Week 8-Haemostasis and Coagulation Tests
1/61
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
62 Terms
Haemostasis
Process of stopping loss of blood from blood vessels
– Include Coagulation (clot formation) and Fibrinolysis (dissolution)
– An interrelated and interdependent system
Hemostasis involve four major phases
– 1. Vasoconstriction / vascular spasms
– 2. Platelet activation / plug formation
– 3. Coagulation / clotting
– 4. Fibrinolysis
Vasoconstriction / vascular spasms→First phase of hemostatsis
blood vessels narrow
Broken blood vessels attract platelets (collagen exposure)
Anchored platelets (adhesion) release serotonin
causes blood vessel muscles to spasm (contract)
Spasms narrow the blood vessel, decreasing blood loss/flow
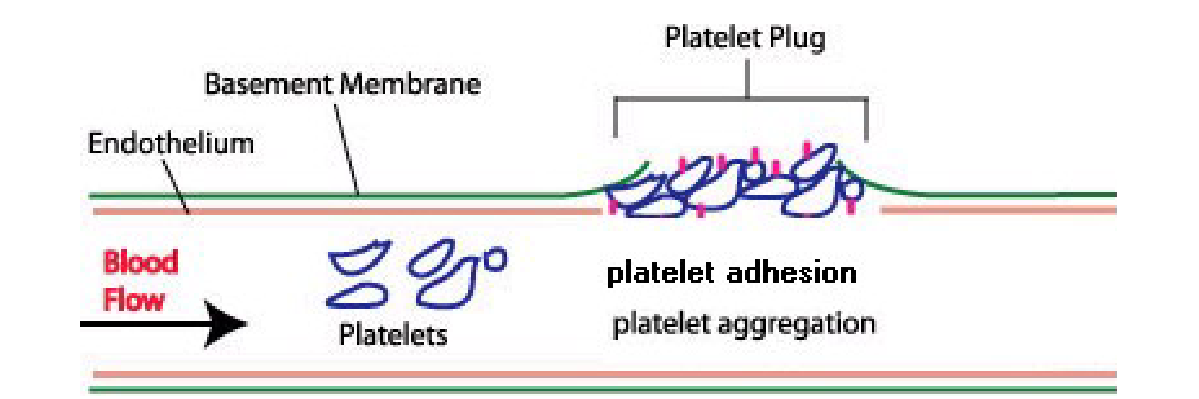
Platelet Activation→Second phase of hemostatsis
undergo Adhesion + Aggregation
Initiated by damaged or irregular blood vessels
Platelets adhere to damaged blood vessel due to collagen (exposed when vessel breaks, platelts have special binding site)
– platelet adhesion
cause platelet to activate, and turn to its dendritic form
Anchored platelets release chemicals to attract more platelets
– platelet aggregation
in dendrite form release chemicals to attract other platelets
like Adenosine Triphosphate (ADP)
inducing aggregation to the site
Thromboxane
cause platelets to interlink and activate exponentially
induces activation of thrombin
stimulate platelet activation further (positive feedback loop)
and induce fibrin to stabilize clots
Aggregate and stick to each other to form a plug
Stop bleeding in a small wound
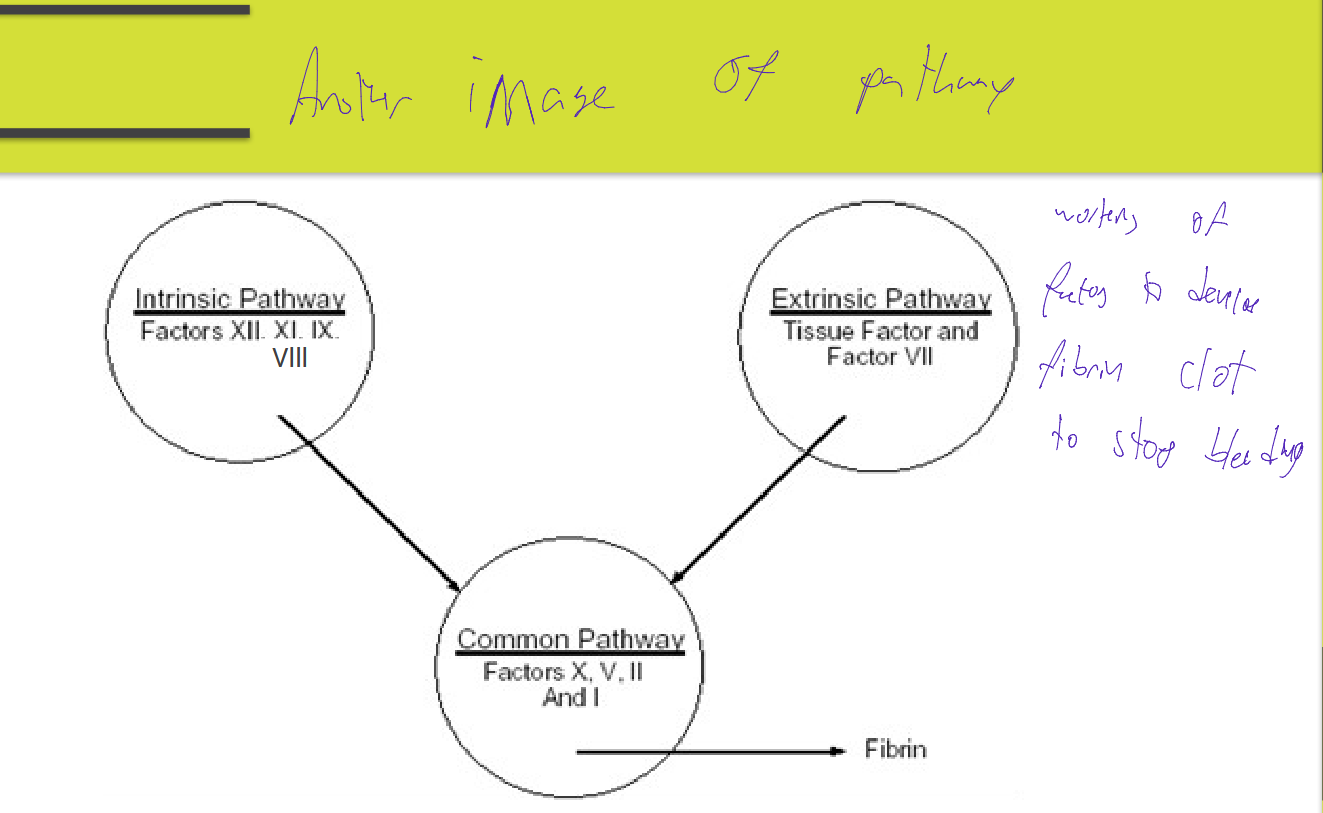
Coagulation / Clotting→third phase of hemostatsis
Intrinsic & Extrinsic pathways merging into a Common pathway
Factors in the Intrinsic pathway: (what is used in a PTT)
Involves factors
XII, (7)
XI, (6)
IX, (4)
VIII, (8)
[X, V, II, and I] (10. 5, 2, 1); (the common pathway)
Each activated factor activates the next in the series
Initiated by contact with surface of blood vessel lining
actor XII is activated; each activated factor activates the next in the series
