H&H exam 2- Sex development and Males
1/60
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
61 Terms
3 types of sex + brief descriptions
chromosomal sex (established at fertilization), gonodal sex (embryonic gonads develop into either testis or an ovary), phenotypical sex (external and internal genitalia and secondary sex characteristics)
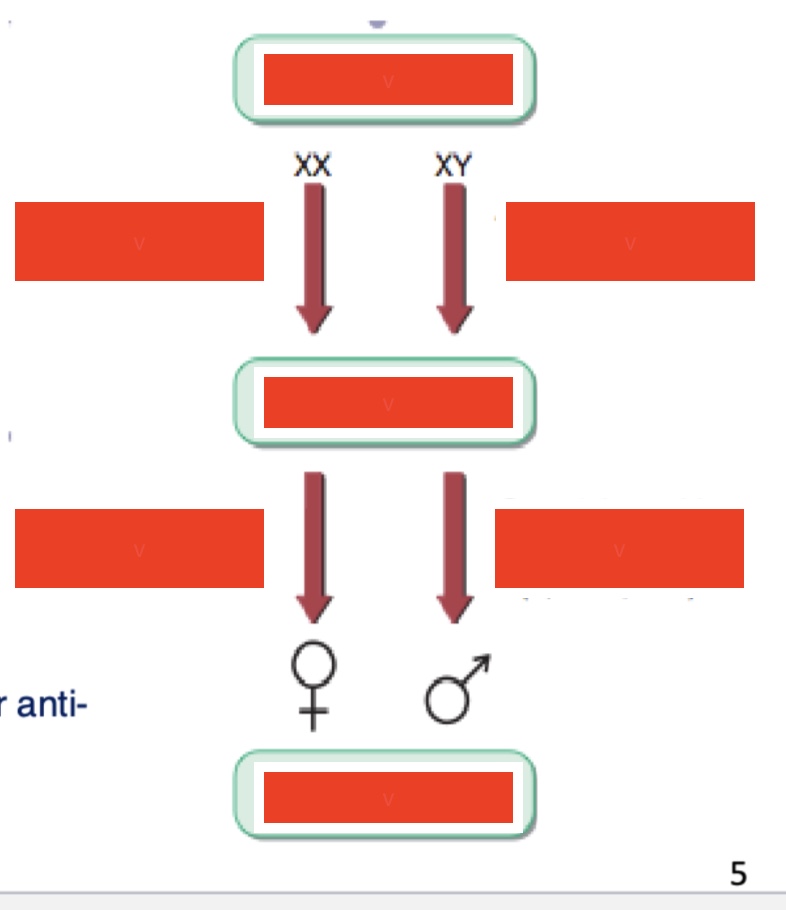
normal sex development label
green boxes: chromosomal sex, gonadal sex, phenotypic sex
left column: ovary-determining genes, gonadal steroids (E2)
right column: testis-determining genes, gonadal steroids and peptides
karyotype for chromosomal sex for males and females
male: 46 XY
female: 46 XX
DHT long
Dihydrogentestosterone
MIS or AMH long
Mullerian inhibiting substance, Anti-Mullerian Hormone
E2 long, what is it (simple)
gonadal steroid, 17β-estradiol
SRY- long, function, what are the implications
Sex-Related gene on the Y chromosome, in the presence of it- testis (activates testis promoting genes), in the absence of it- ovaries, testis-determining factor (TDF), default are ovaries (but not entirely)
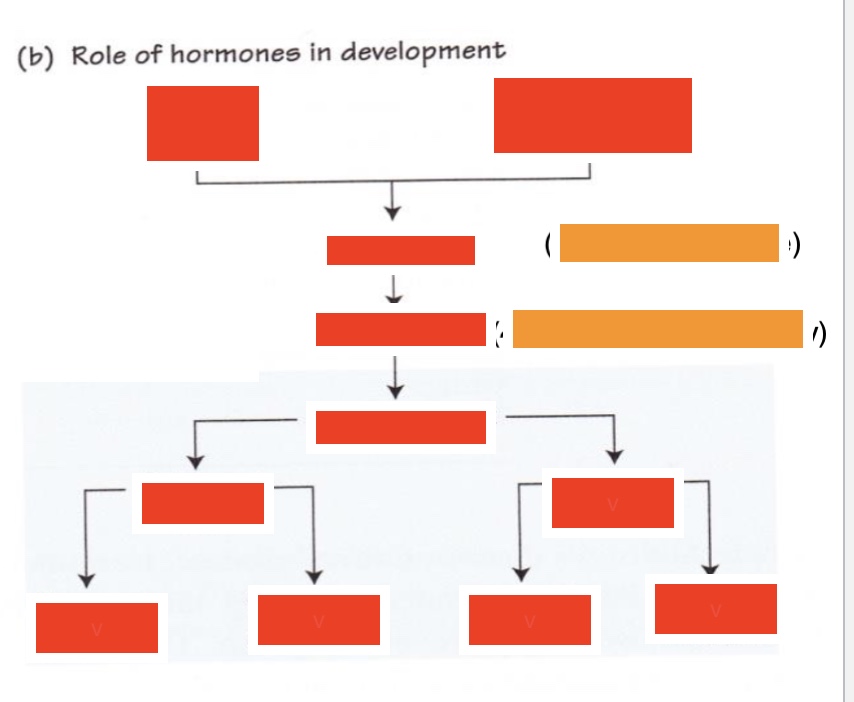
top 3 lines label (both red & orange) (left to right, by line)
ovum, spermatozoon
genetic sex (XX or XY genotype)
gonadal sex (~4 weeks, ovary or testis)
label bottom 3 rows (left to right, by line)
phenotypic sex
peripheral sex, brain sex
external genitalia, secondary sex organs, sexual behaviour, pituitary function
sexual differentiation: at 4 weeks
gonads still indifferent, can develop into testis or ovary
