Lec 10: Advanced Nutrition
1/36
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
37 Terms
nutrition def
science of optimal cellular metabolism and its impact on health and disease
list the main categories of nutrients
carbohydrates
proteins
fats
water
minerals
vitamins
what are some examples of primary and secondary prevention with nutrition
p=health eating, canada food guide, physical activity
s= screening (lipid, BG, BMI, waist circumference, obesity staging)
what are some examples of tertiary prevention with nutrition
dietary interventions=dietician, speech language pathology
enteral nutrition
parenteral nutrition
surgical intervention
pharmacology
what can we assess with nutrition
health history
BMI, calorie count
physical examination (including LOC, pain, nutrition)
safety - allergies
activity levels and ability to complete ADLs
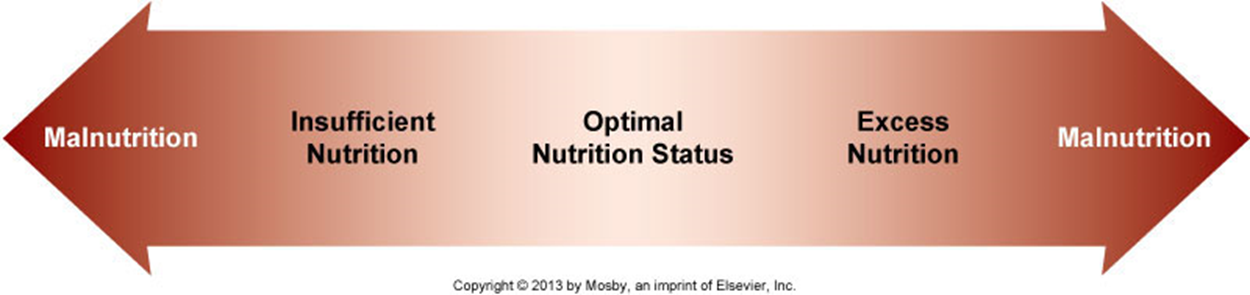
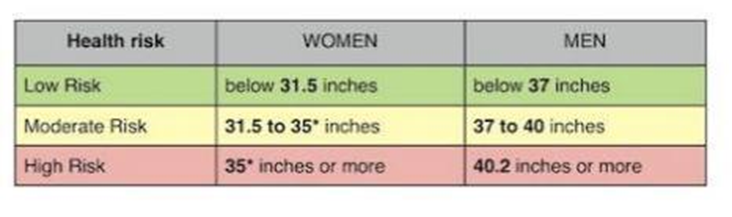
