Looks like no one added any tags here yet for you.
GI bleed
Upper
85% of bleeds
Esophagus, stomach, duodenum
Etiology
Ulcer
Esophageal varices
Liver damage – blood backs up into portal vein and then into esophagus
Lower
Jejunum, ileum, large intestine
Etiology
IBS (irritable bowel syndrome)
Hemorrhoids
UC
Chrons
GI bleed manifestations
Characteristics determine activity
Bright blood is happening in the moment and is not passed through the stomach
Coffee ground emesis
blood mixed with stomach acids
Hematemesis
Blood in vomit
Described as bright red or as coffee ground
Melena
Bright red blood in stool
Low in GI tract
Tarry
Older less severe bleed or traveled through the tract
Occult blood – hidden in the stool
GERD
Lack of pressure -> relaxation of gastroesophageal sphincter
Etiology
Smoking
Chocolate
ETOH
Fatty foods
Caffeine
Meds
Pregnancy
Manifestation
Heart burn
An hour after eating and/or laying down
Chest pain
Can mimic MI (Myocardial Infarction)
Feeling like cannot swallow or stuck in throat
Ulcerations
hiatal hernia
Present to some degree in 50% of the population
Portion of the stomach is moving through diaphragm into the esophagus or next to the esophagus
Manifestations
Heartburn
Dysphagia
Epigastric pain
GERD
Etiology
Paraesophageal hernia if it twists can lead to necrosis
Mallory Weiss tear
Tear in esophagus from prolonged vomiting
ETOH
gastritis
Inflammation of gastric mucosa
Etiology
Endotoxin
Caffeine
ETOH
NSAID
Aspirin
Blocks prostaglandins
Manifestations
Mild - Gastric pain
Severe - Vomiting
Severe - Bleeding
peptic ulcer
Etiology
ETOH
Aspirin, NSAIDS
Bile acids
Helicobacter pylori
Mechanisms
Decrease mucus production and prostaglandin deficiency
Manifestation
Vague abdominal pain to life-threatening hemorrhage
Pain usually burning, cramping, mid epigastric area
Perforation of gastric ulcer can lead to contents in the peritoneum
Decreased hematocrit
Chrons disease
Recurrent inflammation affecting any portion of the GI tract
Affecting LI and SI
15-35 yrs. old
Etiology and pathogenesis
Possible autoimmune problem – tumor necrosis factor
Lesion in bowel
Thickening of bowel and decreased flexibility
All layers of the gut
Genetic/hereditary component
Mechanism
Lesions develop in the bowel
Occur in patchy areas
30% in LI
40% in SI
30% other
chrons manifestations and complications
Manifestations
Periods of exacerbation and remission
Alternate between diarrhea and constipation
Oral lesions
Abdominal pain
Equal urgency and frequency
Weight loss – malabsorption
Increased risk of intestinal cancer
Complications
Fistula development from fibrosis
Skin or vaginal
Fistula between rectum and vagina
Intestinal obstruction
Abdominal and peritoneal abscess
ulcerative colitis
