Test 3 - Echo
1/134
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
135 Terms
Minimal/Trivial TR
normal variant of TR, 80-90% of population has this
Proper leaflet motion
What are you looking for in a 2D eval of the TV
Tricuspid regurgitation
What are you looking for when evaluating the TV with Color Doppler
A4C, sample at tips, measure e’,a’, and deceleration time
Describe evaluating the TV using PW
Regurgitation and stenosis; peak velocity, peak gradient, mean gradient, VTI, PHT
What are you looking for when evaluating the TV using CW + what do you measure
Functional regurgitation
Any regurgitation caused by anything other than the leaflet, occurs in 75% of cases
RV abnormalities, LV HD, pulmonary HTN, annulus abnormalities
What can cause functional regurgitation
Structural TR
Any TR caused by the valves
Rheumatic, prolapse, congenital
What can cause structural TR
Jet area, vena contracta, CW shape&density, PISA, and hepatic vein flow
What do you look at when grading the severity of TR
Flow reversal
If there is severe TR, what happens to the hepatic vein
Weak tracing, parabolic shape
In CW, how will a mild TR appear
Dense tracing, triangular shape, max TR decreases as RAP increases
In CW, how will severe TR look
Tricuspid stenosis
Least common stenosis valulopathy
Rheumatic, congenital (Epstein), carcinoid HD, ra tumor
Causes of TS
Carcinoid heart disease
Thick rigid leaflets which appear frozen
SV/ VTI^tri
Continuity equation for TVA
TVA = 190/PHT
Calculate TVA using PHT
<1 m/s
Normal peak systolic velocity for TV
<2mmHg
Normal mean gradient for TV
7-9cm²
Normal TVA
RVOT in PLAX and PSAX basal
Standard views to image the PV, always color and CW trace VTI
Mild to Moderate
What grade of PR is this
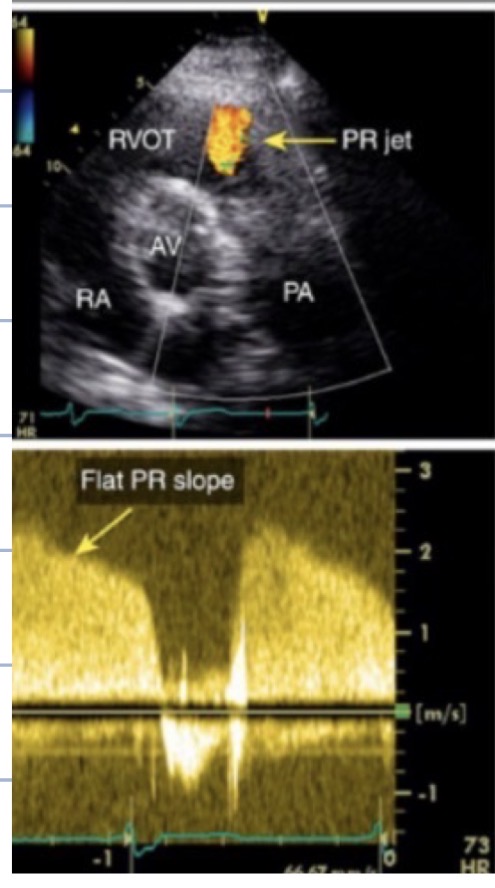
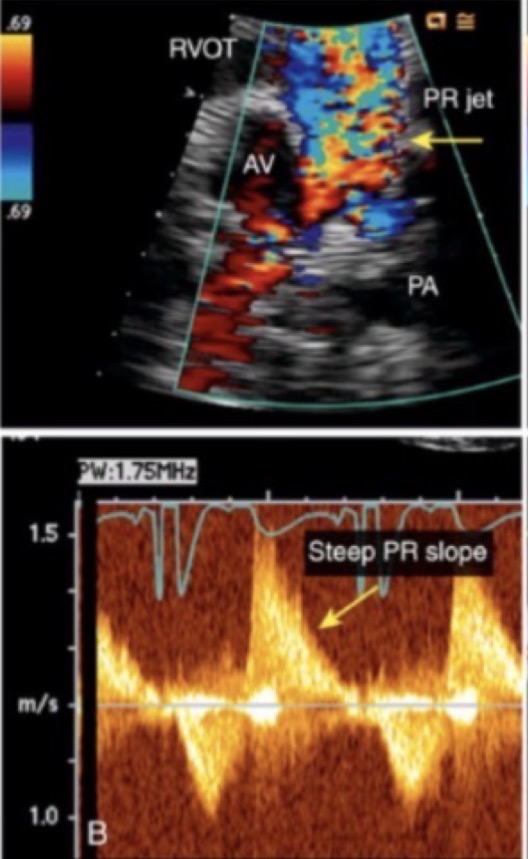
Severe PR
What grade of PR is this
Carcinoid disease and post surgical repair of pulmonic stenosis