waist circumference normal parameters
women = <31.5 in
men = <37 in
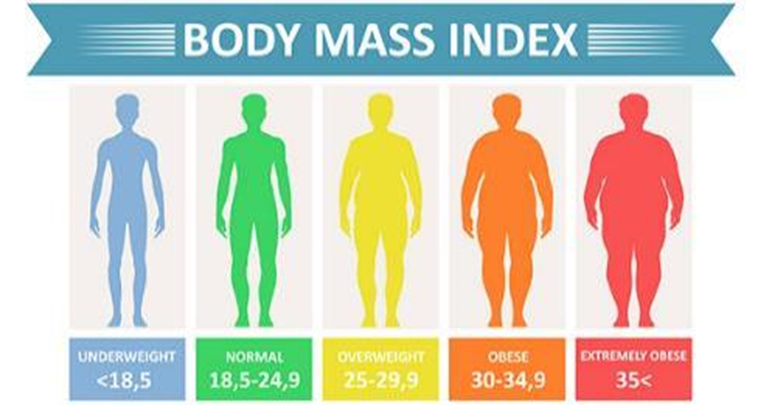
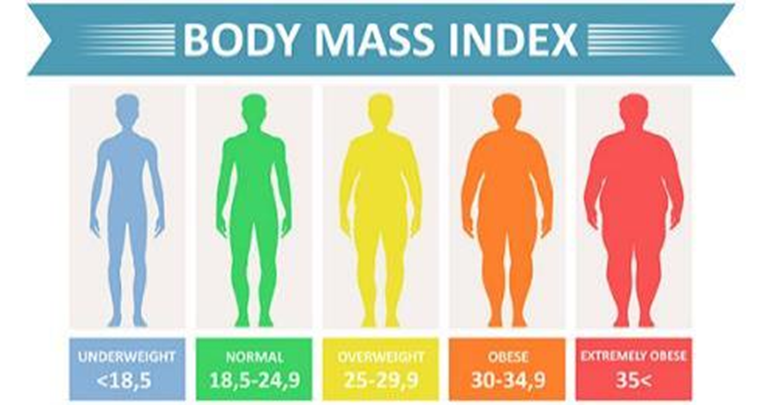
BMI ranges
underweight = <18.5
normal = 18.5-24.9
overweight = 25-29.9
obese = 30-34.9
what labs should we test for and their ranges
pre-albumin= 19-38 mg/dL or 190-380 mg/L
lipase (0-160 U/L)
amylase (23-85 U/L)
BG and hemoglobin A1C
lipid profile
electrolytes
hemoglobin and hematocrit
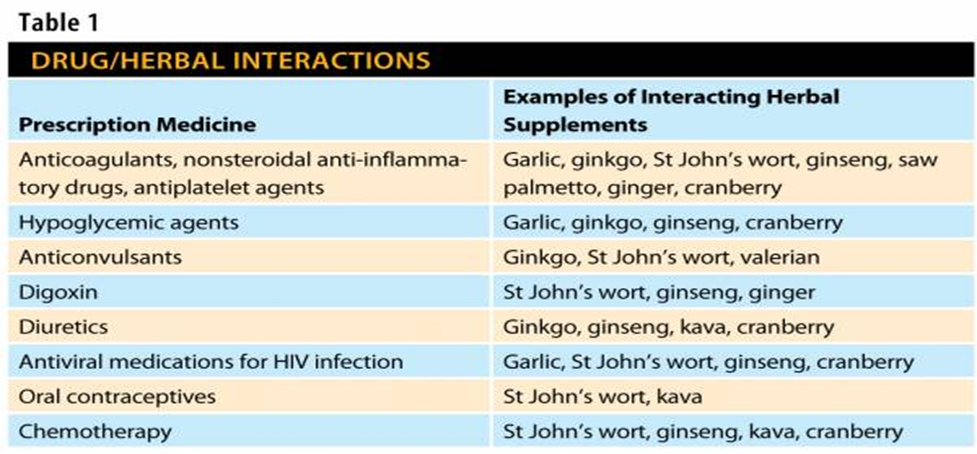
what are some pharmalogical interventions (supplements)
protein and nutrient supplements = ensure, nutrition bars
vitamin supplements = multivitamins, vit B, vit C, folic acid
mineral supplements = iron, calcium, magnesium, zinc
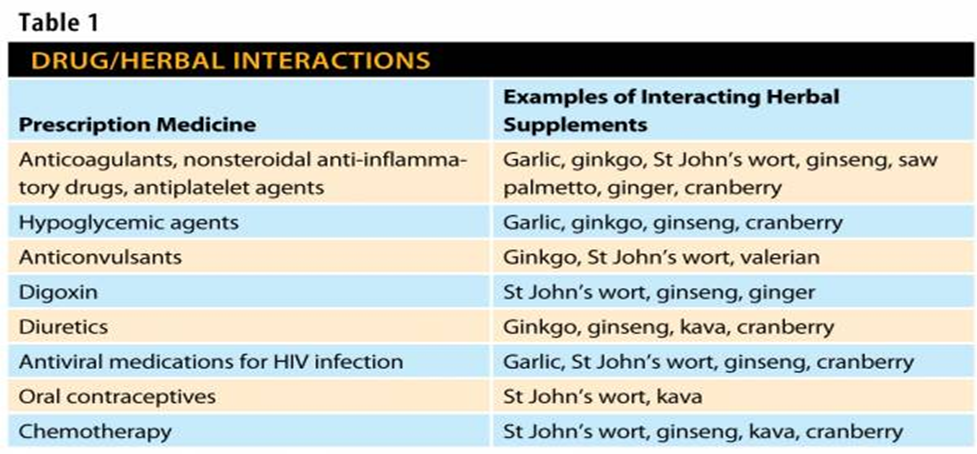
herbal and naturopathic remedies = omega 3 fish oil, glucosamine, ginseng, echinacea, st johns wort, garlic, etc
statins = atorvastatin, simvastatin
insulin or oral diabetic agents
Who needs advanced nutrition?