XII→(need fletcher) XI→(need Ca++ to activate) IX→ (need Ca++ and PF3 to activate) VIII
PF3: platelet factor
![<p>Involves factors</p><ul><li><p>XII, (7)</p></li><li><p>XI, (6)</p></li><li><p>IX, (4)</p></li><li><p>VIII, (8)</p></li><li><p>[X, V, II, and I] (10. 5, 2, 1); (the common pathway)</p></li></ul><p></p><ul><li><p>Each activated factor activates the next in the series</p></li><li><p>Initiated by contact with surface of blood vessel lining</p></li><li><p>actor XII is activated; each activated factor activates the next in the series</p><ul><li><p>XII→(need fletcher) XI→(need Ca++ to activate) IX→ (need Ca++ and PF3 to activate) VIII</p><ul><li><p>PF3: platelet factor</p></li></ul></li></ul></li></ul><p></p>](https://assets.knowt.com/user-attachments/cf90b1ec-b912-4c61-9312-aec2d6be1cf9.png)
PTT (partial prothrombin time)
Used to detect congenital and acquired deficiencies of the above factors and to monitor heparin therapy
factors XII, XI, IX, VIII, [X, V, II, and I]
Each activated factor activates the next in the series
FOR TESTING OF THE INTRINSIC PATHWAY
Extrinsic pathway INVOLVES what factors
Factors
VII,
[X, V, II, I]
Thromboplastin (factor III) is released from tissue and damaged blood vessels, and activates the next factor (factor VII)
factor III+Ca++→ activated VII and activating extrinsic pathway
PT (prothrombin time)
Used to monitor Warfarin/Coumadin therapy
Thromboplastin (factor III) is released from tissue and damaged blood vessels, and activates the next factor
Ca++ is needed to activate factor VII
Factors in the common pathway
Factors X, V, II, and I
• Activated factors VII (by the Extrinsic) or VIII (by Intrinsic)
• Activate the next factors in the series
Factor 10 activate thrombin, allowing further activation of platelets, and fibrin
Is done to perform the following process (ACTIVATES THROMBIN
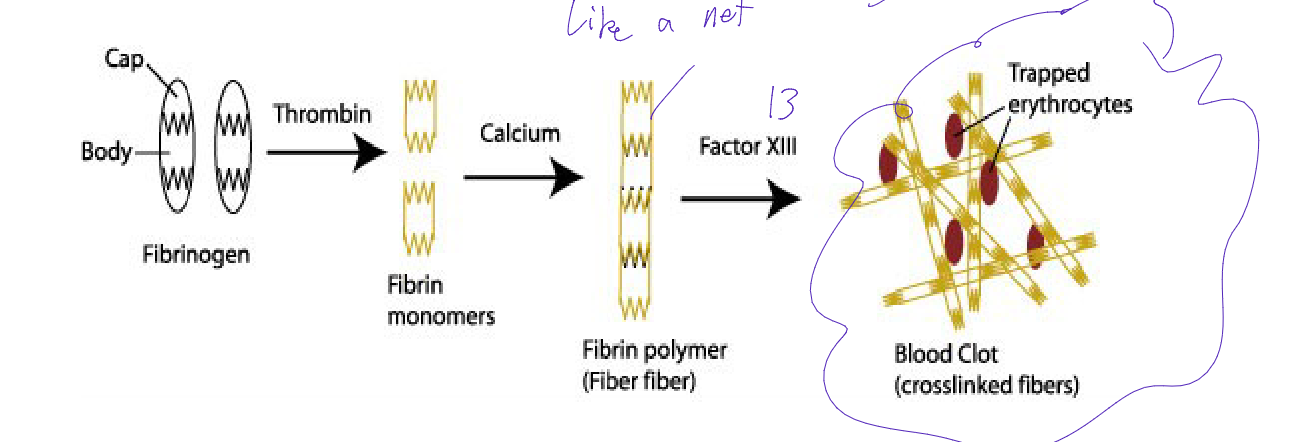
Fibrinogen (I) {with Thrombin)→ Fibrin (monomer) {with calcium)→ Fibrin (polymer) {with factor III) → Stable fibrin clot (secondary hemostatsis)
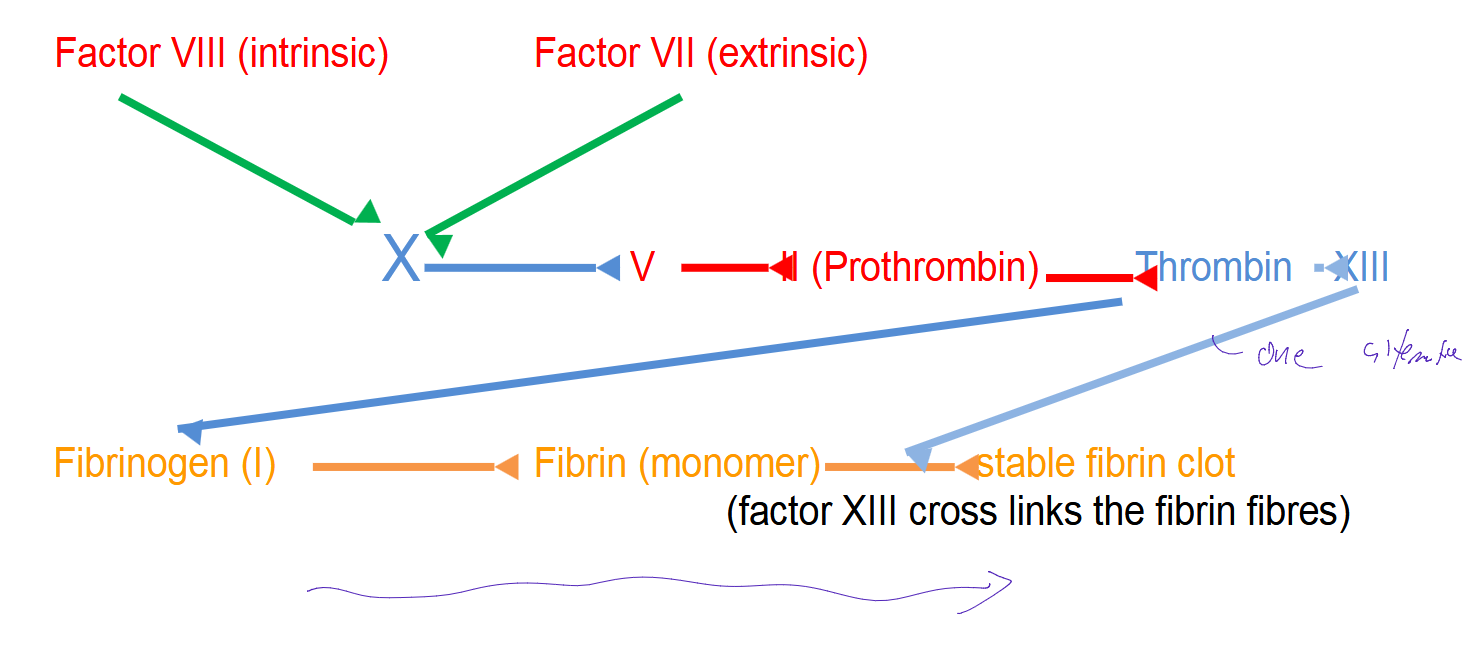
Overview of how Instrinsic and Extrinsic Pathway lead to the common pathway
