Construction of the Body/ Scientific Medicine
1/73
Earn XP
Description and Tags
(Stephen Mawdsley) How have ideas of the body and health changed with the emergence of scientific medicine?
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
74 Terms
Scientific Medicine
How was western medicine practiced before the discovery of scientific medicine?
Public health & disease prevention based on… miasmatic theory
Rooted in Hippocratic trad.
Belief some diseases/ ‘distempers’ were caused by foul air smells & decomposing matter
Infections
spread by individualsbut by contaminated vapoursSolution: clean up waste & reduce fetid odours (body needs clean air to thrive)
Scientific Medicine
How was western medicine practiced before the discovery of scientific medicine?
Public health & disease prevention based on… humoral theory
What defined a ‘healthy’ body in EM thought?
(EM Europe) Most dominant & prevalent model for understanding body
Rooted in Hippocratic trad.
Healthy body defined through balance humors & proper bodily flow (body as site pot. imbalance, sickn. caused by imbalance)
Approach based on observation (i.e. if intervention did something, then sure to restore balance)
Seeking noticeable physiological reaction
Used…
Toxic substances (arsenic power)
Addictive substances (alcohol, opium-derivatives, cocaine…)
Flexible & comprehensive
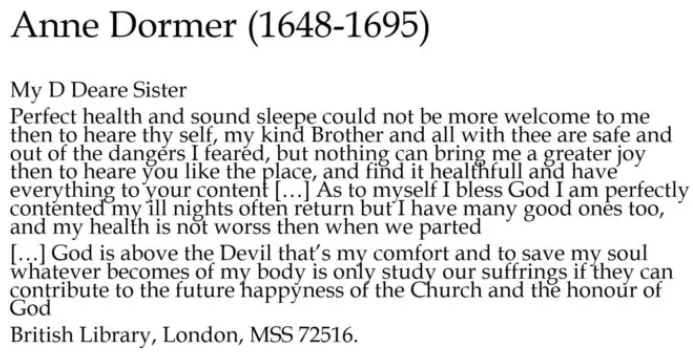
Understood by physicians & by laypeople (letter say. her own health entirely constituted by whether or not she gets good news ← her sister ab. their safety)
shows us how people understand sick/ healthy bodies & how they control narratives around them
appealing to sister for sympathy & connection + act writing & rec. letters is medical act
Interwoven w/other systems like astrology, occult & religion (Notion)
Emotions key way in which people moderate their health: have physical impact on body (grief → blood rushes to heart; dies of broken heart)
(1650s-) Chall. by iatrochemical models for body & disease
(C18) Chall. by nerves (Notion)
Growth interest in statistics & beginnings public health
How was maternal health assessed after CB?
Q: How was maternal health assessed after childbirth?
A: Through a process of purging, particularly the expulsion of lochial blood. A mother was considered 'well' once bleeding ceased, symbolizing the removal of pregnancy remnants.
Q: What was 'lying-in' and how did it function?
A: A month-long postpartum rest period where women were confined to bed. Both religious and medical texts promoted this, marking it as crucial for recovery, symbolized by three stages: bleeding, churching, and return to health.
democratic medicine: exper. sickn. & ability
bedside → lab medicine
define both
when does this shift happen
How does this impact where patient sits in medical encounter?
How was this due to more democratic medicine?
(Nicholas Jewso'n’s article 1976 The Disappearance of the Sick Man ← Medical Cosmology)
Sick indiv. as central story-teller
Physicians could go off patient narrative,
tests→ good doctor had good bedside manner & could induce good/ informative patient narrativeDomestic space
(Roy Porter, 1985) Patient & practicioners co-contstruct narratives of body w/host social & community influences around patient
letter next: appealing to sister for sympathy & connection + act writing & rec. letters = medical act (letter recappting to sister what’s going on w/body & health)
Both patient & practicioners had shared system for understanding body… working off same hymn sheet, even if informed by diff. social & cultural priorities.
C18-19 →
Subject to be classified through observation
Increas. lack interest in patience → importance practitioner’s narrative, informed by shift <_ domestic space medicine, growth hospital & lab test. (test patient narratives w/objective facts)

democratic medicine: exper. sickn. & ability
historiography shift to focusing on patient narrative
larger methodological question we need to grapple with…
is narrative shaped by subjective experience OR by historical & cultural forces
when person descr. what’s wrong w/them, are they doing this ← their subjective somatic exper. OR ← place cultural & social imposition?
How much do those social, cutlural & historical things influence actual exper. body?
Historians increasingly sceptical ab. this shift to focusing on patient narrative
Doesn’t do en. to uncover material & somatic exper. being unwell, healthy & hav. encounter w/practicioner.
But it’s all we’ve got to work w/…
Both patient & practicioners had shared system for understanding body… working off same hymn sheet, even if informed by diff. social & cultural priorities.