pts who are malnourished or are at risk for developing nutrition complications due to:
impaired oral intake (ex decreased LOC)
impaired digestion/absorption (ex gastric surgery)
increased metabolic demand (ex trauma and burns)
altered organ fx (ex end stage liver disease)
Screening process (what do we assess)
changes in weight
changes in oral food and fluid intake
past medical/surgical history
food allergies or following a special diet
diseases and conditions (short bowel syndrome, bowel obstruction, critically ill pts, and severe acute pancreatitis)
what are the major goals with nutrition tx
attaining an optimal level of nutrition
preventing infection
maintaining skin integrity
enhancing coping skills
adjusting to changes in body image
acquiring knowledge of and skill in self-care
preventing complications.
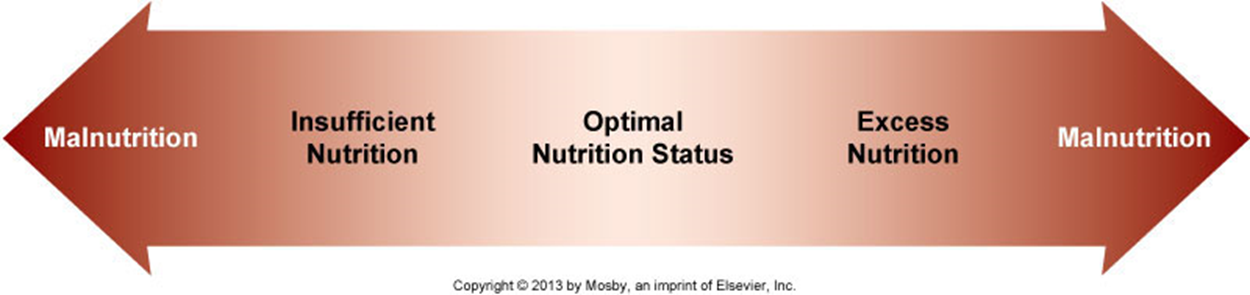
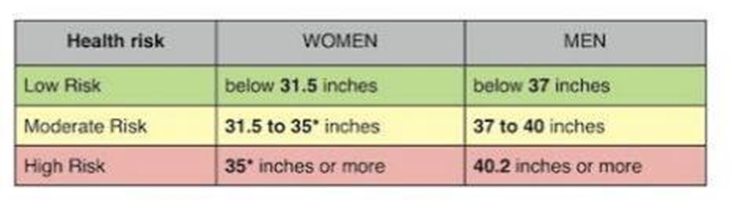
variations
pts unable to take in their total daily calories and protein in a typical oral form => they are at risk of being or are undernourished
who is enteral nutrition used for and def
pts with a functional GI tract that can be accessed
nutrition taken through a tube that goes directly to the stomach or small intestine
who is parenteral nutrition used for and def
