Stroke
1/71
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
72 Terms
Why is it important to determine if a patient's stroke is cardioembolic vs non-cardioembolic?
-It determines appropriate secondary prevention treatment with antithrombotics
-it determines WHEN secondary prevention treatment with antithrombotics can be initiated
What are examples of Atherosclerotic Cardiovascular Disease (ASCVD)?
Stroke
Transient ischemic attack
Stable or unstable angina
Acute coronary syndromes
History of MI
Arterial revascularization
Peripheral arterial disease
What are examples of nonmodifiable risk factors for stroke?
Age
Race
Sex
Low birth weight
Genetic factor
What are examples of modifiable risk factors for stroke?
Hypertension
Cigarette smoking
Diabetes
Dyslipidemia
Atrial fibrillation
Poor diet
Obesity
Physical inactivity
Asymptomatic carotid stenosis
Sickle cell disease
Other CV disease
What agent is used for the primary prevention of stroke?
Low dose aspirin (81 mg)
What is the USPS Task Force recommendation for the primary prevention of stroke in 40-59 year olds with a >10 year CVD risk?
81 mg aspirin for those who are NOT at an increased risk for bleeding
Consider stopping at age 75
What is the USPS Task Force recommendation for the primary prevention of stroke in >60 years with a >10 year CVD risk?
Recommends against initiating low dose aspirin
What is the clinical presentation of a stroke?
Weakness on one side of the body
Inability to speak
Visual impairment
NIHSS score interpretation of 1-5?
Minor stroke
NIHSS score interpretation of 6-15?
Moderate stroke
NIHSS score interpretation of 16-20?
Moderate-severe stroke
NIHSS score interpretation of 21-42?
Severe stroke
What is the reccomended thrombolytic therapy if patient meets criteria?
Alteplase
Tenecteplase
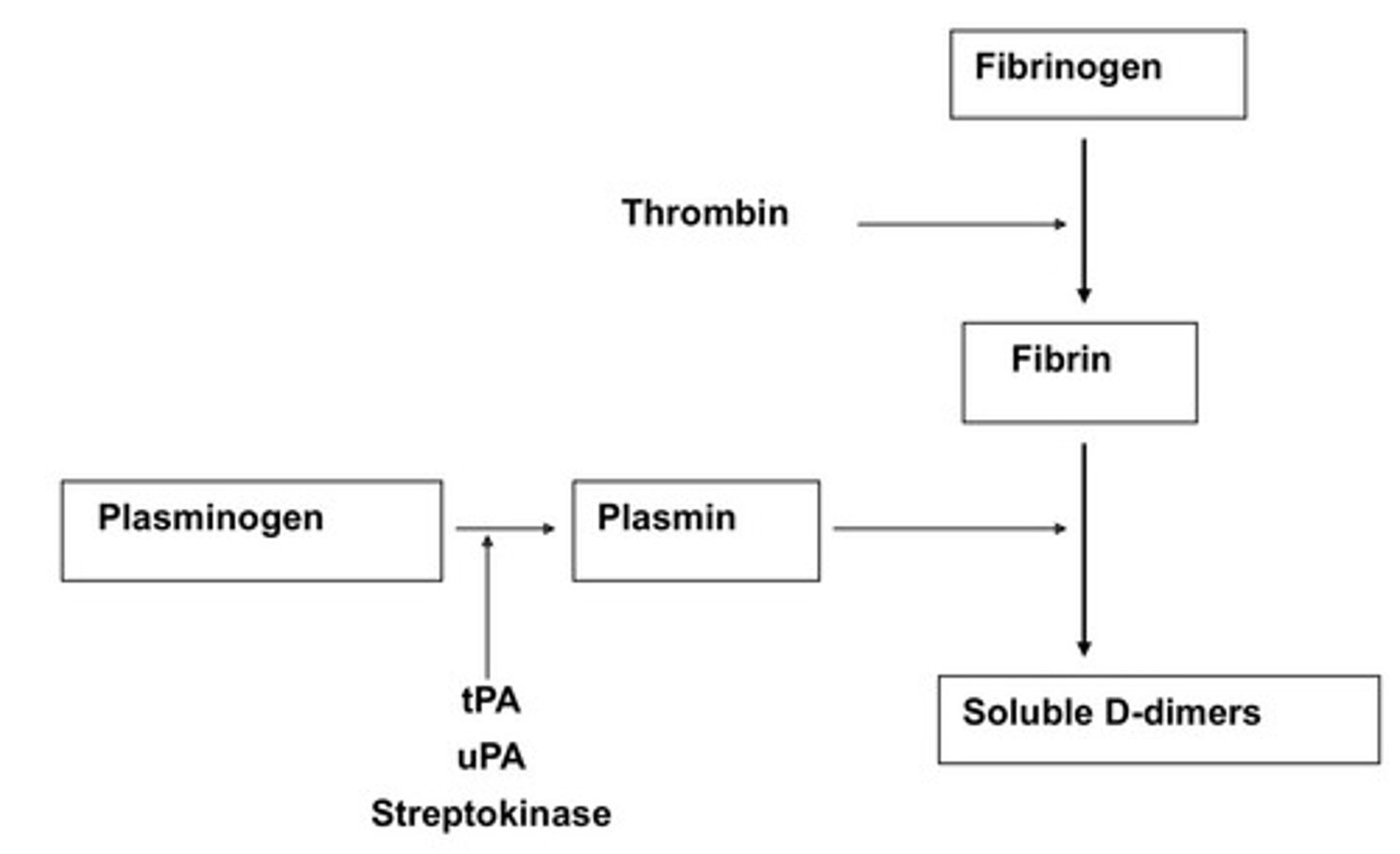
What is the MOA of tPA?