In this sense, model body both draw. on.
accepted/ bad ways feeling ill & behaving…
Both patient & practicioners had shared system for understanding body… working off same hymn sheet, even if informed by diff. social & cultural priorities.
democratic medicine: exper. sickn. & ability
(EM) define ‘medical encounter’
Just ‘clinical encounter’ - m/what we consider ‘medicine’ takes place in other spaces
→ medical encounter = moment/ series overlapping moments in which 2 individuals meet for health-related reason
Medicine takes place in lots locations & overlaps w/other kinds history
Broader social spaces: households, courts, communities
Tak. place in objective context/ where healing main objectivemedical court inspection
when women claim pregnant → can’t be executed (plead the belly); midwives brought in to assess pregnancy
injury work/ assault - medical experts inspect body to determine cause/ progress illness → compensation, not illness)
transatlantic slaves inspected & their suitability for slaves eval.
certain narratives being told, shared model body as practicioners… yet doesn’t have healing at heart nor take place in clinical setting
doctors prov. expertise, not treatm.
democratic medicine: exper. sickn. & ability
PS public nature EM medicine
engraving ← C18 medical text
sold anti-STI spec. pill
this was done by moralistic artists
real moralistic judgement that his clients are wealthy middling sort (excess feasting in middle + ornate clohtes)
criticism & moral judgem. how middling sort get ill & behave when ill (illn. comes ← excess enjoyable things) & dodgy doctors allow. them to behave in this way
mediicne happening in public way… kind disease you suffer ← says someth. ab. who you are & you behaviour
Mid C18 engraving mountebank (EM word for quack doctors)
conflation bet. disabilities, appearance & offering irresponsible/ incorrect medical care
(EM context) medicine not alw. in clinical but also households, courts & communities
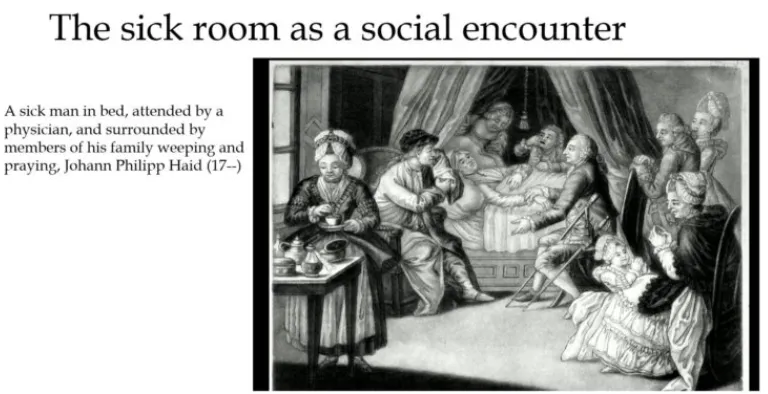
sick room as social encounter (other side)
Being sick v/public/ social… visitation important part EM social norms of going & visiting ill individuals within your community
sufferer sitting amongst host individuals
they’ve set up stations within sick rooms with snacks, entertainm… contrast to how we now perceive illn. as priv. exper.

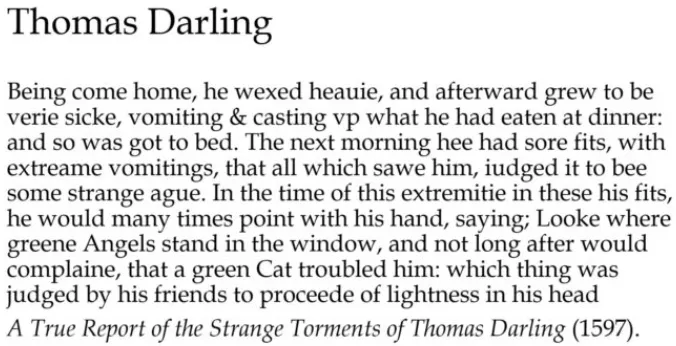
cultural scripts & illn. behaviour
What are ‘cultural scripts’ and how did they shape illness?
A: Shared cultural ideas (about witches, divine punishment, maternal sin) shaped how people interpreted and responded to illness—beyond just medical models.
cultural scripts & illn. behaviour
role religion EM medicine
Humoral & relig. emphasis on moderation & understand. bodily conduct impacts on soul
RC confession
Prot. emphasis on self-exam. (partic. Puritans)
encouraged to use diaries, letters & other written forms ab. their bodies to confess sins & poor conduct
Providence as central framework for mak. sense illn. & environment
Anxiety/ tension ab. salvation
illness as divine test/ retribution… struggling through them → closer to God → salvation OR punishm OR demonic possession… unsure
Importance suffering well & dying well → conduct manuals
earlier letters mentions devil - related to sin & test
being spiritual model for others when ill - their expert. written into guides to show other people ideal conduct due. illn.
cultural scripts & illn. behaviour
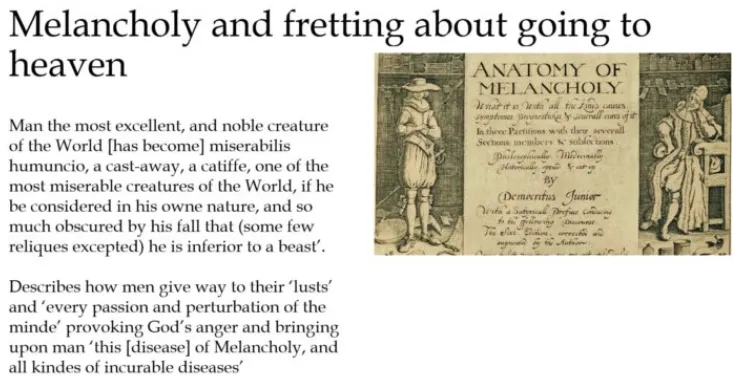
religion x changing ideas melancholy
nowadays akin to depression but then interestesting transform…
(Renaissance) excess melahcolonic humor/ black bile → sleeplessn., poor appetite, irritability, agitation
(end/ mid C17) maybe sign of genius?
most good writers & thinkers been of melancholic dispotion
possibility melancholy punishm. for sin everyone, not spec. sin everyone but reflection world’s moral degradation
Robert Burton’s text Anatomy of Melancholy talks ab. miseries world & their relation to man’s lack morals
men give way to their lusts & every passion & perturbation mind, provoking God’s anger & bringing upon man this disease of melancholy & all kind incurable diseases
religion could offer succour
when people come down w/melahcoly, fret they’re not elect & damned - terrified this is sign not going to haven; they have these symptoms
cultural scripts & illn. behaviour
What is the trad. of a ‘good death’?