Inflammatory condition of the colon
Incidence highest in 20s and 30s
Increase risk of developing colon cancer
Etiology and pathogenesis
Lesions become necrotic and can ulcerate
Only occurs in rectum and colon
Lesions are continuous unlike chrons
UC manifestations and complications
Manifestation
Decreased appetite (anorexia)
Fatigue
Frequent stool – diarrhea's
Bloody stool
Mucousy stool
Fever severe abdominal pain
Complication
Colon cancer
Arthritis
diverticular disease
cannot eat popcorn, nuts, seeds
most prevalent in developed worked bc of lack of fiber
Increased pressure can be caused by lack of activity
Etiology
Mucosal layer herniates through muscular layer
Often multiple diverticula
Occurs most in sigmoid colon
Disease is most prevalent in developed world due to lack of fiber in the diet
Prevention
Increase fiber 20-35g of fiber
Increase hydration
diverticulitis
Mechanism
Inflammation of diverticulum with small ulcerations
Manifestation
Increased WBC
Nausea
Vomiting
fever
Complications
Peritonitis
Bowel obstruction
Hemorrhages
Fistula formation
colorectal cancer
Not every polyp is cancerous
Can be lethal
Symptoms occur in late stages
Why it is so lethal
Etiology
Genetic and environmental causes
Familial adenomatous polyposis
Genetic
Hereditary non-polypuosis colon cancer
No polyps
Environmental
Low-fiber high fat
Dietary fat intake – increase synthesis of bile acids
Inadequate intake of vitamins A, C, and E
Cauliflower cabbage, Brussels sprouts
colorectal cancer manifestations
Bleeding – significant early symptom
Change in bowel habits
Diarrhea
Constipation
Urgency or incomplete emptying of bowel
Pain is a late symptom
IBS (irritable bowel syndrome)
Chronic and recurrent intestinal symptoms
15-20% of the population
Most do not seek medical attention
Etiology
Stress
Hyperactivity of the bowel
Manifestations
Symptoms
Abdominal pain
Complaints of flatus
bloatedness
Nausea
Anorexia
Anxiety
Depression
Vomiting
Signs
Changes in frequency and consistency of stool
Symptoms for at least 3 months to get dx
hepatitis A
Etiology
Virus
Single stranded RNA Virus
Incubation period of 2-6 weeks
Hepatocytes are sole site of replication
Fecal – oral route of transmission
Breastmilk, water, shellfish
Symptoms
Fever
Malaise
Nausea & anorexia
Jaundice
Tea colored urine & clay-colored stools
Once disease resolves – develop antibodies and will not return
hepatitis B
Etiology
Double-stranded – DNA virus binds to hepatocytes
Transmission
Blood and bodily fluids (saliva and semen)
Prophylaxis
Hep B immune globulin
Hep B vaccine
Groups at risk
Healthcare providers
Sexually active heterosexuals or homosexuals
IV drug abusers
Autoimmune response – inflammation of the liver
