Advanced pain management
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
What is Nociceptive Pain?
Pain caused by an injury, physical pressure, or inflammation of some part of the body - Will usually respond well to opioids
What is Neuropathic Pain?
Pain caused by malfunction or damage to the nervous system. It is often described as a burning, tingling, or shooting sensation, and can be accompanied by numbness or a loss of sensation- Responds poorly to opioids so need to use adjuvants – Tricyclic Antidepressants/ Anti-Epileptics/ SNRIs/ Ketamine
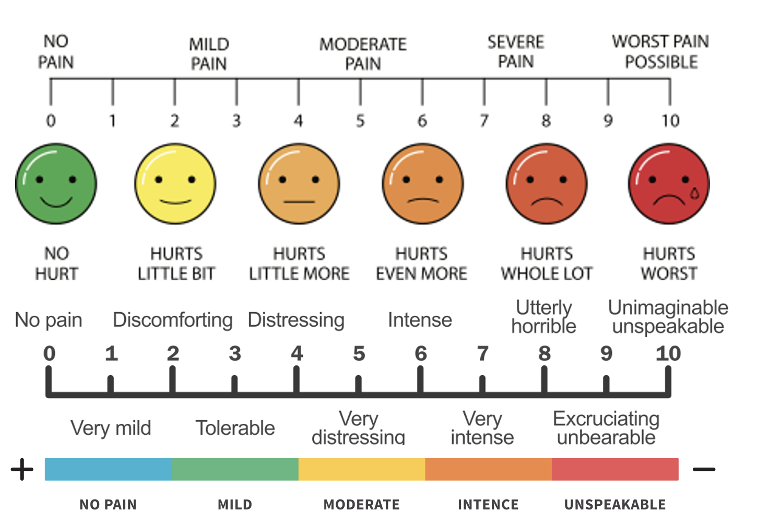
Visual Analogue Scale (VAS)
tool to assess pain intensity
VAS uses a scale from 0 (no pain) to 10 (worst pain imaginable) and can be used to assess pain over the previous 24 hours or over a longer time-period, such as the previous 7 days
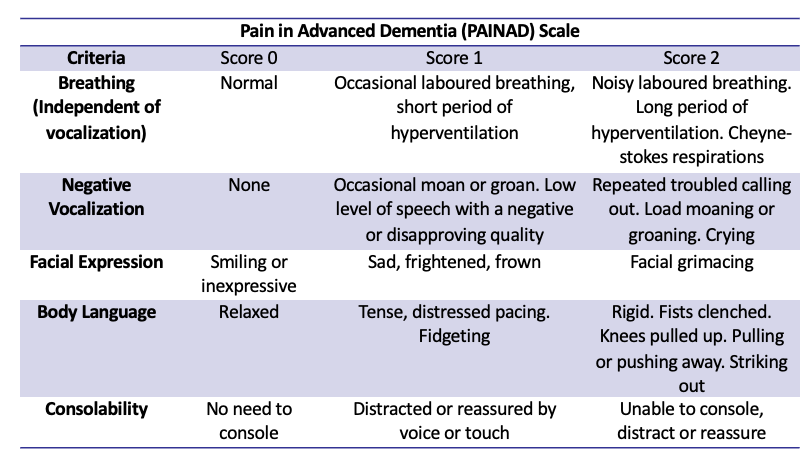
Pain in Advanced Dementia (PAINAD) Scale
Outline the acute pain analgesic ladder for adult patients.