Draws on older MA 7 & classical trad. ars moriendi (ways your death ought to have moral message for others)
Defin. death in positive terms & acceptive/ welcoming its inevitability.
Positive; end suffering, beginning someth. bettr - must accept it as divine will
For prepared, examined Christian, to be feared/ resisted.
Troubling/
accepting divine willto fight death & scream on deathbed
Affirm w/good conscience their devotion to God.
On deathbed, should reaffirm commitm. to God as way being spiritual model to others.
Scientific Medicine
How was western medicine practiced before the discovery of scientific medicine?
→ bloodletting (phlebotomy)
Ab. inspiring physical change in the body
Release of blood believed to allow humors to rebalance
Open a vein; ½ - 3L drained
Came w/risks death, fatigue & infection
It ‘worked’ within prevailing conceptions body/ illn.
(EM) How do we know ab. medical experiences for those who engage w/practicioners?
Writing practices
Relig. emphasis on self-exam. & new trends in book-keeping & autobiographical writing filters down to all levels soc…
Encouraged literate individuals to keep paperwork often on behalf of other fam. members
Episodes illn. seen as important to narrativise within fam. history… so many ← literate EM families talk. ab. illn. & health because narrativising body key route to embodied devotion & going to heaven
Account books, recipe books, commonplace books, diaries, journals, letters, letter books…
These texts priv. but public & used as spiritual model - written self-consciousnly
consciously replicating cultural scripts & idealised patterns behaviour & being
→ self & others constructed in relation to these norms
public diaries: Alice Thornton vs Samuel Jeakes & Samuel Pepys
writes 4 volumes autobiography later in life, all ab. episodes sickn. & trials in her life
writes this explicitily trial happen. to her (accused trying to remarry too quickly + to man betrothed to her daughter) caused her illn.
circulates these within her community to actively rescue her rep.
episodes illn. & how you deal w/them
evid. people use to construct their reputations within communities
sugg. social trials (slanders) could have physical impact, even caus. death
To defend her reputation against slander (accused of remarrying too soon to her daughter’s betrothed), linking social trials to illness, and circulating it locally to recover her standing.
rather than citing social & emotional things as caus. his illn. & context around it, emphas. precision, time places, no. fits
us. his personal exper. hav. fits prev. to assess progress his symptoms
gendered narratives illn. & recovery
What can the difference bet. Alice Thornton & Samuel Jeakes/ Samuel Pepys tell us ab. how men & women differed in writing ab. illness?
(Olivia Weiser) Men & women wrote ab. health & illn. in diff. ways:
Men privileged their own bodily experiences over words & opinions of others - emphas. empirical observation (dates, fits, bodily data) & avoid. social/ emotional context.
Jeakes us. his personal exper. hav. fits prev. to assess progress his symptoms, not prov. social/ emotional context around it - v/spec. assessments their health
Women looked to others as models suffering & attributed their own illn. & recovery to negative/ positive affective relations - linked illnesses to emotional/ social trials (e.g. slander), often ref. others’ suffer. & us. affective lang.
Owing to cultural scripts & expectations + ideas ab. women’s physiology
umoral model & that women are colder & wetter than men: women’s bodies take impression social, practical things because like wax → impressionable
See this throughout women’s letters: desc. feeling symptoms of others (way offer. sympathy + pot. description their own somatic exper.)
Men tend to attribute bodily periods illn. to financial & econ. problems in way suggests still affected by emotions but diff. to women
exper. illn. & ability
EM expectations recovery x historiography
(old historiography) Everybody died → expectation recovery
(new) People expected to recover
Humoral system v/optimistic - health tied to removal bad humors
Frustration & difficulties when experiences
map onto expectations.
gendered narratives illn. & recovery
How did maternal illn. chall. medical prescriptions?
Despite prescriptive models tying recovery to bleeding and churching, many women felt unwell long after. Recovery was not fixed but based on personal perception of restored bodily order.
gendered narratives illn. & recovery
What was the cultural contradiction in postpartum health models?
The idealized one-month recovery did not reflect women’s actual experiences, which often involved prolonged weakness, grief, or complications like breast inflammation and tearing.
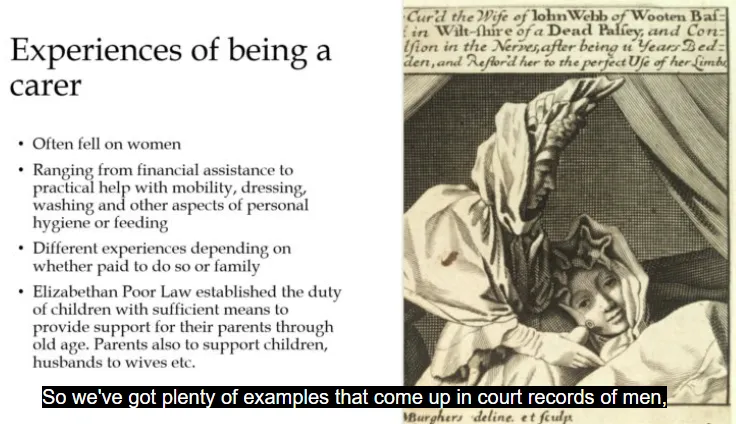
exper. illn. & ability
How did EM people exper. sickn. & recovery?