This leads to damage and destruction of bile cannula
hepatitis B and C manifestations
Manifestations
Do not occur for 2-3 months after exposure
Fulminant hepatitis
Rare syndrome
Rapid (days or weeks) massive necrosis of liver parenchyma and atrophy of liver
High mortality
Fatigue
Malaise
Anorexia
Headache
RUQ pain
Decreases in liver function tests
carrier state Hep B
continue to harbor the virus, no symptoms, are contagious
Anti-HBc – antibody to core antigen- means you had exposure to the disease
Patients do not develop antibody to the surface antigen.
No Anti-HBs
chronic hepatitis
may or may not have symptoms
Later stages develop liver failure
Positive surface antigen
Virus is still replicating
No antibodies
hepatitis C
Chronic hepatitis
Single stranded RNA Virus
Also transmitted through blood and bodily fluids
No vaccine for Hepatitis C
80% of patients will go on to be carriers
Progressive fibrosis leads to cirrhosis and end stage liver disease
Higher incidence of cancer
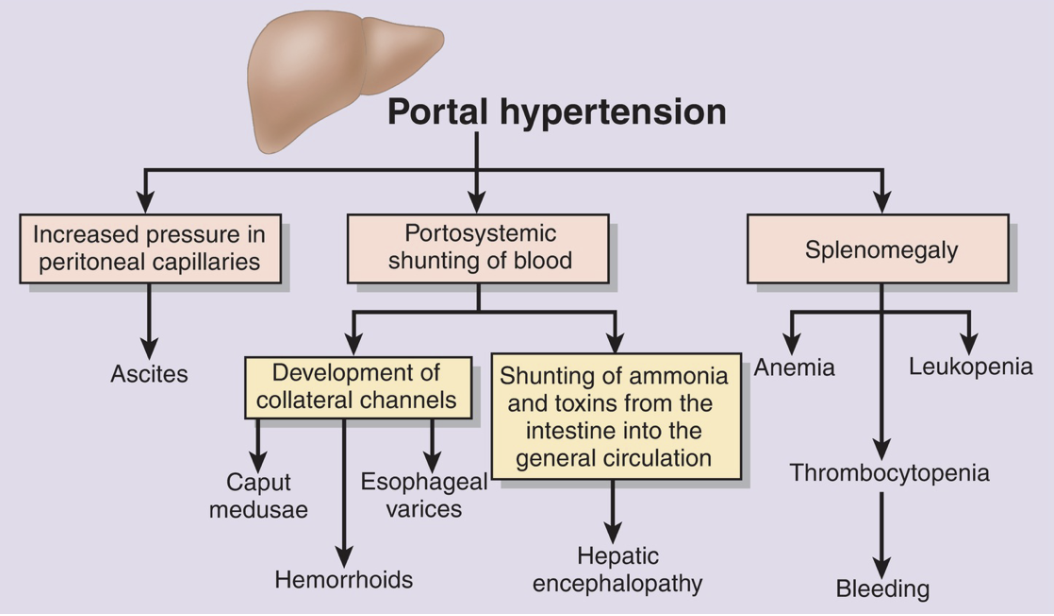
complications of cirrhosis
o portal hypertension
o splenomegaly
o ascites
o hepatorenal syndrome
o hepatic encephalopathy
o esophageal varices
portal hypertension
increased pressure within the portal venous system
can cause:
Ascites
Splenomegaly
esophageal varices
Backup in veins of esophagus
Low pressure system becomes high pressure
Causes weakening and out-punching of esophageal veins
Life threatening
ascites
accumulation of fluid within the peritoneal cavity
spelomegaly
due to shunting of blood into the splenic vein
hepatic encephalopathy
central nervous system manifestations
Toxins cross blood brain barrier
Symptoms
asterixis - flapping tremor
loss of memory
personality changes
impaired speech
Coma
Lactralose
Binds to ammonia and excreted through feces
hepatorenal syndrome
a multiorgan condition affecting the kidneys and the liver
Possibly due to decreased renal blood flow
increased creatinine
increased BUN
decreased urine output
cholelithiasis
development of gallstones
Etiology
high cholesterol in bile
Mechanism
development of cholesterol stones
Manifestation
may be asymptomatic
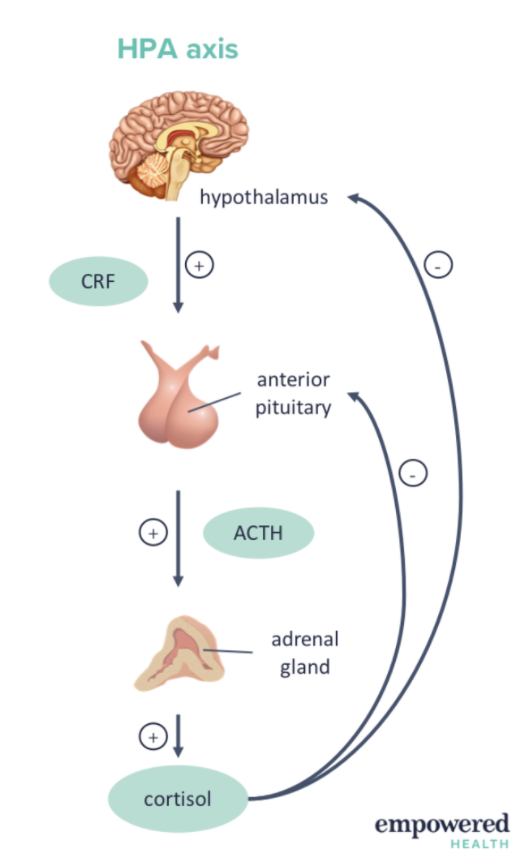
adrenal axis
Stress stimulates hypothalamus to release CRH
Stimulates anterior pituitary to release ACTH
Stimulates adrenal glands to release glucocorticoids and mineralocorticoids
Glucocorticoids - cortisol
Mineralcorticoids – ADH – affects sodium and water
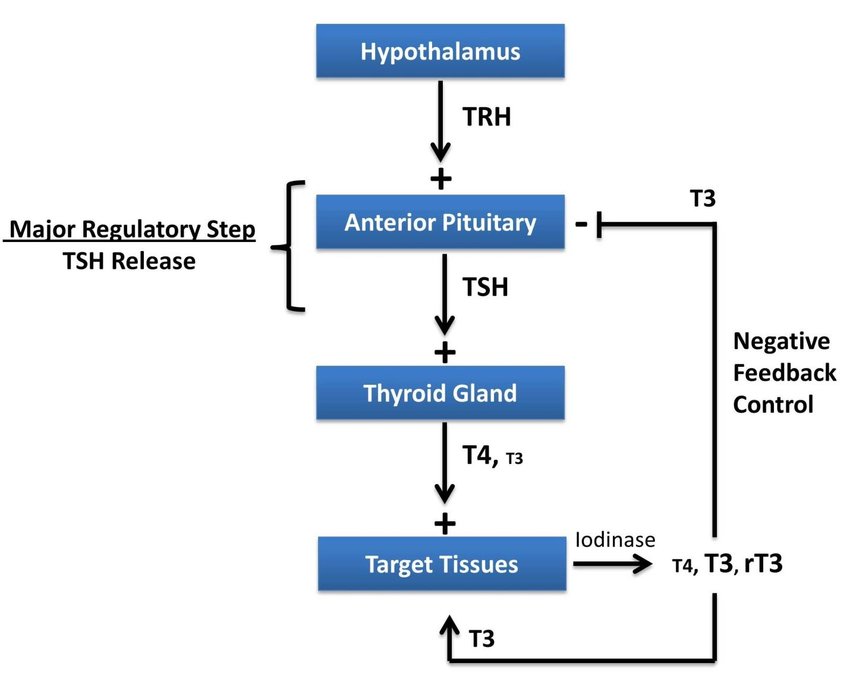
thyroid axis
TRH – thyroid releasing hormone stimulates TSH from anterior pituitary hormone
Stimulates release of T3 or thyroxine (T4) from thyroid
With hypothyroidism there is negative feedback mechanism bc T3 and T4 are decreased so TRH and TSH increase (tertiary problem)
