Assistive Technology Lesson 4: Assistive Devices
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
55 Terms
Assistive Devices
Provides additional means of support
Increases base of support
● parallel bars
● walker
● crutches
● canes
Most commonly used ad in rehabilitation
Full weight-bearing (FWB)
There are no restrictions on weight-bearing;
100% of body weight can be borne on the LE
Non–weight-bearing (NWB)
• No weight is borne on the involved limb; foot/toes make no contact with floor/ ground surface.
Partial weight-bearing (PWB)
Only a portion of weight can be borne on the extremity; sometimes expressed as a percentage of body weight (e.g., 20% or 50%)
Toe-touch weight-bearing (TTWB) or touch-down weight-bearing (TDWB)
Only the toes of the affected extremity contact the floor to improve balance (not to support body weight)
Weight-bearing as tolerated (WBAT)
Weight-bearing is limited by patient tolerance of weight borne on extremity
PARALLEL BARS
for patient instruction in a gait pattern
for practice
relative safety
WALKERS
To improve balance
To relieve weight bearing either fully or partially on a LE
Affords the greatest stability
Provide a wide BOS
Improve anterior and lateral stability
Allows UE to transfer body weight to the floor
Glides
part of the walker thats small, plastic attachments placed on the POSTERIOR legs in combination with wheels on the front legs
Smooth forward progression without having to lift with each steps
ALTERNATIVE: tennis balls
Folding Mechanism
part of the walker thats for patients who travel
Collapse to fit in a car or storage
HANDGRIPS/HANDLES
part of the walker that’s for enlarge and molded handgrips available for px with arthritis
Some with second set of handles to assists with sit to stand
WHEEL ATTACHMENTS
“Rolling Walkers” •
Either 2 infront or all 4 legs with wheels •
For px who are unable to lift a conventional walker •
Swivel wheels / fixed wheels •
3”, 5”, 6” diameter
Altered weight bearing status bawal dito kasi may wheels
TRIPOD ROLLING WALKER
Type of walker thats
Tripod design
Rollators
Ease in maneuverability and turning
Folds
Height adjustment through handles
STORAGE ATTACHMENTS
part of the walker thats only for essential items
May create excessive anterior load -> safety hazard
SEATING SURFACE
part of the walker thas for px with limited endurance
Community ambulators who require periodic rest
Measurment of Walkers
Top of the ___at the level of the greater trochanter
Elbow should be flexed between 20-30 degrees
Full Weight Bearing Gait Pattern (walker)
What gait is
1. The walker is picked up and moved forward about an arm’s length.
2. The first LE is moved forward.
3. The second LE is moved forward past the first.
4. The cycle is repeated
Partial Weight Bearing Gait Pattern (walker)
What gait is
1. The walker is picked up and moved forward about an arm’s length.
2. The involved ___limb is moved forward, and body weight is transferred partially onto this limb and partially through the UEs to the walker.
3. The uninvolved LE is moved forward past the involved limb.
4. The cycle is repeated.
Non-Weight Bearing Gait Pattern (Walker)
1. The walker is picked up and moved forward about an arm’s length.
2. Weight is then transferred through the UEs to the walker. The involved NWB limb is held anterior to the patient’s body but does not make contact with the floor.
3. The uninvolved limb is moved forward.
4. The cycle is repeated
crutches
Improve balance
Relieves weight bearing fully or partially on a LE
Increase BOS
Improve lateral stability
Allow UE to transfer body weight to the floor
AXILLARY CRUTCHES
Type of crutches thats
“Standard crutches”
Lightweight wood or aluminum
Has axillary bar, handpiece, double uprights joined distally by a single leg with rubber suction cap (1.5-3”)
Handgrip adjust 1” increments
Size: 48-60”
PLATFORM ATTACHMENTS
Type of crutches thats
“forearm rests or troughs”
Also used with walkers
Allow transfer of body weight through the forearm to the assistive device.