Illness could cause prolonged disruptions to family life, with both women and men (fathers, husbands) involved in caregiving. Letters and diaries reflect these personal, social, and economic impacts.
exper. illn. & ability
How was disability understood?
Through moral & relig. len
Personal/ parental sin
Suffering (through
ability) could be perceived as test faith
Practical needs - e.g. inability to work
impotent poor supp. by parish & fam.
Charity as important part worship & relig. life (declines after ER) but conditions ways people feel import. to supp. those who can’t work
for people unable to work then owing to physical & mental factors, somebody might be paid to take care of them
Clear identity being ‘disabled’/ ‘able-bodied’ until…
exper. illn. & ability
When did disability become a conceptual identity?
1st time ability conceptualised as ‘identity’ = William Hay, Deformity: An Essay (1754)… shift situational → identity-based thinking
kind work disabled people might do determined by where they lived/ econ. context affected disabled people’s work
David Turner’s book on disability C18 showed how people had an understanding chronic conditions that might continually impact their ability to carry out business… he notes capacity to work was determined not just by nature person’s impairments but also by structure & diversity local econ.
(rural places) active lab. needed → more likely for disabled people to be supp. by parish
(urban centres like London) lots casual employment → more likely to find people w/disabilities working
Rural areas: Disabled people more likely to be supported by the parish.
Urban centers: Availability of casual labor allowed more participation despite disability.
gendered narratives
EM maternal imag.
→ birth marks (crav. strawberries → red marks)
disability like dwarfism recogn. - could ← maternal conduct dur. pregn.
not eating right things
poss. ‘monstrous births’
maternal imagination - pregn. women’s thoughts have dir. impact on shape body child
Agnes Bout’s cat - 16002 story women gave birth to cat; had looked at cat too long whilst pregnant
racial diff.
Aristotle’s mastrpiece (early sex guide): woman mediated too long on rabbits had baby born w/hair all over body
explained racial difference - discusses possibility baby being born black; mother looking at image black man when conception happen. & when pregn.
Q: What was the theory of maternal imagination?
A: Belief that a pregnant woman's thoughts or fixations could imprint on the fetus (e.g., birthmarks, deformities, even racial difference). Seen in stories like women birthing animals or babies with unusual features.
Q: How did these ideas reflect humoral theory?
A: Women were considered "cold and wet," thus more impressionable—like wax. This justified why women’s bodies were thought to respond to emotional, spiritual, or sensory impressions.
Q: What was churching and how was it perceived?
A: A religious ritual marking purification after childbirth. Some women appreciated the attention, others experienced it as disconnected from their true recovery. Social status and obligations also affected whether full “lying-in” was possible.
EM experiences being carer
cultural scripts & illn. behaviour
How did cultural scripts clash with medical prescriptions?
Leah Astbury, ‘Being Well, Looking Ill: Childbirth and the Return to Health in Early Modern England’, Social History of Medicine 30/3 (2017), 500-519.
Medicine claimed to be personalised (based on humoral balance), yet enforced standard recovery timelines (e.g., one month postpartum), creating tension bet. indiv. exper. & normative ideals.
Gap bet. prescription by medical authors & relig. authorities and the experiences of patients.
Being technically healthy vs feel. healthy
Whilst returning to internal estim. former self =
equivocalaim after birth care regimes, feel. healthyalw. correspond to prescriptive timetables.Recovery measured by when woman felt she’d returned to normal functioning
childbirth
medicine as more personal, indiv.
(medical texts) Contradicting stipulations ideal bleed. period → room to manoeuvre; for recovery fast/ sluggish to be perceived as alarming, & for women to read their own bodies & assess whether they’d truly returned to health. Nat. variation rates recovery. Understood variability in speed recuperation indicated in medical lit. & embedded in childbear. narratives families constructed in life-writ. sources BUT need to bleed seen as essential to surviv. childbirth.

cultural script of EM CB
Codified practice/ knowl. conceived women as being cured after month-long ‘lying in’ despite personal/ indiv. nature humoral constitution (medicine had to be personalised to balance humnoral constitution to what people had been born w/) - contradiction
(p.8-10) Rate recovery newly delivered woman & speed @ which she might conceive again reflected maternal & paternal good health & freq. & pleasure their sex + had broader implications for rep. family as a whole.
p.9) unobstructed birth and quick recovery demanded a womb that was yielding-it expelled a baby, the placenta and lochial blood steadily and without retention. A birth that was too swift and painless could, however, be shameful. Laura Gowing in her work on the cultural recognition of pregnancy has suggested that unmarried women accused of infanticide claimed to have had 'short, painless or unexpected labour' both to explain why they had not called for assistance, but also to support the argument the child had been born dead.51
painful birth meant to help you emathise w/JC’s suffering on cross… developm. spirituality
cultural scripts & illn. behaviour
How did cultural scripts clash with medical prescriptions → CB example
Focus on humoral recuperation: compl. excretion corrupting matter → expected to return to former self within month birth
(prescriptively - medical & relig. models childbirth) Bleeding commensurate w/recovery
Mother ‘well’ when she’d been delivered child & placenta + bled aw. lochia. Meant to occur in month after delivery.