Factor VIII (intrinsic) and/or Factor VII (extrinsic) activate factor X
X→V→II (prothrombin)→ Thrombin → XIII
Thrombin can activate Fibrinogen (I)→Fibrin (monomer) → to form a stable fibrin clot
(factor XIII cross links the fibrin fibres)
XIII can direcrly bind to fibrin and form the stable clot
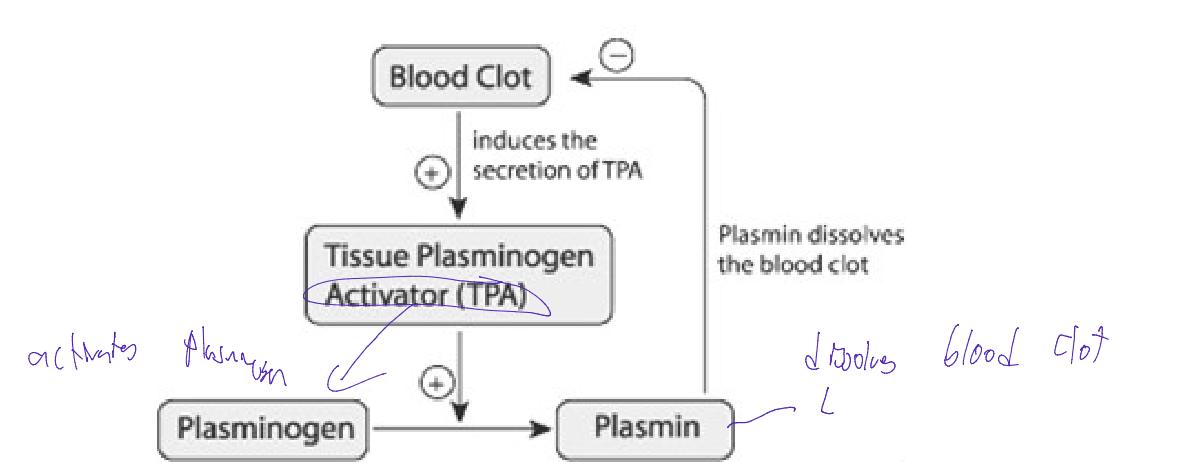
Fibrinolysis
Breakdown of fibrin after tissue is repaired
Initiated by the conversion of plasminogen to plasmin
based on negative feedback loop
Blood clots activate Tissue plasminogen activator (TPA),
this increases Plaminogens conversion into Plasmin
PLASMIN Dissolves blood clot
This more blood clot means increase activation of plasmin
Problems in Haemostasis
Insufficient or delayed clotting
Intravascular clotting:
Thrombus and/or thrombosis
(clot on vessel wall)
embolus
Clot can break off which travels through the blood
lot can lodge in the brain (stroke), heart (cardiac infarction), lung (pulmonary embolism), calves (deep vein thrombosis or phlebitis)
defect of X chromosome (Inherited Disorders Bleeding disorders)
Haemophilia A
factor VIII deficiency
Haemophilia B
factor IX deficiency (Christmas disease)
Chromosome 4 defect
Haemophilia C
factor XI deficiency
Von Wildebrand’s disease {Inherited Disorders: (Bleeding disorders)}
Platelet do not aggregate and do not activate factor VIII
Thrombocytopenia {Inherited Disorders: (Bleeding disorders)}
Low platelet count – can also cause a bleeding disorder
Vitamin K deficiency (Acquired Blood Disorders)
Factors ll, Vll, lX and X are vitamin K dependent
lead to clotting issues
Disseminated Intravascular Coagulation (DIC) (Acquired Blood Disorders)
most often due to infection
clots shut down organs; result in death
Heparin; Coumadin (Warfarin) (Acquired Blood Disorders)
Affect patient ability to clot, could bleed to death
Aspirin (Acquired Blood Disorders)
has anti-platelet properties
Liver Disease(Acquired Blood Disorders)
Most coagulation factors are synthesized in the liver
e.x cirrosis
Coagulation Tests
• Bleeding Time
• Prothrombin Time – PT
• (Activated) Partial Thromboplastin Time – APTT or PTT
Bleeding Time