What are the two most common causes of Pulmonary Regurgitation
The steeper the slope, the more severe the PR
How does slope seen on CW indicate pulmonic regurgitation
Congenital
95% of PV stenosis is ___
Double outlet RV, Tetrology of Fallot
Congenital causes of PV stenosis
PV <3 and PG <36
PV peak velocity and peak gradient MILD values
PV 3-4 PG 26-64
PV peak velocity and peak gradient MODERATE values
PV >4 PG >64
PV peak velocity and peak gradient SEVERE values
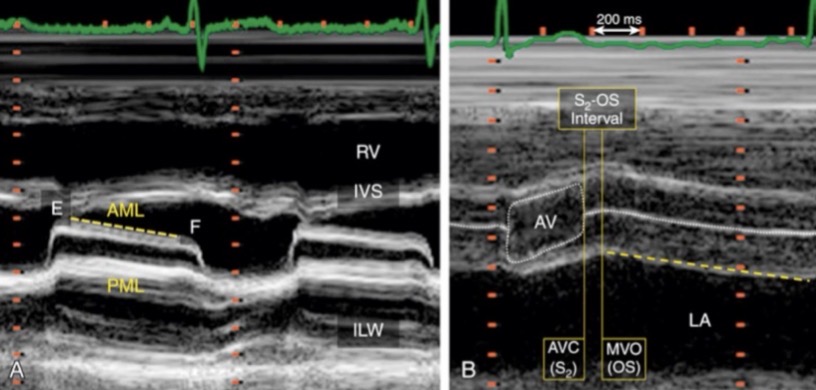
Full opening and closing
What is M-Mode looking for when evaluating the mitral valve
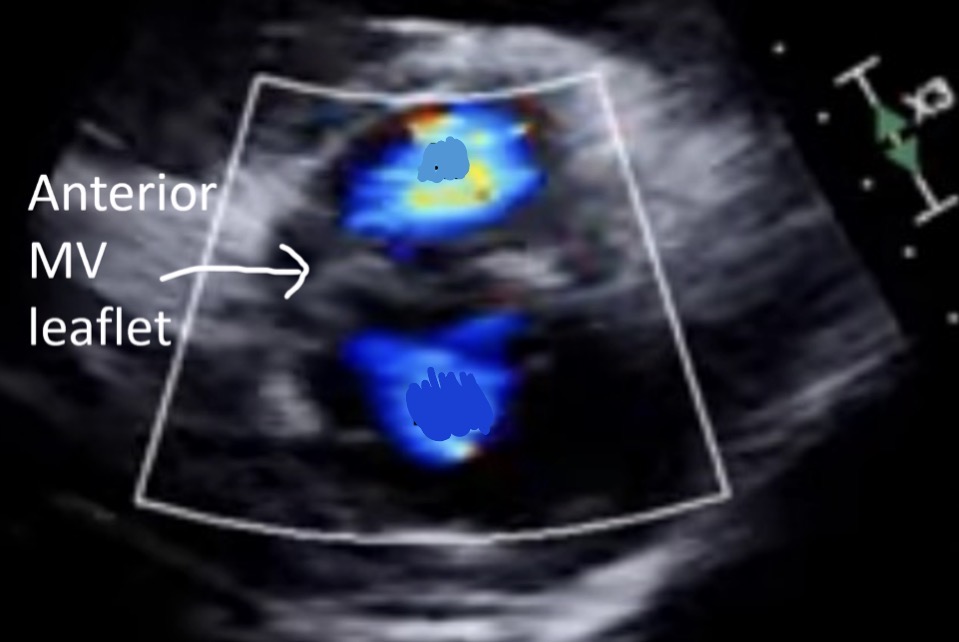
Below
In PSAX MR is seen ____ the anterior leaflet of the MV
Above
In PSAX AI is seen ____ the anterior leaflet of the MV
A4C, sample placed at the tips of open MV leaflets
Describe how to properly evaluate the MV using PW
Peak e’ , peak a’, diastolic deceleration time
What do you measure with PW when evaluating the MV
A4C, sample through a jet
describe how to use CW to evaluate the MV
Trace deceleration time, peak velocity, peak gradient, mean gradient, VTI
What do you measure if stenosis is identified through the MV using CW
If the MV appears abnormal, prosthetic, or has been repaired
When should you measure PHT if there is stenosis in the MV
Trace the backflow on spectral, peak velocity, peak gradient, VTI
What do you measure if regurgitation is seen in the MV using CW
Trace perimeter of leaflet tips at largest opening, measure deceleration, continuity equation, PICA
Ways to evaluate/calculate MVA
4-6 cm²
What is normal MCA size
Mitral stenosis
Obstruction of flow from the LA to LV because of MV narrowing
Rheumatic heart disease, calcification, endocarditis, lupus
List four causes of MS
Rheumatic MS
Most predominant cause of MS
Rheumatic MS
MS described by leaflet thickening and calcification starting at the tips and growing in, causes commissural fusion