malnourished pts that arent candidates for EN
a method of getting nutrition into the body through veins (through peripheral IV or central line)
enteral feeding def
meets nutritional requirements when oral intake is inadequate or not possible, but GI tract is functioning
feed formulas discarded after 24 hours
enteral feed pro’s
safe and cost-effective
preserves GI integrity
preserves the normal sequence of intestinal and hepatic metabolism
maintains fat metabolism and lipoprotein synthesis
maintains normal insulin and glucagon ratios
what forms of tubes are there with EN
nasogastric tube
percutaneous endoscopic gastrostomy (PEG) tube
what methods of EN are there
intermittent bolus feedings
intermittent gravity drip
continuous infusion
cyclic feeding
what do we need to monitor with EN
hydration
free water flushes every 4 to 6 hours
The Care of the Patient Receiving an Enteral Feeding, what to keep in mind
nutritional status and nutritional assessment
factors or illnesses that increase metabolic needs
hydration and fluid needs
digestive tract fx
renal fx and electrolyte status
medications that affect nutrition intake and function of the GI tract
compare the dietary prescription to the patient’s needs
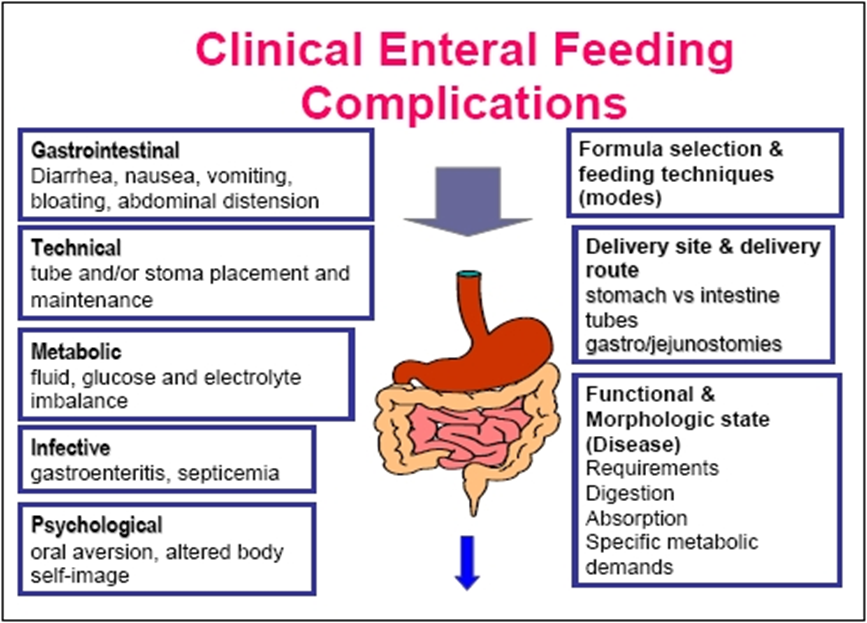