Screening test for platelet function, capillary integrity and clotting factors
Method
• Standard puncture made,
and blood blotted by filter paper to prevent external clotting
Platelet count of < 50×109 - may prolong the bleeding time
old test not readily used
(Miekle Modified) Ivy Method – Bleeding Time Test
Blood pressure cuff on the patient’s forearm inflated to 40 mm Hg
Standard puncture on the forearm by a template device (2 incisions 5 mm wide and 1 mm deep)
Template device (Simplate or Surgicut) retractable blade
Start a stop-watch when the puncture is made
Record the time at which the bleeding stops
Normal Range for bleeding time
• Normal Range 1 - 9 minutes
Critical Value for bleeding time
• Critical Value > 12 min
Quality Control for Bleeding time
• Do not touch the incision when blotting blood droplets (will remove clots forming)
• Record if the patient used aspirin in past 2 weeks (as it affects platelets functionality)
• Proper PPE
• Follow Standard Precautions
Prothrombin Time test – PT
• Used to monitor oral anticoagulant therapy (Coumadin)
• Specimen: citrated plasma (light blue top tube)
• Centrifuge whole blood for 15 min at 3000 rpm (need platelet poor plasma)
• Separate plasma and refrigerate; freeze plasma if not tested within 4 hours
• Note: Some factors deteriorate rapidly – Factors VIII, VII, X, V
• Test Extrinsic pathway III → VII & common pathway → X→ V→ II→ I (→ ) these steps require Ca++)
• PT increased by deficiency of factors VII, X, V, II (prothrombin) and I (fibrinogen)
• PT increased in liver disease
• Factors ll, Vll, lX and X are vitamin K dependent
what factors deterioate rapidly even if tube is clsoed
Factors VIII, VII, X, V
PT – Test procedures
• Reagent – thromboplastin (tissue factor III; of the extrinsic pathway) and Ca++
• Reagent and specimen are incubated for 5 minutes at 37ºC
• Incubate no longer than 10 mins
– Factor VIII deteriorates, Reagent evaporates (and make sure to keep covered)
• Reagent is added to plasma and time to form a clot is measured
• Perform in duplicate: PT result must be within 10%
Factors that increase PT (clinical reasons)
deficiency of factors VII, X, V, II (prothrombin) and I (fibrinogen)