primary disorder
when the end organ is not able to put out the hormone
examples e.g., thyroidectomy or adrenalectomy
hyper/hypothyroidism - problem with thyroid gland TRH and TSH will decrease
hypothyroidism - problem with
secondary disorder
when the hypothalamus or pituitary are unable to put out hormone
example e.g., removal of the pituitary gland
secondary hyper/hypothyroidism - problem with the pituitary or hypothalamus
TSH and TH will increase
TRH will decrease
Hypothalamic pituitary regulation
Hypothalamus causes release of hormone → pituitary releases hormone → stimulates the gland to release hormone that targets cells
antiduretic hormone
arginine vasopressin released from the posterior pituitary in response to increased osmolality sensed in the supraoptic nuclei of the hypothalamus
release also stimulated if plasma volume low
sensed in the aortic and carotid arch, and left atrium target organ distal tubule of the kidney collecting duct
Released from posterior pituitary
Produced in hypothalamus
Does not travel via portal system like with anterior pituitary
Causes release
Plasma osmolarity
How concentrated blood is
280-295 mOs/kg
Increase = release of ADH
Also increase in thirst
thyroid hormone
Helps with metabolic rate
HR and contractility are enhanced
Potentiates (makes the more effective) norepinephrine and epinephrine
Growth and development in children
Metabolic Rate - increase in BMR by 60 to 100% by large amounts of thyroxine secretion
Cardiovascular Function - heart rate and contractility are enhanced
Gastrointestinal Function - increased appetite
Neuromuscular Effects
increased levels, muscles react more vigorously
decreased levels, muscles are more sluggish
diabetes insipidus
insufficiency of ADH
Etiology
neurogenic - inadequate production problems with synthesis, transport, release due to:
tumors
hypophysectomy
aneurysms
thrombosis
infections
immunologic disorders
commonly head injury
nephrogenic - inadequate response
genetic
some drugs damage the renal tubules
pyelonephritis
polycystic disease
general anesthetics
lithium carbonate
diabetes insipidus manifestations
low urine specific gravity 1.000 to 1.005
low urine osmolality
Less concentrated and more watery
polyuria
1/2 cases 4 to 8 L/day
1/4 of cases 8 to 12 L/day
dehydration unless fluid replaced
Increased blood osmolality
SIADH (Syndrome of Inappropriate Antidiuretic Hormone Secretion)
Genetic derepressing
Functions are unlocked
Production of ADH
Cancer cells begin to produce ADH
No regulation
Become hyponatremic
Decrease in serum sodium and serum osmolality
Changes in LOC
Can see seizure activity
Etiology
ectopic tumor cells
oat cell adenocarcinoma of the lung
carcinoma of the duodenum, pancreas, etc.