BUT bodily effects childbear. contin. to impede ability to return to normal household tasks & behaviours long after
Narratives women’s ‘childing’/ ‘childebed’ narratives contin. after they perceiv. their bodies
affectedby pregn. &lab.Recovery ← childbirth
clear, formulaic proc.as medical lit. implies.
Churching supposedly marked moment when mother returned to her normal household activities
Few financial constraints on aristocratic women BUT (Laura Gowing) ‘lying-in for a month was prob. impracticable’ (R3); work/ other obligations curtailed period recuperation + necessitated quieter & less extravag. celebrations
→ For women in
financially & socially privileged en. pos. to enjoy month lying-in, rituals church. & leav. house bore even less rel. to whether they felt well.find PS from Notion
Despite dominance prescriptive framework month to recover, for many women cessation postpartum bleed. & churching
correspondw/when looked/ felt well. (against historiography)Childbearing = fluid, ongoing proc. Women’s bodies could contin. to be effected by birth. long after their formal confinem. up.
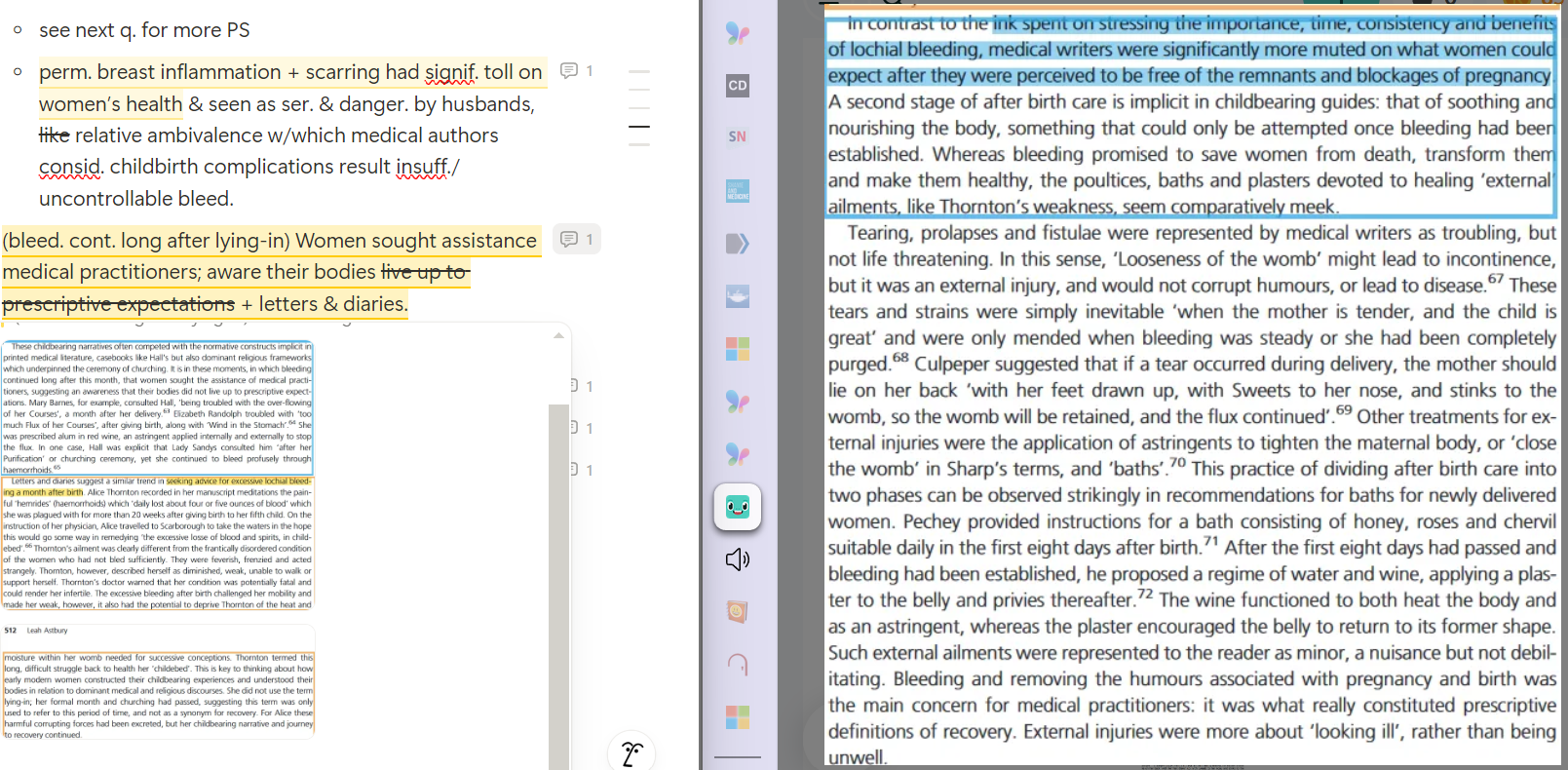
Take into account other childbirth ills (weakn., limping, breast ailments, tearing).
(medically prescriptive material) Consid. life-threatening but contin. to curtail return to former self.