Used when WB is contraindicated through wrist and hand
FOREARM CRUTCHES
Type of crutches thats
“Lofstrand” or “Canadian” crutches
Lightweight wood or aluminum
Has single upright, forearm cuff and handgrip
Dual adjustment ○ Proximal: Forearm cuff ○ Distally: Height of AD
Size: 29-35
MEASUREMENT: Axillary Crutches
Measurement for this type of crutches
Standing:
Approximately 2” below the axilla (2 fingerbreaths)
Distal end of crutch should be resting 2” lateral and 6” anterior to the foot
ESTIMATE: Subtract 16” from px height
HANDPIECE: adjusted to 20-30 deg elbow flexion
MEASUREMENT: Axillary Crutches
What AT is this measurment for
Supine:
Anterior axillary fold to a surface point 6-8” from the lateral border of the heel
MEASUREMENT: Forearm Crutches
What AT is this measurement for
Standing:
Distal end of crutch should be resting 2” lateral and 6” anterior to the foot
Shoulders relaxed, elbow flexed to 20-30 deg flexion
CUFF: proximal third of the forearm, approx. 1-1.5” below the elbow
THREE-POINT GAIT PATTERN (Crutches)
What kind of gait pattern
NWB status is required on LE
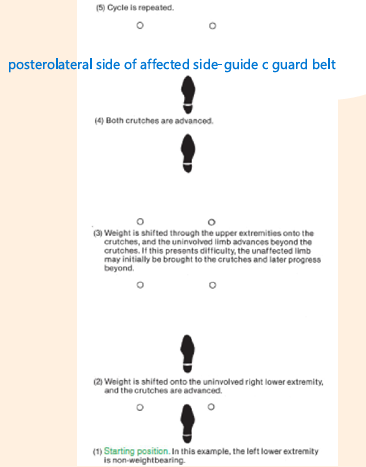
THREE-POINT GAIT PATTERN (Crutches)
What kind of gait pattern
Partial WB modification

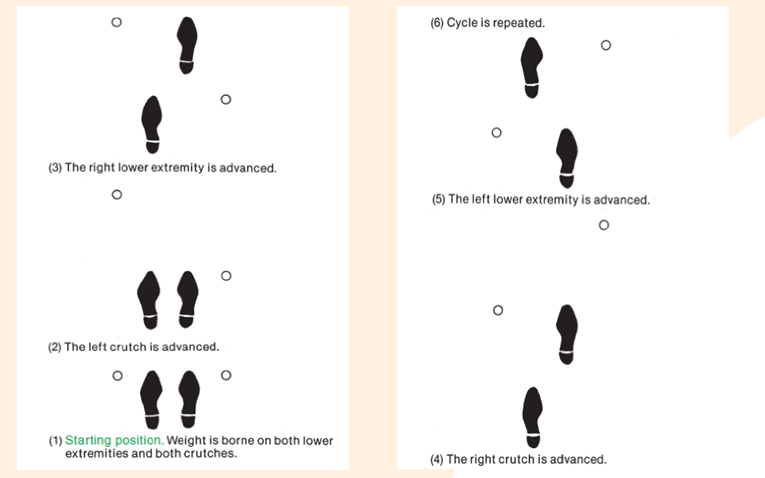
FOUR-POINT GAIT PATTERN
What kind of gait pattern
Slow, steady gait -> 3 point floor contact are maintained
Used with bilateral involvement d/t poor balance, incoordination or muscle weakness
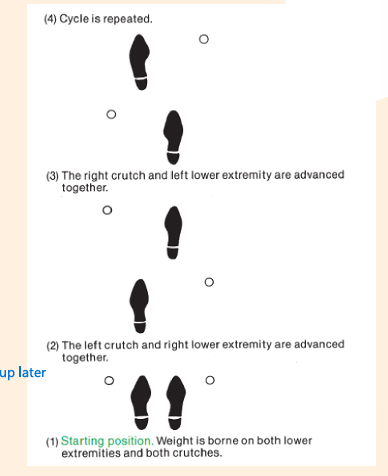
TWO-POINT GAIT PATTERN
What kind of gait pattern
Less stable -> only two points of floor contact are maintained
Requires better balance
More closely simulates normal gait
canes
Most ___used in clinical practice are lightweight and aluminum
Evidence supports the effectiveness of ___to improve balance
Reduce biomechanical load on LE joints
Not intended for use with restricted weight bearing
Typically used opposite the affected extremity
Most closely approximates the normal gait pattern
STANDARD CANE
Type of cane thats
Single-point cane / straight cane
Wood or acrylic
“crook” (half-circle) or T-shaped handle
STANDARD ADJUSTABLE ALUMINUM CANE
Type of cane thats
Aluminum, crook handle with molded plastic cover
Telescoping design with push button mechanism reinforced by thumb screw of rotation sleeve
Adjustable 27-38.5”
STANDARD ADJUSTABLE OFFSET CANE
Type of cane thats
Straight offset handle
Adjustable 27-38.5”
HEMI CANE
type of cane thats
Very broad base with 4 points of floor contact with rubber tips
Legs farther from the patient are angled to maintain floor contact and to improve stability
Fold flat
Adjustable approx. 29-37”
ROLLING CANE
Type of cane thats
Wide, wheeled base for uninterrupted forward progression •
Contoured handgrip
Adjustable 28-37”
Pressure sensitive brake
LASER CANE
Type of cane thats
Bright red laser line projected across the floor designed to overcome freezing episodes while walking
Look at laser line during freezing (shufflinh and festinating- parkinsons patients) episodes only
Regular Rubber Tip
what kind of cane tip

Tripod Tip
what kind of tip

Foldable Spiked Tip
what kind of tip

CANES MEASUREMENT
what kind of measurment is this
Place ___approx. 6’ to lateral border of toes •
Two methods
Top of ___at the level of the greater trochanter ○
Elbow should be flexed between 20-30 degrees**
Allows the arm to lengthen and shorten during different phases of gait
Shock absorption mechanism
** more impt indicator of correct cane height
CANES GAIT PATTERN
what kind of gait pattern is this
Placing the ___too far forward or to the side will cause forward or lateral bending -> decreasing dynamic stability
Bilateral involvement? •
Which side is cane more comfy?