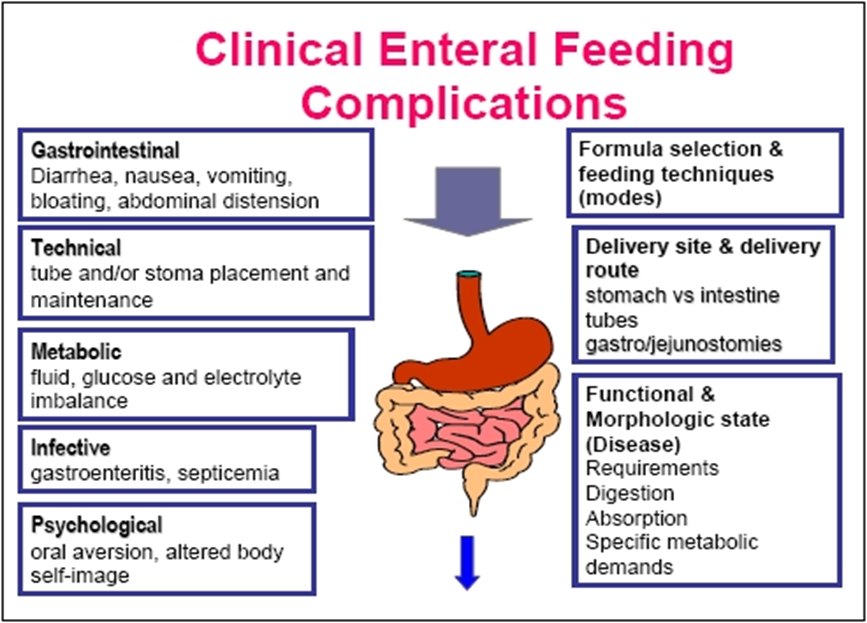
Enteral Feeding Complications
fluid/electrolytes=dumping syndrome, refeeding syndrome
glucose regulation
infection/inflammation/tissue integrity
gas exchange (on placement of NG tube, aspiration)
perfusion (hemorrhage)
pain with bloating/distension
elimination = N&V diarrhea, constipation
psychosocial (comfort, functional ability)
parenteral nutrition def
method to provide nutrients to the body by an IV route
how long should PN be done for once initiated
at least 7-14 days
who are the types of pts who cant be fed enterally or have intestinal failure but parentally
extended bowel rest
sepsis
head injury
burns
perioperative bowel rest
what are the diff methods for PN
total parenteral nutrition (TPN) - through a central IV line
peripheral parenteral nutrition (PPN) - through a peripheral IV line
PN characteristics
short term or long term
provides total or supplemental nutrition intravenously
caution needs to be used for critical ill, pediatric, and neonatal pts
Nurse’s role and responsibilities
nutrition/hydration status
electrolytes
S&S of hypoglycemia or hyperglycemia, monitor BG levels
assess for potential complications
VS including temp q4h or by protocol
measure weight
I&O