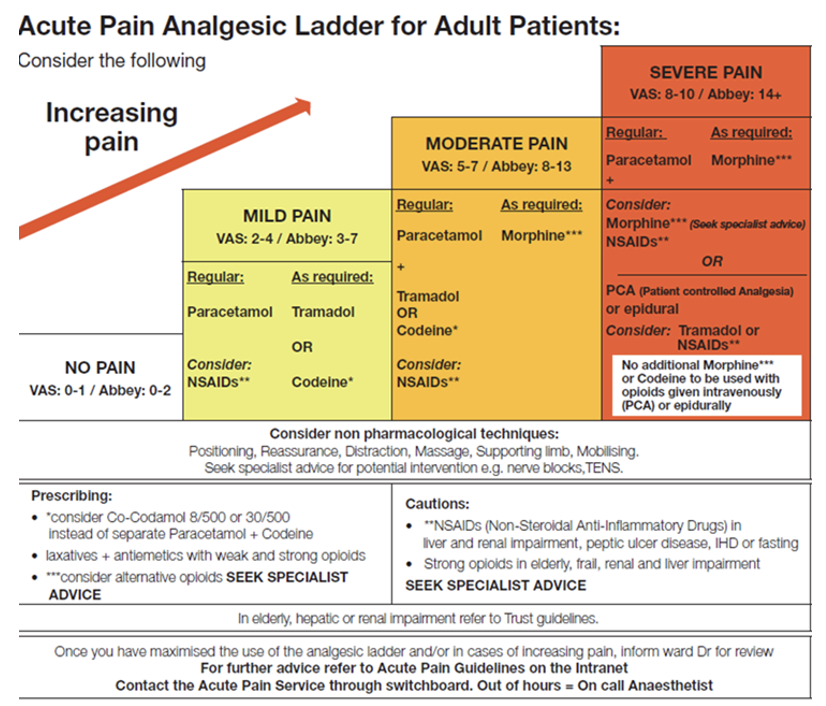
State the important information associated with Paracetamol
Mild to moderate pain
Analgesic and antipyretic
No anti-inflammatory effect
No major interactions
Adult dose 1g every 4-6 hours (Max 4g / 24 hours)
Hepatotoxic in overdose
In adults, single doses above 10 grams or 200 mg/kg of bodyweight, whichever is lower, have a reasonable likelihood of causing toxicity
State the important information associated with Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
Most common: Ibuprofen, Naproxen, Diclofenac , Aspirin
Others: Celecoxib, Etodolac, Etoricoxib, Ketoprofen, Mefenamic acid, Meloxicam, Piroxicam
Mild to moderate pain
Inhibit PG synthesis (inflammation pathway)
Inhibit thromboxane synthesis (blood clotting pathway)
Analgesic, antipyretic and anti-inflammatory
The lowest effective dose of NSAID should be prescribed for the…
shortest period of time to control symptoms.
All NSAID use can be associated with a small increased risk of…
thrombotic events independent of baseline cardiovascular risk factors or duration of NSAID use; however, the greatest risk may be in those receiving high doses long term.
What considerations should be made when giving Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)?
Use the lowest dose, for the shortest duration.
Increase risk for arterial thrombotic events
Consider the need for gastroprotection
Use with caution in the elderly
What contraindications and cautions are associated with Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)?
History of hypersensitivity or allergy to NSAIDs or aspirin
Severe hepatic, renal and cardiac failure
History of upper GI bleeding/ perforation linked to NSAID use
Active or previous acute peptic ulcer
Last trimester of pregnancy
Concurrent use with other NSAIDs / Aspirin at analgesic doses/ Anticoagulants (DOACS, Warfarin/Heparin)
State the adverse effects of Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
Dyspepsia and other UGI complication
Renal failure
Prolonged bleeding
Bronchospasm
Allergies reactions such as rashes, wheezing, throat swelling
May aggravate asthma
Cardiovascular events (MI, stroke, heart failure, hypertension)
Fluid retention and oedema
State the important information associated with Codeine
8mg, 15mg, 30mg, 60mg QDS
Approx. 10% of people are poor metabolisers due to a CYP2D6 deficiency cannot convert Codeine into Morphine
Commonly cause constipation by inhibiting peristalsis. Can also be used to treat diarrhoea
60mg QDS = 25mg morphine a day
State the important information associated with Dihydrocodeine
30mg QDS
Reliably metabolised and eliminated (only safe weak opioid in breast feeding )
Is similar strength to codeine but doses above 30mg provide little extra analgesia but increase adverse effects
30mg QDS = 12.5mg morphine a day
State the important information associated with Tramadol
Moderate to severe pain
It has noradrenaline and serotonin effects as well as opioid analgesic (Mu receptor)
Use in renal impairment = 50mg TDS and titrate
When should you AVOID Tramadol?
Uncontrolled epilepsy
Acute intoxication with alcohol/ hypnotics/ analgesics
Head injury
MAOIs: tranylcypromine/ phenelzine/ isocarboxazid/ moclobemide – as can lead to serotonin syndrome
When should Tramadol be used in CAUTION?