(bleed. cont. long after lying-in) Women sought assistance medical practitioners; aware their bodies live up to prescriptive expectations + letters & diaries.
life-writing, health & family
What role did life-writing play in understanding health?
Were men involved in maternal health narratives?
How did family and health intersect in the early modern period?
correspondence, journals & spiritual meditation of women & their families
Letters & diaries allowed both men and women to record, share, & assess their own or others’ health. Recover often defined in terms of how one felt,
merely medical criteria.Yes. Men wrote ab. CB, symptoms, and bleeding-in letters.
(Magdalena S. Sanchez) CB
nec. seen as‘strictly feminine event’+ domestic medicinejustfemale domain(Sarah Reed & Jennifer Evans) Acted as informers, commentators, seekers of care & repositories of knowledge.
Historiographic: shows fam. more import. context for birthing than female communities dom. prev. histories birthing.
Rate of recovery and return to sexual activity affected not just maternal but paternal health and family reputation. Illness had implications for family honour and social standing.
Prolonged recovery (brought on by insuffic. purging/ lasting weaknesses & ailments) signif. disrupted fam. life
Disruption to normal & expected routine mirrored & reflected internal bodily disorder mother & child.
Fathers; daily duties & activities curtailed by diffic. & arduous recoveries.
Female correspondence also records disruption to social arrangements - immobility could prevent women ←fulfilling normal household duties.
Scientific Medicine
How was western medicine practiced before the discovery of scientific medicine?
→ purgatives/ emetics
Ab. inspir. a physical change in body
Purgatives/ emetics intended to cause body to expel contents stomach/ bowel
Noticeable change
Health risks: dehydration, electrolyte imbalance/ death
Scientific Medicine
How was western medicine practiced before the discovery of scientific medicine?
→ poisons to treat diseases
historic medicinal uses/ treatments/ cures for
arsenic
syphilis
some cancers
skin conditions
mercury
diuretic
laxative
syphilis
dewormer
Scientific Medicine
How was western medicine practiced before the discovery of scientific medicine?
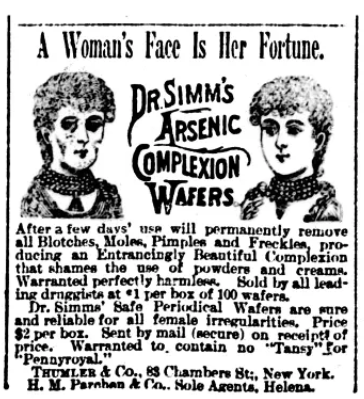
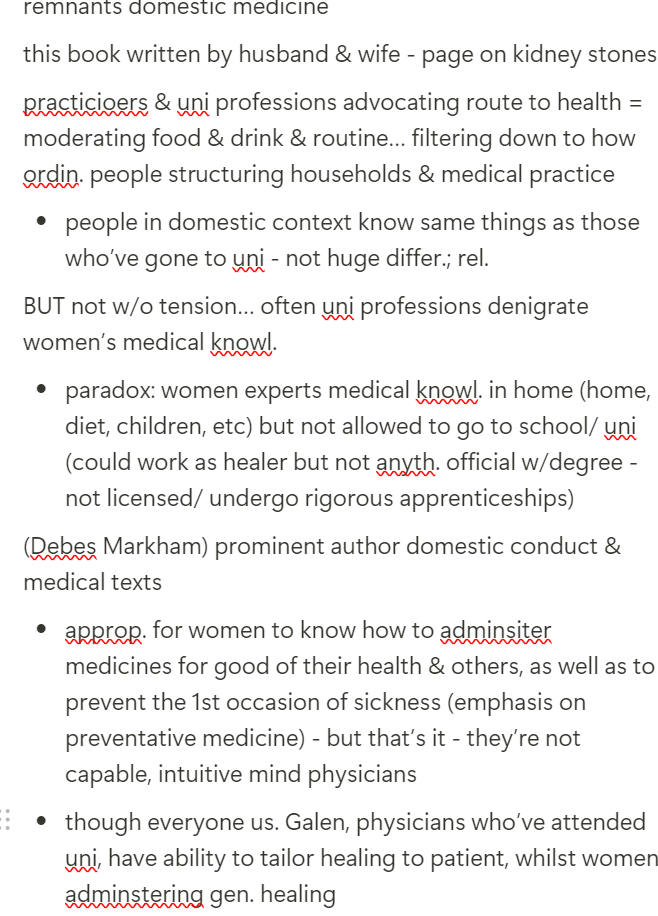
→ recipe books & domestic medicine
What practitioners & uni professors advocate filters down to how ordin. people structure households & medical practice…
ideology borrowed ← W medicine
based on premise you & your fam. know your body best
power/empowering
privacy
offered guidance in prep. & administ. homemade preparations
domestic & fam. medicne books v/pop. (early 1800s-early 1900s)
affordable (altern. to expense consulting physician)
autonomy (could grow some ingredients in own garden)
tensions for women… (picture)
Scientific Medicine
How was western medicine practiced before the discovery of scientific medicine?