Mechanism
water retention
expansion of intravascular volume
SIADH manifestations
Signs
hyponatremia - dilutional
hypo osmolality - dilutional
urine hyperosmolality - concentrated
Symptoms
thirst
impaired taste
GI symptoms
vomiting
abdominal cramps
Neuro symptoms
confusion
lethargy
muscle twitching
Convulsions
hypothyroidism
Etiology
lymphocytic thyroiditis most common
thyroidectomy
secondary hypothyroidism
Manifestations of hypothyroidism
Weakness – most common
fatigue
tendency to gain weight
cold intolerance
decreased gastric motility
mental dullness
lethargy
impaired memory
Goiter
Not enough iodine
Still increases in size because it is trying to release T3 and T4
hyperthyroidism
Etiology & Mechanisms
graves' disease – most common
Antibodies produced that bind for TSH in thyroid
Cause release of T3 and T4
adenoma of the thyroid
OD thyroid hormone
myxedema coma
coma
hypothermia
cardiovascular collapse
hypoglycemia
hyponatremia
hyperthyroidism manifestations
hypermetabolic state – most common
Nervousness
Goiter
Increases due to overactivity
Exophthalmos
Buildup of mucous membrane behind the eye
irritability
fatigue
weight loss
large appetite
tachycardia
palpitations
shortness of breath
Sweating
Loss of menstrual cycle
Oligomenorrhea
Increase in temperature
addison’s disease (primary adrenal insufficiency)
Etiology
Autoimmune - 75% of cases
Many other rare causes
fungal infection
viral infections
metastatic cancer
adrenal hemorrhage
genetic predisposition
Mechanism
90% of adrenal gland destroyed before signs show up
addison’s manifestations
insufficient mineralocorticoid effects – most common
urinary losses of sodium, chloride, water, decreased excretion of potassium
orthostatic hypotension
dehydration
weakness
fatigue
hyperkalemia
hyponatremia
insufficient glucocorticoid effects
poor tolerance to stress
hypoglycemia
lethargy
weakness
Bronze color to skin
Produce too many melanocytes stimulating hormones
cushing’s
Etiology
administration of corticosteroids – most common
prednisone
inappropriate production of ACTH from ectopic tumors
inappropriate production of CRH from ectopic tumors
adrenal tumors
pituitary tumors producing too much ACTH
cushing’s manifestations
Manifestations
Obesity - extremities are unaffected altered fat metabolism – most common
Skin - loss of subcutaneous fat skin becomes thinner
Poor wound healing
Musculoskeletal system - increased bone resorption causes osteoporosis, muscle wasting
Cardiovascular system - HTN
Gastrointestinal system - increased gastric acid secretion
Sex Characteristics -
menstrual irregularities
increased facial hair in females
decreased libido in men and women
Eyes - increased ocular pressure
Glucose Intolerance – insulin resistance, increased gluconeogenesis
Psychological Changes - irritability, emotional lability, depression, paranoia
Thinning of hair
Facial flush
Pendulous abdomen
Easy bruising
Increased blood glucose
Insulin resistance
Osteoporosis
secondary adrenal insufficiency
destruction of pituitary
Etiology
pituitary tumors
pituitary infarctions
trauma
radiation
surgery
Manifestations
Insufficient glucocorticoid effects
poor tolerance to stress, hypotension
hypoglycemia
lethargy
Weakness
parathyroid hormone
responsive to ionized calcium
produces parathyroid hormone
Helps reabsorb calcium in the kidneys and gut
Helps osteoclasts to break down bone and increase calcium levels
hypoparathyroidism