How does sexual differentiation happen in males (basic ish) (3 main points)
under the control of SRY gene, genes activated for testoicular development, Sertolli cells produce Mullerian inhibiting hormone (MIH), causing atrophy of the mullerian duct, Leydig cells secrete testosterone (which after conversion to dihydrogentestosterone supports development of the Wolfian duct)
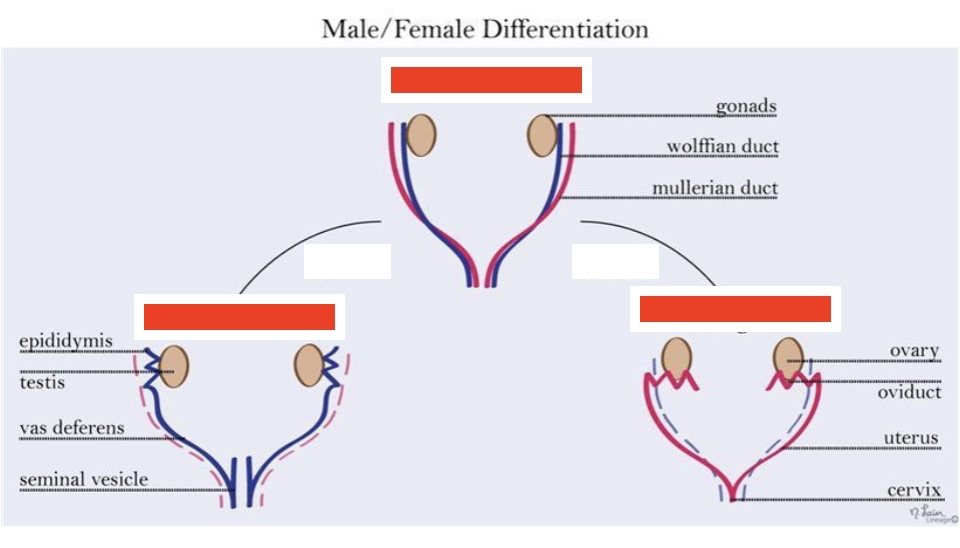
label left to right
male gonad, bipotential gonad, female gonad
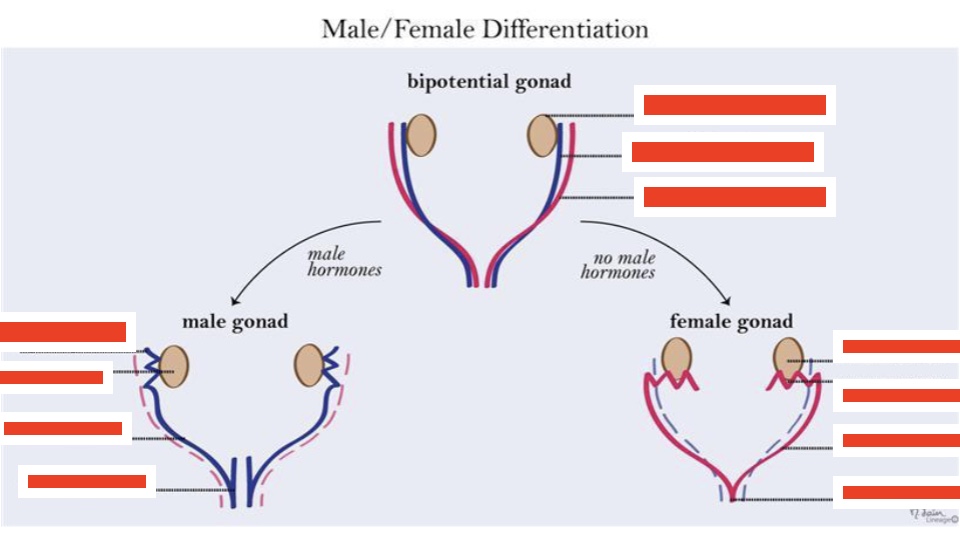
label the bipotential gonad (top to bottom)
gonads, wolffian duct, mullerian duct
label the male gonad (top to bottom)
epididymis, testis, vas deferens, seminal vesicle
label the female gonad (top to bottom)
ovary, oviduct, uterus, cervix
How does the expression of SRY induce testis development?
SRY→SOXY9→FGF9→Serolli cells
what happens when there is a mutation of SRY in 46 XY males (eg a deletion)
no testes development
what happens when there is a translocation of SRY into 46 XX females? What is it called?
Induces testis development and a male phenotype, ovo-testicular disorder of sexual development
Difference in sex development: Ovo-testicular disorder of sexual development description, percentages of how it works
formerly called true hermaphroditism, both an ovary and a testis in one individual or an ovotestis, 60% 46XX, 15%XY, 25% mosaicism
ovotestis description
ovarian and testicular tissue combines in the same gonad
Androgen Insensitivity Syndrome (AIS) description, prevalence