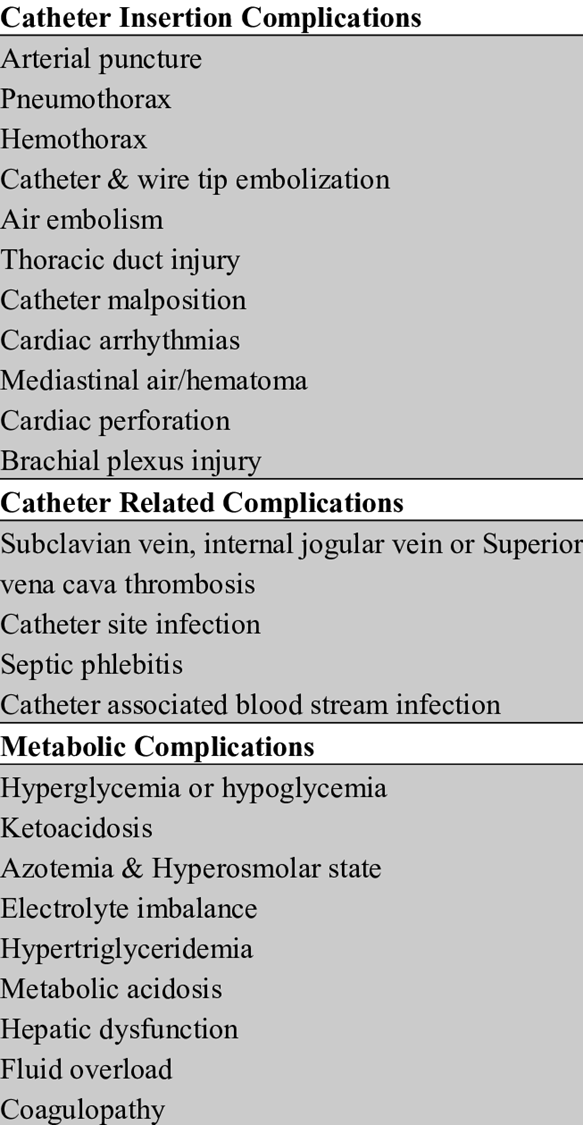
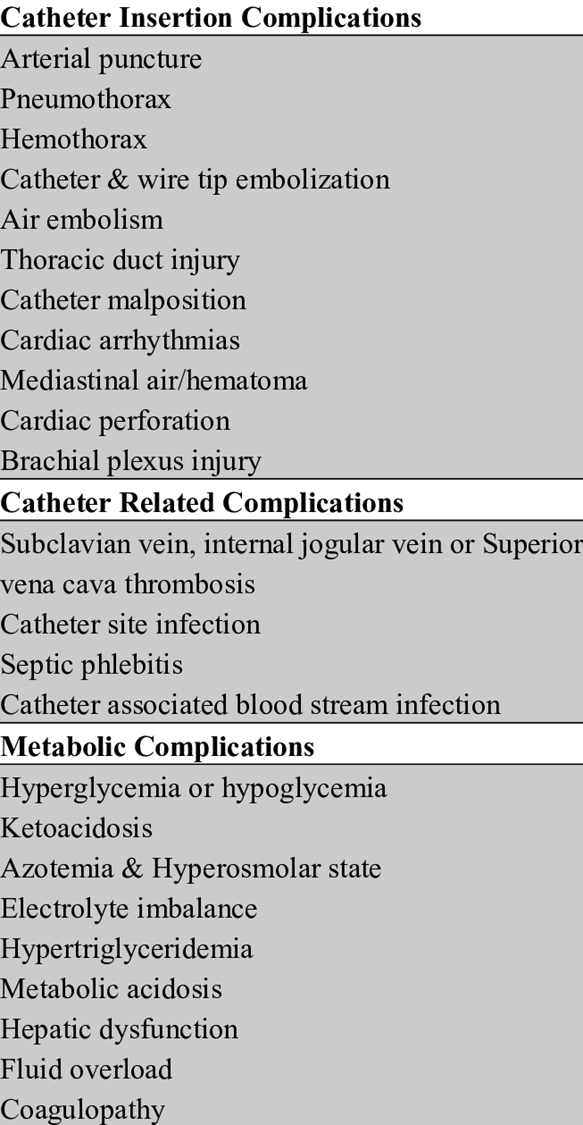
Parenteral Nutrition Complications
infection= culture and sensitivity of drainage at site or of infected IV catheter tip
gas exchange - air embolism, pneumothorax, hypercapnia
pt positioning for air embolism, chest tube for pneumothorax, ask for help
perfusion - catheter occlusion or dislodgement
glucose management = give D10W if pt disconnected from PN
acid base or electrolyte imbalance = consult doctor
fluid overload, azotemia = check BUN, urea, creatinine; meds for fluid overload, adjust admin rate
what are the key lab values for monitoring liver fx and their ranges
total bilirubin = <20 u/mol
albumin = 35-50 g/l
alanine aminotransferase (ALT) = <50 u/l
aspartate aminotransferase (AST) = 0-40 u/l
TOTAL BILIRUBIN [<20 UMOL/L] def
combo of unconjugated & conjugated
derived from the breakdown of RBCs
small amount is absorbed back into the blood then excreted by the kidneys and responsible for the yellow color of urine
elevated with obstruction to the flow of bile
ALBUMIN [35-50 G/L] def
protein produced by the liver and helps maintains the oncotic pressure in the vascular system
binds to substances (drugs, lipids, hormones, toxins) and converted to a water-soluble form by the liver