Etiology
incidental surgical removal during thyroidectomy
Signs - manifestations related to hypocalcemia
increased neuromuscular excitability
Seizures
Abnormal EKG (due to lack of calcium)
Trousseau's - carpal pedal spasm
Symptoms
tingling in the hands
hyperparathyroidism
Seen more than hypoparathyroidism
Etiology
Idiopathic – do not know why
Will remove part of parathyroid glands to treat it
Manifestations
pathologic fractures
increased calcium in blood
Can lead to calcium stones in the kidneys
Osteopenia
Pathologic fractures
excretion of phosphate
glucagon
Alpha cells of the pancreas
Released with decreased glucose levels
Stimulates glycogenolysis (glycogen -> glucose) & gluconeogenesis (breakdown of amino acids to form glucose)
insulin
Beta cells of the pancreas
Released with increases in glucose
Promotes movement of glucose into cells
Helps build fat stores
Decreases gluconeogenesis
type 1 DM
Etiology
Genetic factors
Autoimmunity
Pancreatic beta cells destroyed by T-lymphocytes
Results in insulin deficiency and eventually dependence
Environmental factors
Mechanisms
Develops during childhood or young adults
Begins asymptomatic
Insulin dependent
Manifestations
Polydipsia
Very thirsty
So much sugar in bloodstream
Increasing amount of solutes in the bloodstream creates a state of dehydration
Polyphagia
Increased hunger
Glucose cannot enter cells due to decrease in insulin
Body is starving
Polyuria
Kidneys are trying to dump out excess glucose in urine
type 2 DM
Etiology
Genetic and Environmental Factors
60% of individuals with this type of DM have a sibling or parent with Type II DM
Glucose Metabolism
Hyperglycemic; sufficient insulin levels, insufficient insulin receptors
Mechanism
Non-Insulin Dependent
Failure of beta cells to keep up with insulin production
Insufficient insulin production by beta cells
Insulin resistance secondary to obesity – can reverse with weight loss
Adequate insulin production decreased sensitivity
May initially be asymptomatic
diabetic ketoacidosis
Usually type 1 DM
Lack of insulin -> fatty acid mobilization -> ketone bodies - > metabolic acidosis
CBG 400-600 mg/dl
Hyperglycemia – osmotic diuresis
Glucosuria (glucose in urine), polyuria (excessive urination), dehydration, hypokalemia (low levels of potassium)
Potassium moves inside the cell with insulin
With no insulin it stays in the blood stream and is unused
DKA manifestations
Manifestations
fruity breath
Tachypnea
Polyuria
Polydipsia
N/V
Fatigue
Dehydration
coma
HHNK (hyperglycemic hyperosmolar nonketotic coma)
Usually, T2DM
Plasma glucose > 600
Higher than DKA
No ketone bodies
Osmotic diuresis -> dehydration
most frequently in type II NIDDM individuals
Type 2 non-insulin dependent diabetes mellitus
mortality rate 40 to 70 %
Manifestations
Decreased LOC
Seizure
Hemiparesis
One sided weakness
Aphasia
Muscle fasciculations (twitches)
Polyuria
Dehydration
Hyperthermia
diabetic neuropathy
Etiology
vessel ischemia to nerve
demyelination of the Schwann cell
Manifestations
loss of feeling
loss of touch
position sense lost
impaired temperature and pain sensation
impotence
diabetic retinopathy
leakage of plasma from the vessels
fibrotic changes and new blood vessels develop in the retina due to ischemia
nephropathy
Causes CKD (chronic kidney disease) or end stage renal disease
sleep stages
non-REM
stage 1-4
REM sleep
sleep deprivation
Manifestations
Drowsiness