mutation in androgen receptor (X linked), 1 in 100,000 chromosomal males (46XY), testosterone levels (usually) normal for males
Complete AIS 5 features
female phenotype, normal breast development, scanty pubic and axillary hair, short vagina (but no uterus), female psychosexual orientation
Partial AIS 3 features
perineoscrotal hypospadias (dislocated urethra), small undescended testes, gynecomastia (increase in male breast tissue during puberty)
Klienefelter syndrome: description, prevalence, percentages when it happens
47XXY, 1 in 1000 men (75% not diagnosed), meiotic non-disjunction of sex hormones during gametogenesis (40% during spermatogenesis, 60% during oogenesis)
Other variants of Klinefelter syndrome description
mosaicism, 48XXYY, 48XXXY- rare and result from chromosomal mitotic non-disjunction within the zygote
clinical features of Klinefelter Syndrome (7)
low T (50-75%↓), High FSH and LH (85%↑), increase of estradiol (conversion of testosterone), infertility, “eunuchoid” proportions, incomplete development of male physical characteristics, gynecomastia
What is incomplete development of male physical characteristics also called
under-virilisation
What happens between 6 and 8 years of age in terms of puberty (2)
adrenal glands produce more androgens (DHEA), reactivation of the H-P-Axis and production of GnRH
GnRh throughout development
active in fetal life and early infancy, quiescent until early puberty when it it is reactivated
Why do obese children enter puberty earlier?
