Gait Alignment/Deviations TF
1/65
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
66 Terms
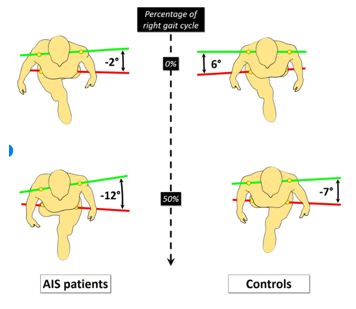
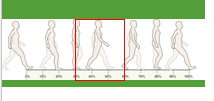
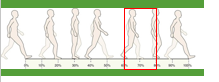
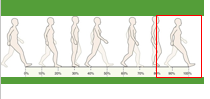
Pelvic Rotation
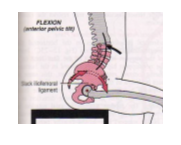
Pelvic tilt
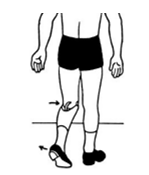
Knee and hip flexion
Knee and ankle interaction
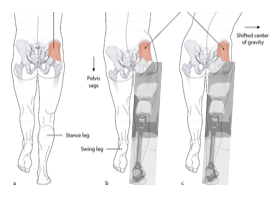
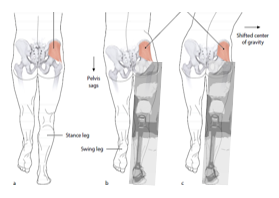
Lateral pelvic displacement
Determinants of gait
“Symptom”
What is observed
“Cause”
Patient/prosthetic gait problem
Goal in gait assessment
Attempt to match normal gait
What methods of assessment are available and which ones are clinically applicable?
Sound - use multiple senses
Feedback from patient
Force plates/sensors
Outcome measures - speed, time, TUG
Slow motion video capture - looking for specific phases of gait
Weak knee extensors results in
Foot slap at IC
Locked ankle results in
Knee buckling to allow HRF to move posteriorly
Where do you start making adjustments during static and dynamic alignment?
SOCKET
What do TF patients typically lose relating to gait?
Trunk rotation/arm swing
Applying force to ASIS, shifting weight into hand, allowing loading of the prosthesis
Transverse pelvic rotation
What does loading the prosthesis toe help with?
Weight distribution - helping with initiating knee extension and give them energy return
When would giving a patient stance flexion be justifiable?
When shock absorption is needed at IC
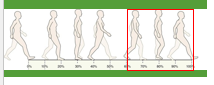
Name the different stance phase deviations
Foot slap
Foot rotation
Knee instability
Lateral trunk bending
Abducted gait
Delayed progression
Drop off
Unequal step length
Excessive lordosis
In someone who is not an amputee, when would foot slap occur?
If they have a weak tibialis anterior
Rapid plantarflexion to foot flat
Foot slap

Prosthetic causes for foot slap occurring
Prosthetic heel/bumper is too soft (articulated ankle)
When would a patient like having the foot slap deviation?
To provide stability in early stance, allowing the GRF to go anterior relative to the knee quicker for increased stability
Too hard of heel - long toe lever - locked ankle in an orthosis all lead to what?
Rapid knee flexion
External foot rotation in early stance - heel hits and instead of knee flexion the foot will rotate
Foot rotation

If you notice foot rotation at toe off, what could be the issue?
They can have too stiff of a toe lever
Prosthetic causes for foot rotation to occur
Prosthetic heel/bumper too firm
Shoe heel too firm
Socket rotation due to insufficient modification
Uncontrolled knee flexion in early stance - different than stance flexion
Knee instability

Causes for knee instability occurring from the patient
Weak hip extensors
Causes for knee instability because of the prosthetic
Insufficient socket flexion
Knee unit too far anterior
Foot in too much DF
Prosthetic heel (or shoe) too firm
Shoe heel height