PT increased in liver disease
Vitamin K deficency
factors ll, Vll, lX and X are vitamin K dependent
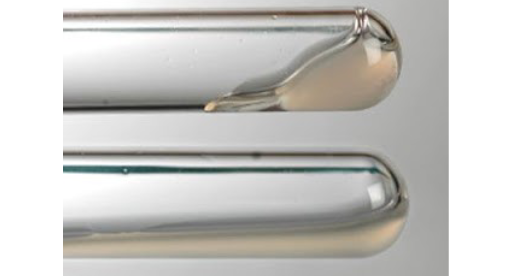
Manual PT: Tilt Tube
• Mix plasma and reagent and tilt tubes
• Examine visually for clot to form (based on the viscosity of the plasma mixed with reagent)
Automated PT
• Instrument monitors tube for change in optical density or electrical resistance and plasma viscosity
– End point fibrin clot
is affected by
colored plasmas
hemolyzed plasma
lipemic plasma
billirubin
turbing reagents
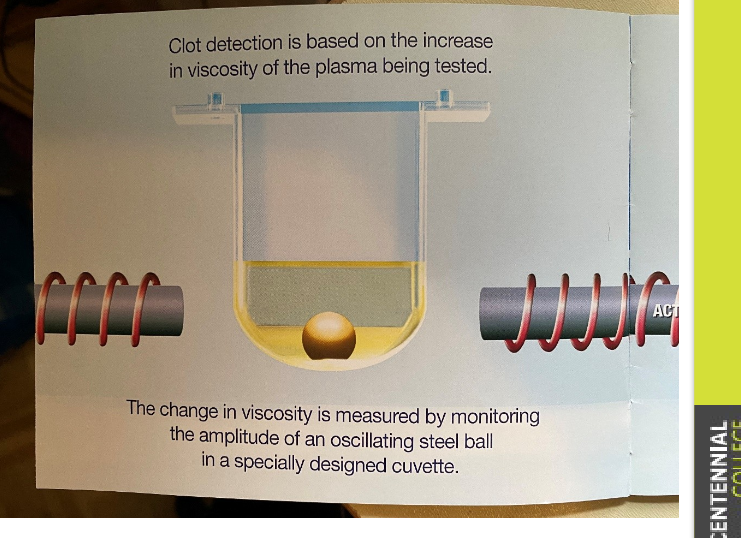
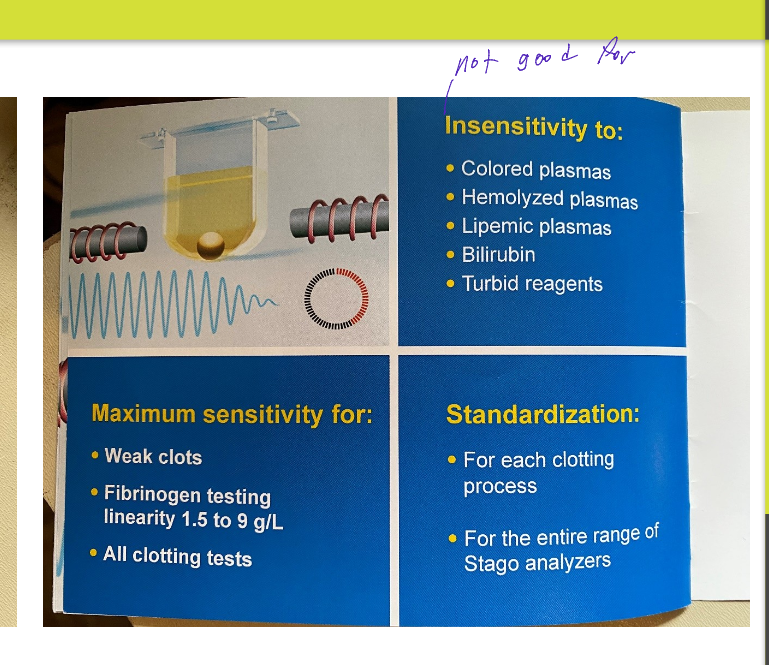
SEMI –AUTOMATED PT (Stago)
Viscosity based detection of clotting
using amplitude of oscillating steel ball in specialized cuvette
insensitive to and unaffected
colored plasmas
hemolyzed plasma
lipemic plasma
billirubin
turbing reagents
The increase viscosity is measured through the motion of a stainless steel ball
Constant pendulum swings of the ball are created by an electromagnetic field that is applied alternately on opposite sides of the cuvette by two independent driving coils
As soon as the plasma starts to clot (as of coagulation process being initiated by addition of the clot starting reagent),
the viscosity of the plasma starts to increase, and this change in plasma viscosity affects ball movement, slowing it down
•End product – solid clot
Result reporting of PT
PT, in sec, is converted to an International Normalized Ratio (INR)
INR (International Normalized Ratio)
is a way of standardizing the results of prothrombin time tests, regardless of the testing method
Helps the doctor to understand results in the same way even when they come from different labs and different test methods
treatment with blood-thinning medicine (anticoagulant therapy) will be standardized
In some labs, only the INR is reported and the PT (Sec) is not reported
Calculations for INR/ PT ratio
PT patient sec / PT mean normal cont. sec)ISI
ISI is specific to thromboplastin used
Normal Range of PT/INR
PT 10 - 14 sec
INR 0.8 - 1
Therapeutic Range of PT/INR (if comadin or heparin given)
PT 16 - 18 sec
INR 2 - 3