Initiates local fibrinolysis by binding to fibrin in a thrombus and converting entrapped plasminogen to plasmin
What is the dose of alteplase?
0.9 mg/day (max 90 mg) with 10% of the dose given as a bolus over 1 minute
Remainder of the dose is given over 1 hour
What is the dose of tenecteplase?
0.25 mg/kg (max 25 mg) single rapid IV bolus
Why does tPA have extensive exclusion and inclusion criteria?
Increases risk for major bleeding
Are thrombolytics indicated in mild non-disabling strokes presenting within 4.5 hours of symptom onset?
No -
Not superior in improving functional outcomes compared to double
antiplatelet treatment (DAPT)
What is the criteria for tPA?
Clinical diagnosis of tPA
Noncontrast CT scan reading
Time frame within 4.5 hours
Blood glucose before initiation
CI in INR >1.7, aPTT >40s, platelets < 100,000
Past medical history CI
Current medications CI
BP <185/110 mmHg
Why is there a tPA criteria for a clinical diagnosis and CT or MRI brain imaging?
To rule out a cerebral hemorrhage
Why is there a tPA criteria for a timeframe of 4.5 hours of symptom onset?
Faster treatment improves functional outcomes
Treatment should be initiated as quickly as possible
Why is there a tPA criteria for a blood glucose reading before intiation?
To rule out hypoglycemia as it could present as similar symptoms
Why is there a tPA criteria for specific coagulopathie labs?
To prevent bleeding
What are the past medical history contraindications in tPA?
Traumatic brain injury <14 days
Neurosurgery <14 days
Spinal cord injury within 3 months
Infective endocarditis
Severe coagulopathy
Aortic arch dissection
Intracranial neoplasm
What are the current medications contraindication in tPA?
LMWH (if full treatment dose received within 24 hours)
DOAC (relative contraindication if received within 48 hours)
What is the BP threshold to initiate tPA?
Lower BP to <185/110 mmHg before initiating to prevent converting to a intracranial hemorrrhage
What agents can be used to lower BP to <185/110 mmHg?
IV Labetalol
IV Nicardipine
IV Clevidipine
What is the BP monitoring required during tPA administration?
Every 15 min during & after IVT for 2 hours
Every 30 minutes for 6 hours
Every hour for 16 hours
What is the follow-up CT requirement for tPA administration?
Follow up CT or MRI 24 hours after IVT
Obtain before starting anticoagulants or antiplatelet agents
When is aspirin indicated for acute stroke treatment?
When a patient is ineligble for tPA
If a patient receives tPA (generally) withhold aspirin for at least _____ to reduce the risk of hemorrhage?
24 hours
When is aspirin + clopidogrel (DAPT) indicated?
Minor noncardioembolic ischemic stroke (NIHSS ≤3) or TIA
When should DAPT be initiated in a minor noncardioembolic stroke?
Initiate within 24 hours of symptom onset
How long should DAPT be continued in a noncardioembolic stroke?
Continued for 21 days followed by single anti-platelet therapy
Can DAPT be given in patients who received IV thrombolysis?
No
What is the acute BP management for non-tPA candidates?
If BP > 220/110 mm Hg, lower BP by 15% during the first 24 hours
What is the supportive care oxygen requirement?