Should the socket ever be extended?
NO
Bending toward prosthesis/affected side in stance
Lateral trunk bending
Patient causes for lateral trunk bending to occur
Short residual limb
Weak hip abductors - as this deviation takes weight off of the gluteus medius
Prosthetic causes for lateral trunk bending to occur
Px too short
Femur not stabilized laterally - could be that the lateral wall was not shaped, wide M-L dimension, insufficient socket adduction
Pain - ramus pressure or distal-lateral femur pressure

Prosthesis held away from midline (>4” BOS from the medial border of the heel)
Abducted gait
Patient causes for abducted gait to occur
Weak or contracted abductors
Poor balance, insecurity
Prosthetic causes for abducted gait
Prosthesis too long
Lateral wall not shaped
Pain in the ramus or distal-lateral femur pressure
If the patient is experiencing abducted gait, where should you start?
Try to fix first with a translation plate
Sensation of “walking uphill” during terminal stance
Delayed progression
Prosthetic causes for delayed progression
Toe lever too long - excessive PF or the foot too far anterior
Foot too far anterior
Foot category too high (too stiff)
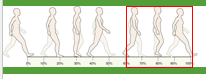
Sensation of “stepping in a hole” during terminal stance
Drop off

Prosthetic causes for drop off
Toe lever too short - foot too DF or socket too far anterior to knee/foot

How could drop off also appear as in gait?
Knee flexing too early in the gait cycle
What can cause unequal step length?
Patient cause - new patient, poor balance, insecurity
Prosthetic cause - insufficient socket flexion (same ideas as if the socket was extended, not giving the patient enough ROM), painful socket
Long prosthetic step, short sound side step
Unequal step length
How can you fix unequal step length?
Alignment and gait training
Pelvic motion used to increase step length
Excessive lordosid
What does excessive lordosis compensate for?
Weak hip extensors/abdominals
Patient causes for excessive lordosis
Weak hip abductors/abdominals
Hip flexion contracture
Prosthetic causes for excessive lordosis
Insufficient socket flexion
List the swing phase deviations
Medial/lateral whip
Uneven heel rise
Circumduction
Vaulting
Terminal impact
Foot moves in a medial or lateral arc - observe direction of heel in early swing
Medial/lateral whip
What direction will the trunk swing toward in a medial/lateral whip?
Swing toward the Affected side
Patient causes for a medial/lateral whip
Weak musculature or improper donning
Prosthetic causes for medial/lateral whip
Knee axis in excessive rotation
Socket fit - too tight/too loose
Medial whip
External rotation - hip stays toward midline
Lateral whip
Internal rotation - hip stays in midline
Name differences between medial/lateral whip and circumduction
Hip stays in normal midline for a whip while in circumduction it does not.
Circumduction - at the hip
Whip - at the knee
Heel rises too high and too quickly from initial to mid swing - opposite can also occur
Uneven heel rise
Patient causes for uneven heel rise
Forceful hip flexion
Prosthetic causes for uneven heel rise
Incorrect flexion resistance - friction/valve setting, programming (MPK)
Hip moves in a lateral arc (abduction and flexion) to provide clearance
Circumduction
Patient causes for circumduction
Lack of confidence to flex the knee
Prosthetic causes for circumduction
Prosthesis too stable (or locked knee)
Excessive extension bias (as many knees come with an extension assist)
Excessive resistance to flexion
Inadequate suspension
Prosthesis too long - limb position to the socket
What side will the trunk lean toward when patient circumducts?
Opposite/unaffected side
Excessive PF to provide clearance
Vaulting
Patient causes for vaulting
Habit
Prosthetic causes for vaulting
Px too stable
Excessive extension bias
Excessive resistance to flexion
Inadequate suspension
Prosthesis too long - needing extra clearance
Full extension forcefully achieved prior to IC (“clunk”)
Terminal impact
Patient causes for terminal impact
Habit/preference
Prosthetic causes for terminal impact
Insufficient knee friction
Excessive extension assist
Footwear - heel height and durometer
Limb volume - shrinking/swelling of residual limb, sock ply management
Improper donning - rotation
Patient fatigue
Patient motivation
Other considerations for gait deviations