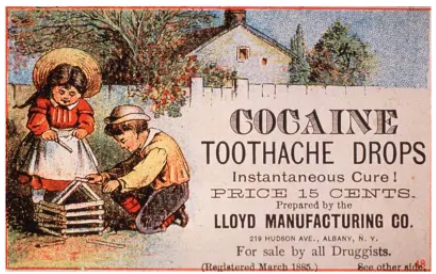
→ patent medicines
Ran parallel w/domestic medicine; complimentary
Touted as ‘cure-alls’ for range ailments/ afflictions
Often contained addictive/ habituating substances (alcohol, cocaine, opium…)
Efficacy (if any) limited; risks includ. addiction & illnesses related to other known ingredients.
Poss. to market ∵ limited govt oversight on drug safety (regulations to ensure manufacturers proved efficacy product they were advertis.)
medical marketplace
physicians
barber-surgeons
apothecaries
midwives
other healers
Top 3 classically focused on by historians
uni
no degrees - often perform same role as hairdressers (part same guild - both use knives, scissors)
EM version pharmacist - no diagnosis but social space for engag. w/medicine etc
go through apprenticiship
have some kind accreditation ← institution
all kinds people who make money out offer. healing but maybe don’t do so in way aligns w/occupational identity
transition aw. ← humoral & miasmatic theory → new ways understanding body & illn.: germ theory
scientific medicine
Body as biochemical organism
Most diseases caused by microorgamisms/ pathogens (bacteria, yeasts, viruses), infection
Allowed for more complex explanations that can be studied/ replicated in lab
Overturned 1000s yrs teaching & practice
Req. consid. step-change in how physicians approached disease & body
Shift slow & universal
Why did this transition occur?
important moment; recogn. labaratory research has practical benefit (doesn’t just happen in uni but can help patients)
How quick was the proc. shift?
Slow: took decades (1850s-80s)
Many stakeholders invested in older prevailing theories/ some physicians reluctant to change way seeing body & disease…
Humoral & Miasmatic theory grounded on 1000s yrs teaching & trad.
Medical schools had to change curriculum
Politics medicine
To bring ab. lasting change, needed new gen. physicians educated in germ theory…
What do missed opportunities along the way reveal ab. why this was?
1850s/60s: Ignaz Semmelweis (1818-65)
reception
signif. in proponing germ research
Hungarian physician, practiced Vienna 1840s
→ (Vienna Gen. Hospital) concerned ab. high incidence puerperal/ childbed fever
Noticed midwife births had lower incidence illn./ death than physicians’. difference bet. physician v. midwife births
Theorised infections being caused by unique practice physicians - some type contagion.
Believed correlation existed bet. physicians who undertook postmortem examinations w/someth. on their hands & instruments.
Termed contaminants cadaverous particles → refined to decaying animal-organic matter’
To remove particles, recommended washing hands w/chloride of lime before attend. to CB women
Theory poorly received by most physicians (believed disease caused by miasmas/ imbalance humors)
Many stakeholders invested in older prevailing theories (e.g. Hippocratic trad.) → info.
taken seriously & enacted upon.Shows level entrenchment Humoralism/Miasmatic theory; reveals politics medicine
Theory grounded in hospital archives & clinical observations/ notes; early beginnings evid.-based research
Early articulation germ theory disease
How universal was this shift?
Competition remained
Singular approach to medicine
Growth competitive medical marketplace/ remained whereby scientific medicine is 1 of many options avail. (compet. bet. those offer. care & patients seek. solutions): orthodox v. orthodox medicine
Some remain invested in/ persisted Hippocratic conceptions disease
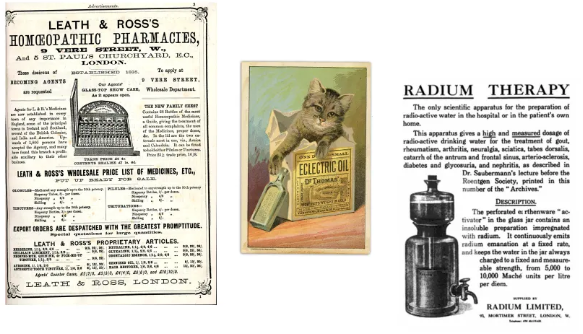
Water cures
Homeopathy
Radium therapy
Herbal remedies (home manuals)
Consumers selected 1/ more depending on exper. & preference.
patients might select multiple solutions to help them…
→ Soc. needed to invest in lab.s to make them viable…
importance lab
Scientific medicine = prod. bridging lab discoveries w/clinical medicine
BUT soc./culture had to be willing to accept evidence ← lab (i.e. linked to grow. status research)
Investment in medicine & science to allow suffic. momentum & resources
Growing professionalis. scientific disciplines (i.e. chemistry, physics...)
lab discoveries (1870s/80s)
Louis Pasteur (1822-95)
French chemist & biologist
Advanced theory microorganisms played role in causing illness; based on lab research in 1950s & 60s
Argued micro-organisms could be controlled through antisepsis (antisepsis killed bacteria)
His theory disproved miasmatic theory
lab discoveries (1870s/80s)
Joseph Lister (1827-1912)
British scientist & surgeon
(1850s/60s) Research into control micro-orgamisms on living tissues
Advanced techniques for applied antisepsis & wound management
Used carbolic acid to limit growth micro-organisms
Argued surgical equipment needed to be cleaned before use
lab discoveries (1870s/80s)
Rochert Koch (1833-1910)
German physician
(1870s/80s) Researched causative agents cholera, anthrax & TB
Developed techniques to culture bacteria for lab study, which helped to prove their relevance to medicine
lab study = so that other researchers could study them & reproduce the results
Helped to create methods to control contagious disease
What were outcomes transition?
reorientation doctor-patient rel.
strengthened lab-clinic connection
increased prof. esteem (increased specialisms & hierarchies in medicine)
power to influence ideology (prov. power to define ‘normal’, ‘disabled’ & ‘deviant’)
role clinic
outcomes transition
reorientation doctor-patient rel.