Critical Range of PT/INR
PT > 25 sec
INR > 4
abnormal prothrombin time is often caused by:
liver disease or by treatment with blood thinners
Some Drugs that can affect the PT result:
Aspirin, (decrease; double check)
Vit. K supplement (increase)
antibiotics
and the birth control pill
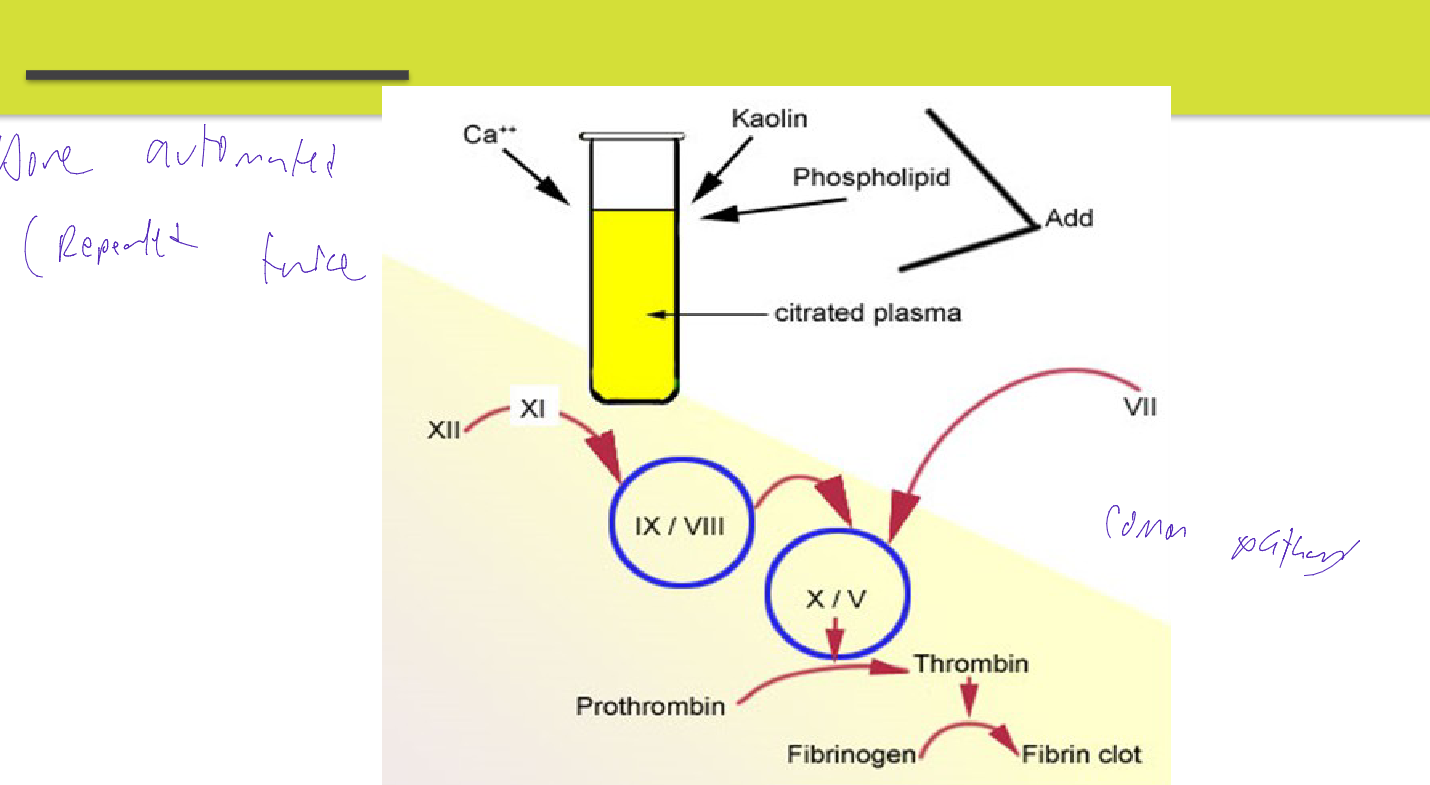
(Activated) Partial Thromboplastin Time, APTT or PTT
Used to monitor intravenous anticoagulant therapy (Heparin)
Specimen same as PT (3.2% Na Citrate - plasma)
If frozen (-200C or -700C), plasma should be thawed rapidly at 370C, then gently mixed and tested immediately
Mixing is critical before testing in order to resuspend proteins that may have been precipitated by freezing
• Most useful routine screening tests for the intrinsic pathway and common pathways
• Intrinsic pathway XII→XI→IX→VIII
• Common pathway →X→V→II→I
– (→these steps require Ca++)
• Used to monitor intravenous anticoagulant therapy (Heparin)
Testing for APTT or PTT
Two reagents
• Cephaloplasmin (phospholipid) with contact activator
• CaCl2
• Both reagents and specimen must be equilibrated for 5 minutes at 37ºC
• Cephaloplasmin (phospholipid) is added to the specimen and factor XII is activated after 3 minutes
– CaCl2 is added to complete the clotting cascade
done in dublicate
Normal Range PTT
25 - 35 sec
Therapeutic Range PTT
.5 to 2x normal control
Critical Value PTT
> 60 - 100 sec
Quality Control for PTT
Normal and Abnormal Control plasma must be run every 8 hours
Manual Duplicate results:
<40 sec: must be within ±2 seconds or repeat
>40 sec: must be within ±3 seconds or repeat
Source of Errors Associated with specimen
– Order of draw
– Inappropriate ratio of anticoagulant to blood
– Clotted, hemolyzed or lipemic samples
– <10,000 platelets x109/L (false high)
– Delay in testing or processing
– Inappropriate storage
Source of Errors Associated with storage
Incorrect preparation of reagents
– Failure to properly store reagents (or not warm them up)
– Use of reagents beyond reconstituted stability time or expiration date
– Contaminated reagents
Source of Errors Associated with procedure
– Incorrect temperature