Which side would make balance more stable/improve ambulatory endurance?
Is one side more able to correct gait deviation
More safer
Grip strength
Two canes? -> two or four point gait pattern
Bed rails
Enables the patient to perform bed mobility and transfers and avoid soft-tissue pressure and dev’t of contractures as a result of prolonged immobilization
Protects the patient from rolling off the bed
Overhead trapeze
AT for moving a supine patient to a sitting position
Call light
When turned activated, a light/buzz over the patient’s doorway interpreting that the patient requires assistance
Sliding board
-It can help ease the transfer by bridging the gap between a surface to another surface (i.e., bed to wheelchair)
Pivot disk
Used to facilitate the pivoting process for patients during pivot transfers
More commonly used for moderate and maximum-assist manual transfers
Marisa lift/sit-to-stand lift
Designed to lift a dependent patient for the purpose of transfer
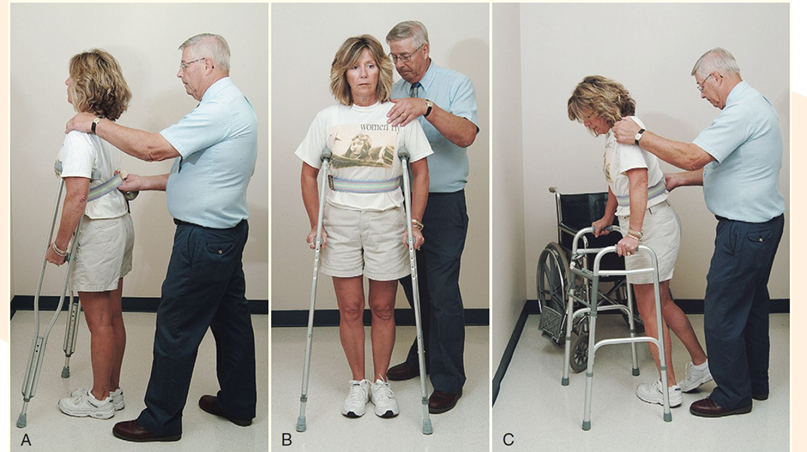
Guarding techniques during ambulatory exercis
1. The therapist stands posterior and lateral to the patient’s weaker side.
2. A wide BOS should be maintained with the therapist’s leading LE following the assistive device. The therapist’s opposite LE should be externally rotated and follow the patient’s weaker LE.
3. One of the therapist’s hands is placed posteriorly on the guarding belt and the other anterior to, but not touching, the patient’s shoulder on the weaker side.
Stair climbing
If railing is available, it should always be used, even if it requires placing the assistive device in the hand in which it is not normally used
GOOD LEG GOES TO HEAVEN, BAD LEG GOES TO HELL
Guarding techniques on stair climbing: ASCENDING STAIRS
1. The therapist is positioned posterior and lateral on the affected side behind the patient.
2. A wide BOS should be maintained with each foot on a different stair.
3. A step should be taken only when the patient is not moving.
4. One hand is placed posteriorly on the guarding belt and one is anterior to, but not touching, the shoulder on the weaker side.
Guarding techniques on stair climbing: DESCENDING STAIRS
1. The therapist is positioned anterior and lateral on the affected side in front of the patient.
2. A wide BOS should be maintained with each foot on a different stair.
3. A step should be taken only when the patient is not moving.
4. One hand is placed anteriorly on the guarding belt and one is anterior to, but not touching, the shoulder on the weaker side.
Guarding techniques on stair climbing:CANE- Ascending
1. The unaffected lower extremity leads up.
2. The cane and affected lower extremity follow
Guarding techniques on stair climbing:CANE- Descending
1. The affected lower extremity and cane lead down.
2. The unaffected lower extremity follows.