Opening snap murmur, malar flush, hemoptysis, chest pain, fatigue, tachy
Signs and symptoms of Rheumatic MS
Malar flush
Plum red cheeks due to CO2 retention
Hemoptysis
Coughing up blood
Pulmonary edema and HTN, LAE, MR, increase risk for LA thrombus
List consequences of MS
Commissurotomy, balloon valvuloplasty, MV replacement, medications
List four treatments for MS
Commissurotomy
Procedure where the valve fusion is snipped
Balloon valvuloplasty
Balloon is inserted with a catheter to expand the valve
Anterior leaflet doming, RMS
What is the hockey stick sign and what pathology is it related to
Leaflet thickening, fish mouth appearance, hockey stick sign, chordal thickening
ECHO findings of RMS
Mitral Annular Calcification (MAC)
MC non rheumatic MS
Mitral Annular Calcification (MAC)
Calcium deposits in the mitral valve annulus
Reduces annular dilation, impaired mobility, calcifications on both leaflets
How does MAC affect the leaflets
MAC does not cause commissural fusion
What is one way to differentiate MAC from RMS
Cor Triatrium
Rare anomaly where a fibrous membrane divides the LA into two chambers
Flail Leaflet
Free movement of the leaflet into the LA, caused by ruptured chordae or papillary
Mitral Regurgitation
Retrograde flow from the LV to the LA through an incompetent MV
MV prolapse, flail MV, ischemic HD, RHD, Marfan’s
List 5 causes of MR
Fatigue, dyspnea, and dyspnea on exertion*
Signs and symptoms of MR
LAE, increase LA pressure, Pulmonary HTN, CHF
Complications of MR
Reduce amount of regurg
What is the goal of MR treatment
Mitraclip, surgical repair, MV replacement
Three treatments of MR
MV prolapse
Bulging of MV leaflets into LA during systole
leaflets bulge into LA in systole
What creates the systolic click sound associated with MV prolapse
Flail MV, Marfan’s, flail chordae or paps
Causes of MV prolapse
LAE, increased endocarditis, thrombus caused by afib
Complications of MV prolapse
S wave flip, D wave > S wave