– Incorrect incubation times (↑ incubation time = ↓PTT due to contact activation and > 5min heating will result in loss of heat-labile factor V)
– Incorrect volumes of sample, reagents or both
Automated Coagulation Instrument Maintenance
• Practice proper PPE
• Always wear non-latex examination gloves when performing
maintenance work or inspection
• Each instrument is different. Follow the specified manufactures tools and parts
Maintenance Schedule-of autmoated PT
Daily
• Probe cleaning reagent is cycled through the instrument –system maintenance menu
• Check consumables (cuvettes, etc.)
Weekly
• Clean sample area, reagent wells and light path
Monthly
Clean and replace filters, change waste containers
Instrument Calibration
• Six months or when QC is off (as needed)
Reagent Change
• As needed Controls
• Make fresh daily
Point of Care Coagulating Tests
defined as medical diagnostic testing performed outside the clinical laboratory in close proximity to where the patient is receiving care
typically performed by non-laboratory personnel and the results are used for clinical decision making
POCT devices are often ‘hand held’ or may be small portable analyzers
generally more expensive than in lab testing but is appropriate and cost effective in some clinical settings
Testing is performed near the patient and informs immediate decisions for clinical management of the patient
FAST TAT
Laboratory ensure program quality
Example POCT tests
blood glucose
urine dipsticks
blood gases
chemistry
hematology
coagulation
cardiac markers
pregnancy tests
Quality Assurance for Point of Care Test Operators
• Training for all POCT operators who perform Point-of-Care Testing (POCT)
• To meet accreditation standards POCT operators must be knowledgeable about the types of Point-of-Care Testing (POCT) they are responsible for
• POCT operators are accountable to complete training
• Training can be In house or online
• POCT operators have documented evidence of training
• POCT operators are qualified to perform their responsibilities and perform tests according to the manufacturer’s instructions to obtain accurate and reliable results.