lack of this protein allows fluid to leak into the interstitial spaces
ASPARTATE AMINOTRANSFERASE (AST) [0-40 U/L] def
highest concentration within the liver and used to detect liver necrosis
comparison of the ratio of AST to ALT helps evaluate liver disease
with alcoholic cirrhosis, the AST is usually twice that of ALT
non-alcoholic fatty liver disease, the ALT is higher than AST
both enzymes rise before there are any signs of jaundice
what lab values are used to monitor renal fx and their ranges
blood urea nitrogen (BUN) = 2.5-8 mmol or 7-20 mg/dl
creatinine = 50-105 umol/l
BLOOD UREA NITROGEN (BUN) [2.5-8 MMOL/L OR 7 TO 20 MG/DL] def
waste product of protein metabolism and excreted by the kidneys
elevation can be an indication of renal failure or dehydration
over hydration and liver failure invalidate it as a test for renal failure
CREATININE [50-105 UMOL/L] def
end product of muscle metabolism
only condition where you see an elevation is damage to a large number of nephrons in the kidney
only increased when 1/4 of the nephrons are non-functioning
3 types of acute renal failure= pre, intra, post
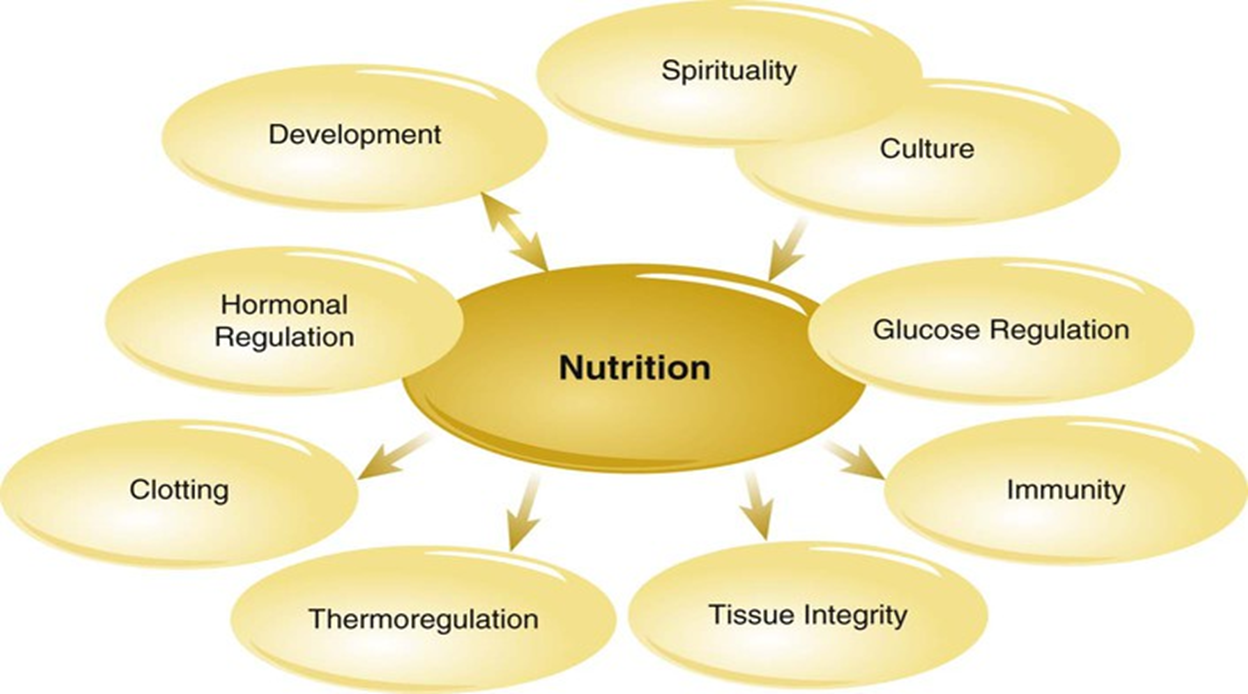
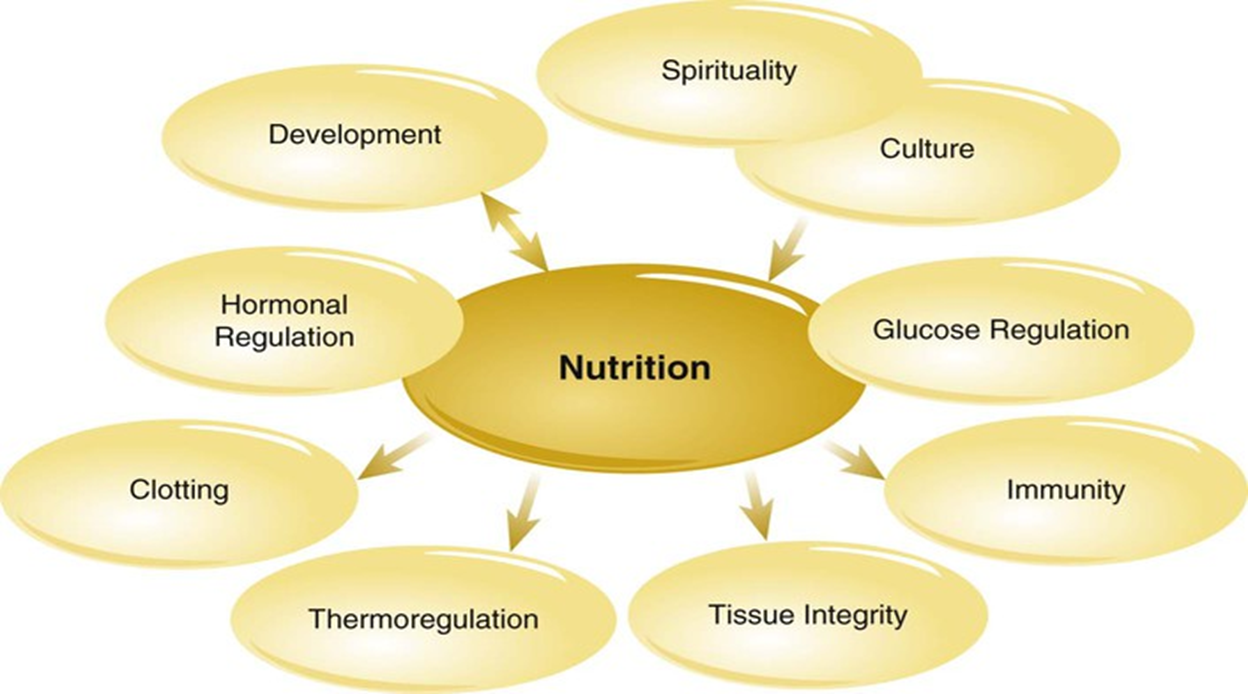
Interrelated Concepts pic