SSRIs: citalopram/ escitalopram/ fluoxetine/paroxetine/ sertraline (serotonin syndrome)
Current or history or mental health disorder/ substance abuse
State the important information associated with Morphine
If needing lots of PRN doses, then the need for regular MR dosing must be considered and reviewed regularly
Morphine liquid 10mg/5ml contains high levels of sugar and 10% alcohol
IR tablets - Sevredol
Oral dispersible morphine: 1.25mg/ 2.5mg/ 5mg/ 10mg/ 20mg - Actimorph
Actimorph is a Schedule 2 controlled drug - useful for patients who may struggle to measure out low doses of morphine liquid
State the important information associated with Oxycodone
Oxycodone is sometimes tolerated when morphine is causing excess sedation, nausea and or hallucinations.
More expensive but tends to produce less side effects, slightly less effect on GI tract
Used in preference to morphine, if the patient has a worsening renal function
State the important information associated with Gabapentin
Gabapentin is an option for peripheral neuropathic pain and may have a role in supplementing other forms of pain relief
In 2019, gabapentin was reclassified as Schedule 3 under the Misuse of Drugs Regulations 2001
The MHRA published guidance on prescribing gabapentin due to the growing concern of abuse. When prescribing gabapentin, patients should be evaluated carefully for a history of drug abuse (for example, through the use ofscreening tools) and dependence before prescribing
Patients on gabapentin should also be observed for possible signs of abuse and dependence and ensure that patients are aware of the risk of potentially fatal interactions with other medicines that cause central nervous system and respiratory depression, particularly opioids and alcohol
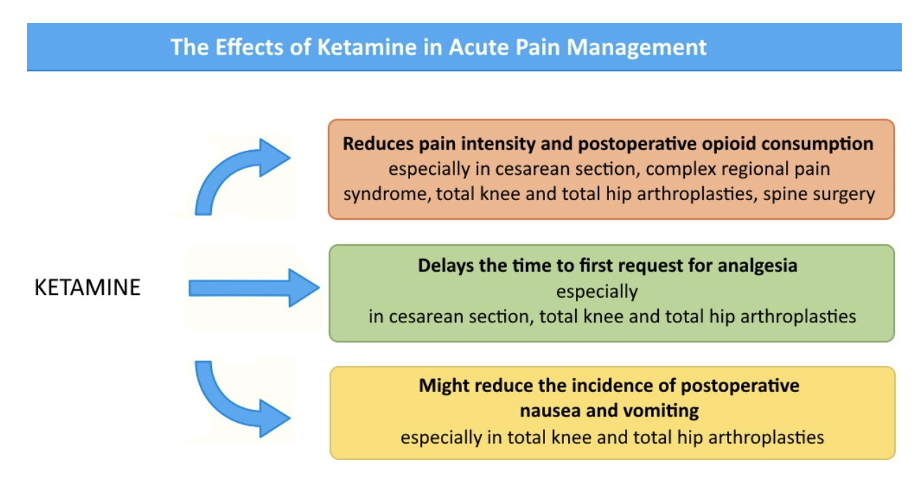
State the important information associated with Ketamine
The inclusion of ketamine may be effective in patients with escalating opioid requirementsbut the benefits of its use offset by dose-dependent adverse effects, including hypersalivation, nausea and vomiting and psychotomimetic effects
Give some examples of of Goals of Acute Pain Management
Post-Operatively: DrEaMing (Drinking, Eating and Mobilising) has gained prominence. DrEaMing is now one of the 5 Perioperative Quality Improvement Programmes (PQIP) priorities. It is now recommended not to treat according to pain intensity and attempt to remove all pain, but to promote DrEaMing
Opioid tolerance is more likely to occur in patients managed on…
doses of 60mg oral morphine equivalent (OME) and higher
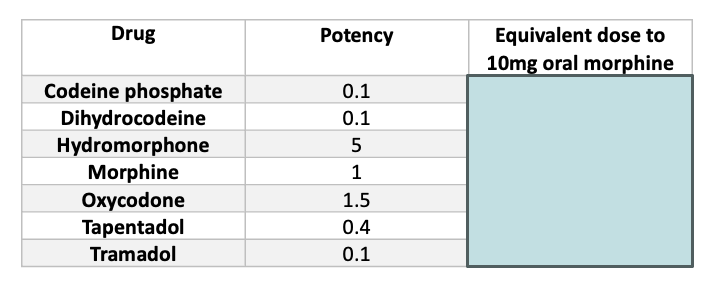
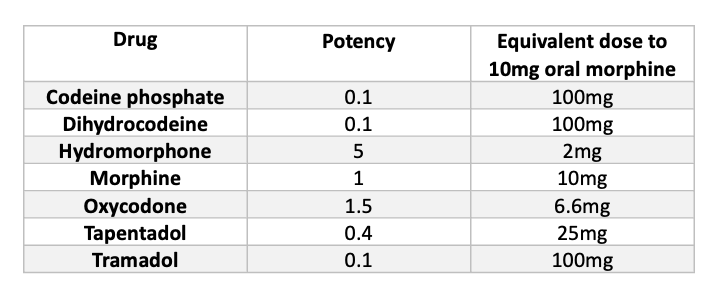
Fill in the following table for Oral Morphine Equivalent (OME).