• A Policies & Procedures Manual is available to POCT operators
• Assess POCT operator competency as per SOP and accreditation
Criteria for Result Reporting (general)
• Run QC for accuracy and precision
• Test results are reported only when all performance specifications for a test are within QC acceptable limits
• Remedial actions are taken and documented when required
• When instrument problems are detected, all patient results obtained since the last acceptable quality control run are evaluated to determine if they have been adversely affected
• Reported result include pertinent information required for interpretation
• Patient specimen is analyzed only after meter function checks are OK
• Calibrate the system for each new box of test strips
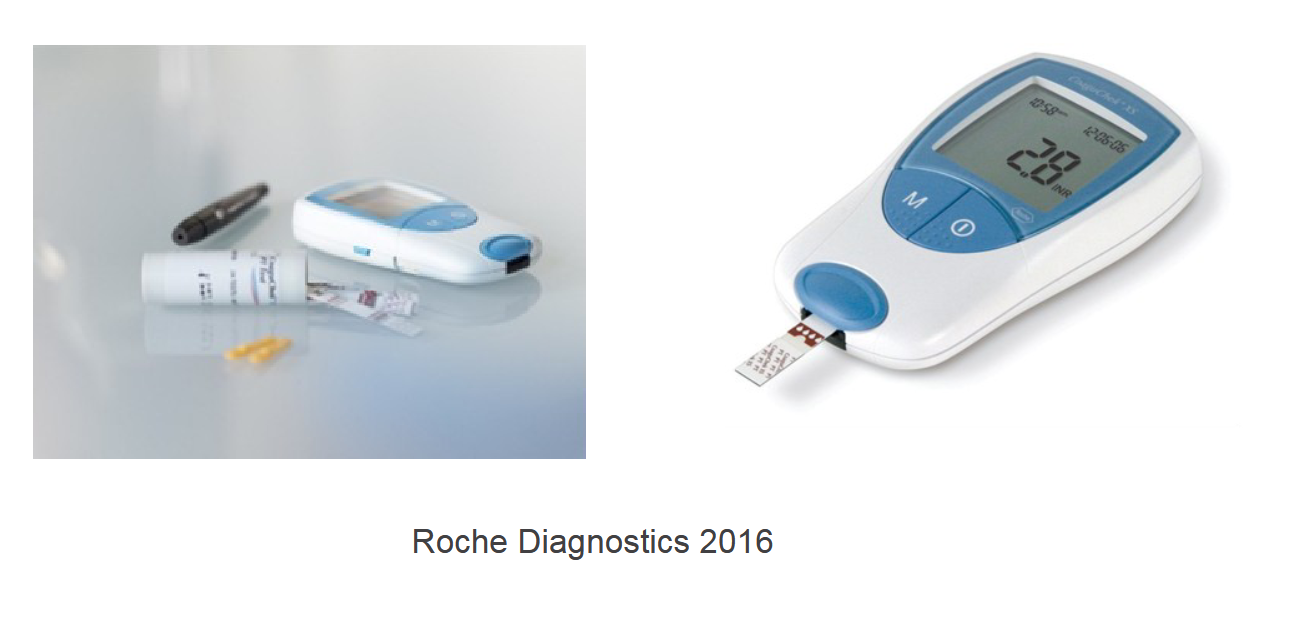
Example of a POCT coagulatin test→CoaguChek XS System
• PT/INR in one minute
• Finger-prick or venous sample (minimum 8 ul)
• Test strip has reagent and code
• A blood drop is applied within 15 sec of collection
• The meter starts the test and the blood mixe with the ingredients on the test strip
• When the meter determines that the blood has clotted, it stops the measurement and calculate the result
• Results are stored in the meter
• Battery operated
Safety Precaution
• All samples must be regarded as potentially infectious.
• POCT operators must follow PPE
Maintenance
Daily
• Check expiry date of strips
• Place the meter on a flat surface, free of vibrations
• Ensure that internal QC results are acceptable during testing.
• Follow the policies and procedures for collecting and handling
samples, testing patient samples, and reporting test results.
• Report or log patient tests result
• Clean and disinfect POC system
Monthly
• Review QA Checklist. Include all the actions associated with the erroneous result
Every 3- 6 Months
• Perform an external evaluation of accuracy, such as split sample testing or have two operators test the same patient and compare results
As Needed:
Train new POCT operators
QUALITY ASSURANCE (ASSESSMENT)
• QA involves the entire testing process including safety, personnel, specimen collection and handling, performing the test, recording results and finally reporting patient test results to providers
• Develop a corrective action plan and implement the corrections
• The QA process involves investigation, identification and resolution of any problems with subsequent development of policies that will prevent recurrence
• These new policies will be periodically reviewed to ensure the actions taken corrected the initial problem over time
Pre-analytic Errors
• Patient ID
• Sample collection
• Test Ordering
• Incomplete Requisition
• Leaving the test strip exposed to light for extended time
• Selecting the correct site
• Specimen accessing