles weaken/atrophy
If condition affects CVD system:
****WET beriber
If condition affects Nervous system:
**DRY beriber
SEVERE DEFICIENCY IN ALCOHOLICS —→ Wernicke-Karsokoff Syndrome
Niacin B3:
Pellagra
Symptoms referred to as “the Fours Ds”
Diarrhea, dermatitis, dementia, death
Folate B9:
Inability to synthesize DNA during folate deficiency
Results in large, immature red blood cells that are fewer in number:
**Macrocytic anemia
Vitamin B12:
Macrocytic anemia
If due to lack of intrinsic factor:
Pernicious anemia
List the primary functions of vitamin B12 and folate.
Folate
Cell division
DNA replication requires folate during cell division
AffectsL
Red blood cell synthesis
Central nervous system formation during fetal development
Vitamin B12
Essential in converting folate into active form
Maintains the insulating lining that covers nerve fibers known as”
**Myelin shealth
Vitamins B12 and folate are important for homocysteine metabolism
High levels of homocysteine (AA) in blood = increased risk of CVD
Identify dietary sources of vitamin B12, folate, and folic acid.
Vitamin B12
Milk, cheese, meat (especially organ meats), poultry and seafood
Ready to eat cerals, soy products, supplements
Folate (naturally occuring form)
Orange juice, green leafy veggies, legumes, tomato juice, asparagus
Folic acid (synthetic form, easier to absorb in GI)
Supplements, enriched grains
Identify the toxicity condition associated with niacin.
One of the few water-soluble vitamins to have toxicity symptoms
Overconsumption of supplements or fortified foods
**”Niacin flush
Overconsumption of 3x to 4x RDA
Redness of face, arms, and legs
Temporary condition
High doses of nicotinic acid prescribed for cholesterol reduction results in niacin flush
**Liver injury
a. Describe the process of vitamin B12 absorption.
i. When B12 is consumed from food, what must happen first in
the stomach so that B12 can eventually be absorbed?ii) What protein is required for B12 absorption?
ccc
Identify individuals at risk for vitamin B12 deficiency and describe
why these individuals are at risk.
c
Describe the differences between macrominerals and microminerals.
v
Describe the process of blood calcium regulation when blood calcium becomes low.
v
What are the functions of calcium in the body?
v
Identify at least 3 good dietary sources of calcium.
v
List 3 modifiable and 3 non-modifiable risk factors for osteoporosis.
c
What are the primary functions of magnesium, phosphorus and sulfur in the body?
c
Identify 3 dietary sources of magnesium.
c
What minerals are involved with bone health?
v
What is the primary storage form of sulfur in the body?
c
Identify the role of iron in the body.
c
List the type of food sources (ie. animal or plant) that contain heme vs. non-heme iron.
c
Describe absorption of iron in the body.
v
What factors can increase and what factors decrease iron absorption?
v
What form of iron is most easily absorbed?
v
Identify individuals with increased iron requirements.
v
Identify the leading nutrient deficiency worldwide.
c
What are potential causes of anemia?
v
List the blood tests used to screen for anemia. Which is the most sensitive to low iron stores?
c
What is the condition associated with iron toxicity? What is the cause of this condition?
c
What factor(s) hinder zinc absorption and what factor(s) enhance zinc absorption?
d
What are two symptoms of zinc toxicity and deficiency.
v
Identify the primary function of copper in the body.
v
What other mineral may hinder copper absorption?
v
What is the primary role of iodine in the body?
c
What may occur if an individual becomes iodine deficient?
v
List 2 common dietary sources of iodine.
v
What is the primary function of selenium in the human body?
v
What is the primary function of selenium in the human body?
v
Can an individual consume too much fluoride? If so, what condition may develop?
vv
What population group may be recommended to take a chromium supplement? Why might this population take supplemental chromium?
List the two federal agencies involved in regulating supplements and supplement claims and labeling.
c
Identify populations in which dietary supplement use is most prevalent.
v
Describe steps involved in making an informed decision about taking dietary supplements.
c
Do doctors recommend beta-carotene for the general public?
NO
Is vitamin D toxicity common?
NO, toxicity is NOT common
Occurs from overuse of supplements
What factors influence vitamin D synthesis?
Distance from equator
Amount of clothing coverage on body
Sun block use
Cloud cover or smog
Age
Skin color
Is there an increased need for vitamin C in smokers?
YES
Describe the primary deficiency conditions associated with thiamin
(B1)
Occurs in malnourished individuals and alcoholics
Beriber**
Heart becomes enlarged, fluid accumulates in skin and muscles weaken/atrophy
If condition affects CVD system:
****WET beriber
If condition affects Nervous system:
**DRY beriber
SEVERE DEFICIENCY IN ALCOHOLICS —→ Wernicke-Karsokoff Syndrome
Describe the primary deficiency conditions associated with Niacin B3
Pellagra
Symptoms referred to as “the Fours Ds”
Diarrhea, dermatitis, dementia, death
Describe the primary deficiency conditions associated with Folate B9
Inability to synthesize DNA during folate deficiency
Results in large, immature red blood cells that are fewer in number:
**Macrocytic anemia
Describe the primary deficiency conditions associated with Vitamin B12
Macrocytic anemia
If due to lack of intrinsic factor:
Pernicious anemia