Inability to concentrate
Impaired memory
Reduced physical strength
Diminished ability to fight off infections
Hallucinations
Severe mood swings
sleep changes across lifespan
sleep stage 50-60 minutes in infants
Will sleep a lot
80% is REM sleep
Newborns sleep 17-24 hours a day
Age 2 – REM 30-35%
Infants in 6 months 14-15 hours
sleep stage 90 minutes long in the adult
decreased sleep requirement over time
stage 4 sleep is absent in individuals 70 years of age or older
Sleep in elderly is related to dementia
Easier to wake up bc no stage 4
physiologic changes in sleep
cough reflex diminished
decreased clearance of respiratory secretions
decreased swallowing and esophageal motility
decreased glomerular filtration rate
increased aldosterone production
REM
serotonin needed for priming of REM sleep
loss of muscle tone
loss of ability to thermoregulate
eye movements
Rapid irregular respirations
fever manifestations
Behavioral
Put on clothes
Put on blankets
Experiential
Increased amount of slow sleep
CV
HR increase
10% rise in metabolic rate per 1 C degree rise
Increased O2 consumption because metabolic rate
Immune system function is enhanced
Fever is treated when it gets to hyperthermia because it can damage CNS
Treat pregnant moms
People w cardiac or pulmonary problems – cannot tolerate metabolic rate
Physiologic
Cardiovascular
increased heart rate
increased cardiac output
Pulmonary
increased oxygen consumption
increased respiratory rate
Metabolic
decreased production of albumin
increased production of acute phase proteins
altered drug metabolism
Immune System
immune system function enhanced during fever
hypothermia
Mild hypothermia 32-35oC (89.6-95oF).
Moderate hypothermia 28-32oC (82.4-89.6oF)
Severe
hypothermia < 28oC (<82.4oF)
Etiology
Long extractions from car accidents
Water
Outside sports
Populations at Risk
Elderly
very young
individuals with chronic diseases
Manifestations
decreased heart rate
decreased cardiac output
development of coagulopathies
depressed CNS
pain
whatever the patient says it is
REM
25% of sleep
Decrease in temperature
More psychologically restorative
Towards end of sleep cycle
Dreams
Decreased with alcohol if drinking before bed
Sleep Stages 1-4
Stage 1
light sleep
Stage 2
50% of sleep
Stage 3
15% of sleep
More physiologically restorative
Stage 4
15% of sleep
deep sleep
circadian rhythm
Cortisol peaks an hour before you wake up
In depressed people cortisol stays up in the afternoon
Depressed people have prolonged sleep
Stomach most likely to be empty in the morning
Temperature goes down as you start to fall asleep but is highest in the evening
spinothalamic tract
Transmitted from thalamus to sensory cortex
Fast Pain vs. Slow Pain
A delta axons - myelinated
C fibers - unmyelinated
pain manifestations
increased heart rate
increased blood pressure
increased respiratory rate
dilated pupils
Stress response
pallor and perspiration
nausea and vomiting
urine retention
elevated blood glucose
From stress response
visceral pain
visceral organs
Hard to locate exactly where pain
Afferent pathways from the heart are shared with pathways in other areas - left arm, chest, jaw
all bladder pain refers to the right shoulder
Brain cannot differentiate
somatic pain
muscles, tendons
cutaneous pain
superficial structures
referred pain
pain that is perceived at a site different from its point of origin but innervated by the same spinal segment