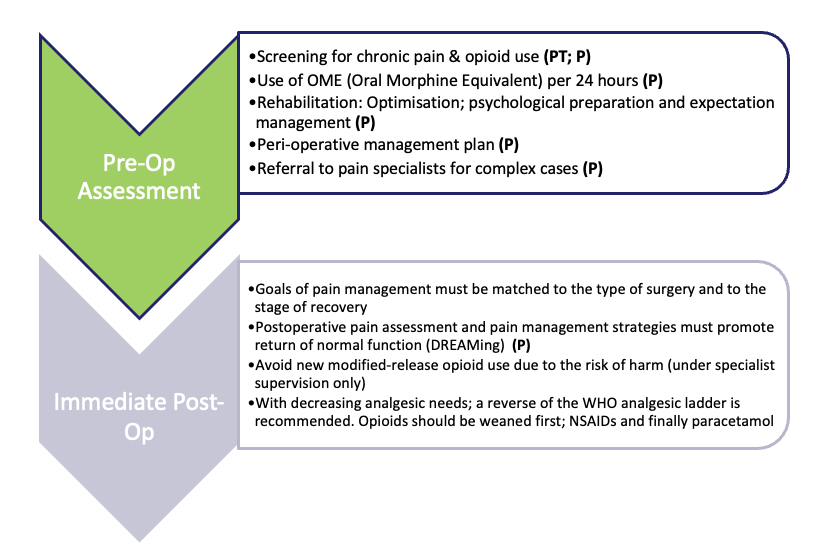
What is the best practice for pharmacy teams pre and immediate post operation?
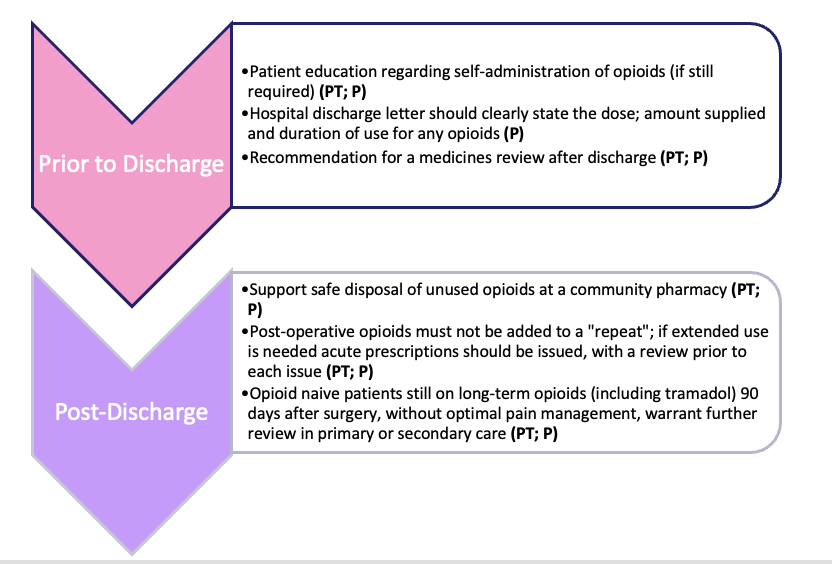
What is the best practice for pharmacy teams prior and post discharge?
What are the different types of Non-Pharmacological Management for chronic pain?
Non-pharmacological measures have the advantage of being low cost and relatively easy to implement
Physical application – transcutaneous electrical nerve stimulation (TENS); acupuncture and heat or cold packs
Physical activity – light or moderate exercise; deep breathing
Spiritual and psychological – meditation; praying; visualisation; cognitive behavioural therapy (CBT)
Distractions – conversations; music; TV
Effective patient education and a multidisciplinary approach is also thought to improve post-operative pain management