involvement of leptin (from adipose tissues) to enter puberty
tanner scale description
scale of physical development in children, adolescents and adults, based on external primary and secondary sex characteristics
Puberty events in males order
testiscular volume rises earlier than genitalia or pubic hair
What happens in early puberty- males (9)
nocturnal surges of LH and FSH, increase in testicular volume, ↑T levels, deepening of the voice, prostate growth, facial hair growth, initiation of recession of temporal hairline, GH increases IGF-1 and linear bone growth, prolongued pubertal exposure to gonadal steroids causes epiphyseal closure
Causes of precocious puberty description, 2
age <9, premature sexual development, gonadotropin-dependant (central precoucious puberty), gonadotropin independent (androgens from the testes or adrenals)
delay puberty when, causes (5)
not started by 14, constitututional delay of growth and puberty, systemic disorders (malnutrition, anorexia- bc leptin is very low), CNS tumors, H-P causes (low gonadotropin- can be congenital or aquired), androgen insensitivity
Male hormones: acronyms & long (5+1)
GnRH- Gonadotropin releasing hormone
LH- Luteinizing Hormone
FSH- Follicle Stimulating Hormone
DHEA: Dehydro-epiandrosteron
DHT: Dihydrotestosterone
and estrogens
Leydig cells description
stimulate testosterone synthesis, regulatory control of androgen synthesis is mediated by testosterone feedback on both hypothalamus and the pituitary gland
Sertolli cells description
nurture germ cells to divide, differentiate and mature into sperm (spermatogenesis), secrete inhibin B which suppresses pituitary FSH
How is GnRH released?
in distinct pulses every 2 hrs, resulting in discrete pulses of LH and FSH
ABP long
androgen binding protein
How do Leydig cells work?
activated by LH (binds to membrane receptor), cAMP and PKA - leads to new protein synthesis, creates enzymes that convert cholesterol into testosterone
What is the result of Leydig cells function
local T concentration is very high around them, (in circulation is a lot more diluted), has a paracrine effect on Sertolli cells
How do Sertolli cells work? (from diagram) (4 ish steps)
activated by FSH - cAMP and PKA - new protein synthesis which creates: inhibins, aromatase (which converts T to estradiol), ABP, then high ABP and T [] induces production of sperm cells
Maturation of the sperm cells (3 points)
occurs gradually from the basal lamina to the lumen of the tubule, complete maturation requires 74 days, spermatozoa spend 21 days in the epididymis for further maturation
how many sperm cells does an adult testes produce in a day? Why is this relevant?
100 million, makes it a lot more difficult to make a male reproductive pill
Percentages of T binding
0.5-3% - unbound
50-70% - albumin
30-45% - SHBG (Sex hormone binding globulin)
circulating testosterone, where is how big percentage derived from?
95% of circulating T is derived from the testis
DHT vs testosterone
DHT is more powerful than Testosterone
Where is T mainly metabolized and excreted?
mainly metabolized in the liver and excreted in the kidneys
Influence of T on: skin (2), male sex organs (3), muscle (1)
skin: growth of facial and body hair, supports collagen
male sex organs: sperm production, prostate growth, erectile function
muscle: increased muscle mass and strength
Influence of T on: brain (3), bone marrow (1), bone (1)
brain: sex drive, positive feelings, aids cognition and memory
bone marrow: red blood cell production
bone: bone density and maintenance
DHT & hair
causes hair loss- decreases blood flow to hair follicle and decreases keratin production, finasteride can block conversion of T to DHT
disorders of the male reproductive axis during adulthood (3 + sub points)
Hypogonadism- primary testicular cause of hypogonadism, androgen insensitivity syndrome, hypogonadotropic hypogonadism (secondary)
gynecomastia, aging-related changes in male reproductive function
T levels and aging
they decrease natural over time as you age, can be beneficial to boost it later on with T treatments
total testosterone levels testing results
<200ng/dl - T deficiency
200-350ng/dl - repeat testing
>350ng/dl - androgen deficiency unlikely
What to do if testosterone deficiency found (how to determine if primary or secondary hypogonadism)
test the LH level- high level LH→ primary hypogonadism, low/inappropriately normal level of LH→secondary hypogonadism
signs of hypogonadosim both severe and partial
severe: absence puberty, sexual infantilism (hypospadias, undescended testes)
partial: delayed/arrested sex development, abnormalities in LH pulse frequency/amplitude
aquired hypogonadotropic disorders: reversible (6ish)
stress, severe illness (HIV, COPD, etc.), malnutrition, opioids & marijuana, exercise-induced (only women)
Obesity associated secondary hypogonadism
1- leptin increases→ SHBG decreases→testosterone long =, later decrease
2- testosterone → aromatization in adipose tissue → increase in estradiol
Adverse effects of (ab)use of anabolic steroids
suppression of LH and FSH,
Testing for abuse of steroids
high ration of T to epitestosterone, (normal ratio is 1:1, anything higher than 4:1 indicates doping use)