Supplemental oxygen to maintain oxygen saturation >94%
What is the supportive care hyperthermia requirement?
Temperature >100.4°F should be treated with antipyretic medications
What is the supportive care hyperglycemia requirement?
Treat blood glucose to achieve 140-180 mg/dL
What are the VTE prophylaxis options for stroke patients?
Unfractionated heparin (UFH) 5000 units SC BID or TID
Enoxaparin (LMWH) 40 units SC daily
Fondaparinux 2.5 mg SC daily
Rivaroxaban 10 mg PO daily
What VTE prophylaxis agent should be used if impaired mobility?
UFH or LMWH
Should compression socks be used for VTE prophylaxis in stroke patients?
No - they cause harm!
What is secondary prevention for non-cardioembolic stroke patients?
Lifelong antiplatete therapy
What are antiplatelet options for a noncardioembolic stroke?
Aspirin 50 - 325 mg PO daily
Dipyridamole ER 200 mg + aspirin 25 mg PO BID
Clopidogrel 75 mg PO daily
Antiplatelet monotherapy after 21 days of ASA + clopidogrel
Can DAPT be used for >90 days?
No!
Continuous use of DAPT for >90 days or the use of triple antiplatelet therapy is associated with excess risk of hemorrhage.
What is the antiplatelet therapy for a intracranial large artery atherosclerosis with 50-99% stenosis?
Aspirin 325 mg daily is preferred to warfarin
Clioztisol 200 mg daily might be considered in addition to aspirin
What is the antiplatelet therapy for a intracranial large artery atherosclerosis with 70-99% stenosis?
90 days of ASA + clopidogrel is reasonable
What is the MOA of ciloztisol
Inhibitors of phosphodiesterase III to increase cyclic AMP
Reversible inhibition of platelet aggregation
Vasodilation
Inhibition of vascular smooth muscle cell proliferation.
If you have a stroke when you already taking aspirin should you increase the aspirin dose?
Effectiveness of increasing the dose of aspirin not well established
What MUST you obtain before starting antiplatelet or anticoagulant?
A follow-up CT or MRI scan at 24 hours after IV tPA
When can home BP medications be resumed post stroke?
After neurologic stability- 48-72 hours
What is the BP goal to reduce the risk of a recurrent stroke and vascular event?
<130/80 mmHg
What are the lipid goals for a very high risk patient?
>50% reduction in LDL-C
Target LDL-C <55 mg/dL
What are the criteria for a very high risk patient?
At least 2 major ASCVD events or 1 major ASCVD event and at least 2 high-risk conditions
What are major ASCVD events?
ACS within past 12 months
History of MI
History of ischemic stroke
Symptomatic PAD
What are high-risk conditions?
Age >65
Coronary bypass or percutaneous intervention (PCI)
Current smoker
Diabetes
Hx of congestive HF
Hypertension
LDL-C >100 mg/dL despite maximally tolerated statin + ezetimibe
What are the lipid goals for a patient not at very high risk?
>50% reduction in LDL-C
Target LDL-C <70 mg/dL
What is a cardioembolic stroke?
Blood stagnates in dysfunctional
atrium
Thrombus forms in left atrium
Thrombus then has potential to leave left atrium and cause embolic CVA
What is used to evaluate the annual stroke risk in atrial fibrillation patients?
CHA2DS2-VASc
What does "C" mean and how many points is it?
C = Congestive Heart Failure/Left Ventricular Dysfunction (1 point)
What does "H" mean and how many points is it?
H = Hypertension (1 point)
What does "A" mean and how many points is it?
A = Age > 75 (2 points)
What does "D" mean and how many points is it?
D = Diabetes mellitus (1 point)
What does "S" mean and how many points is it?
S = Stroke/TIA/thromboembolism (2 points)
What does "V" mean and how many points is it?
V = Vascular disease (prior MI, PAD, or aortic plaque) (1 point)
What does "A" mean and how many points is it?
A = Age 65-74 (1 point)
What does "Sc" mean and how many points is it?
Sc = Sex category (female) (1 point)
CHA2DS2-VASC score of >2 male or >3 female
Anticoagulation
CHA2DS2-VASC score of 1 male or 2 female
Anticoagulation is reasonable
What is secondary prevention in cardioembolic strokes?
DOACs (Apixaban, Dabigatran, Edoxaban, Rivaroxaban)
Warfarin
What secondary prevention in cardioembolic stroke is perferred?
DOACs
When should anticoagulation be initiated in cardioembolic stroke?
2-14 days after stroke to prevent bleeding