PW sign of severe MR
EROA, Doppler-volumetric method, SV method
Quantitative ways to evaluate for MR
220/PHT
Formula for calculating the MVA using PHT
Hockey stick sign, RMS
What is this image showing
AI is above and MR is below
Which is MR and which is AI
3, Mercedes Bens
The AV has __ cusps and appears as the “____” sign when closed
2
How many coronary arteries arise off the AV cusps
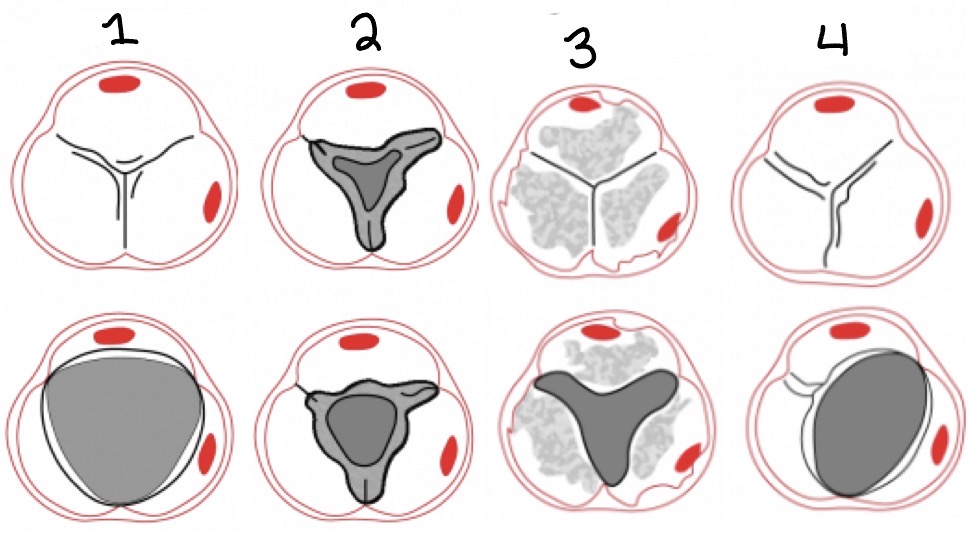
Normal, Rhematic, Calcification, Bicuspid
Label the different AV appearances
Bicuspid AV
Mc congenital abnormality of the AV
Bicuspid AV
Mc cause of isolated AO stenosis in patients under 50
85
AO stenosis occurs in __% of all BAV cases
Non centered valves, systolic doming, oval valves
ECHO features of Bicuspid AV
AO dilation, aneurysm, disection, coartation
Abnormalities associated with bicuspid valves
Stenosis, regurgitation, AO dilation
Complications of bicuspid AV
Unicuspid AV
AV that appears stenosis at birth
Unicuspid AV
AV with one attachment point, solitary opening
Quadricuspid AV
AV that appears like an x on PSAX
Aliasing
What are you looking for in color Doppler at the AV
Peak velocity and VTI, spectral signal (rapid upstroke and ED click
PW eval of the AV measure…
Aortic insufficiency (peak velocity and pressure Half time)
CW eval of the AV look for…
Plaimetry of AV Orfice
Tracing AV in systole to look for calcified AO stenosis
Continuity equation
equation which determines AVA
(CSA lvot x VTI lvot) / VTIav
How do you calculate the AVA
AVA x VTIav = CSA lvot x VTI lvot
Continuity equation
Volume flow rate should be constant throughout the body
What does the continuity equation tell us
Inaccurate LVOT measurement, irregular rhythm, sub AO obstruction, inaccurate sampling
Pitfalls that can affect the continuity equation
Pi x (D/2)²
CSA lvot equation
V lvot / V av
Velocity ratio equation
If there is low EF
When is the velocity ratio used instead of the continuity equation