Medicine ab. study power (Foucault)
Pre-scientific medicine, patient might be involved in negotiating cause & diagnosis (knowl. co-creation)
W/scientific medicine, physician (as expert) drew on medical equipment & testing
Patient input reduced; patient power reduced (silenced)
scans, tests… things that could be done to body that only expert could know ab.
outcomes transition
strengthened lab-clinic connection
Grounded link bet. lab research & clinical applications
Data/ evid. that can be replicated → cornerstone to medical research
Labs as sites to create replicable data & evid. → pressure for human & animal experimentation to create new knowl.
→ new industry know. creation in lab (1880s & 90s)
outcomes transition
increased prof. esteem
(pre C19) Physician & surgeon consid. high-ranking occupations
W/science came esteem
Professionalisation: growth medical societies & claim to esoteric knowl.
Strengthened influence & power physicians; increased their power
Greater physician influence on policymak. & expert testimony
outcome transition
power to influence ideology
W/increased medical auth. emerged opportun. to shape ideology (ability to shape how soc. thinks ab. illness, disease & wider issues like politics)
Ideas somet. informed by assumptions & prejudices W physicians (often MC-UC white men, able-bodied & heterosexual), who had certain perceptions what it meant to be healthy
Background often influenced conceptions of:
female body
what was normal or deviant
disability/ ability
sexuality
definitions mental wellbeing & capacity
outcome transition
change role clinic/ hospital
Expansion hospitals: places to treat poor → sites to treat higher classes
As well as place to provide treatm. → create new knowl. (patients material for study physicians/ researchers: how they respond to treatments…)
Growth medical specialisations (specialist know.) & hierarchies
Places to train wider range health professionals: physicians, nurses, researchers & administrators
Whole apparatus around mangaging scientific medicine in clinic
case study how scientific medicine shaped CB: medicalised CB in USA (1900-50s)
How much did hospital births increase?
Why did physicians & expectant mothers seek CB in hospital?
(by 1940) 55% US births within hospital
(by 1950) 88%
(1960) Outside some isol. rural areas, alm. unheard of for American women to deliver their babies at home (R2)
UC & MC women increasingly sought institutional location for their confinements
concerns birthing women
medical professionalisation
urbanisation, immigration & industrialisation
Why did physicians & expectant mothers seek CB in hospital?
medical professionalisation spoke to concerns birthing women
pain & safety
Mystification medical knowl. in post-bacteriological era
(Judith Walzer Leavitt) Historians trad. focus on tak. advantage medical progress & convenience doctors
… BUT more image science’s pot. applied in hospital, lure safety & rationalism newest tech. & scientific methods could offer
Women recogn. risks CB ( fear severe pain CB + complications/ death to mother/ baby) & wanted best possible outcome: w/ physician’ claims special expertise over CB, hospital birth promised to alleviate these stresses/worries…
(by mid-to-late C19) Grow. knowl. germ theory → myth physicians could offer sterile environment reduce chance infection; home harder to sterilise
Avail. antibiotics, improvements in pain relief, surgical intervention & avail. blood transfusions (mid-1940s), range experts avail. for consultation in case complications
Promised modern, rational & scientific approach
(momentum to further medicalise CB continued into 1950s) New surgical techniques → growth in Cesarean births; og used for complicated births when the safety of mother/ baby in jeopardy
Popularised; promised to be less painful, could be scheduled, promoted as more ‘rational’ approach to CB
medical professionalisation spoke to concerns birthing women
Convenience: need to balance existing home/ caring demands with delivering a baby
quipm. & supporting staff → CB easier & less time-consuming)
Hastened by specialists’ attempts to wrest birth aw. ← gen. practitioners by systematising birth procedures within hospital setting: (’20s, ‘30s) part new move medical specialties to make obstetrics scientific, systematic & predictable by putting it under control specialist…
Systematic use pain-reliev. drugs, lab. inducers & tech. intervention (caeserean): women could plan when have baby & doctors could predict course lab.; controlled it (PS)
twilight sleep: sep. ← loved ones; fam. environm. controlled by others; cons. dur. parts her lab. & delivery - but gained protection for life & health… gave up some kinds control for others; new benefits seemed more important
Why did physicians & expectant mothers seek CB in hospital?
urbanisation, immigration & industrialisation
Declining ability women’s trad. networks to meet demands CB (social CB)
Urbanisation, immig. & industrialisation (migration rural → urban centres for work…) gave CB women less control over circumstances
Destroyed women’s larger social networks, partic. immigrants
Increased physical & social isol. left women
ableto find help they needed ∵supportive/ comforting home atmosphere/ less family/ friends avail. to help w/CB
Hospitals fill void & promise to fill level care
Despite perceived benefits, pot. risks…
+ check Notion for why doctors wanted hospitalised CB, even if not in their best interests…
Some surgical interventions could → health complications
Over-use equipment (forceps)
Specialist (OBGYN)
alw. avail.Cycle: use anaesthesia → increased instrumentation ∵ drugged women less effective @ push. baby out (1/4 hospital CBs operative) → increased hazard (R30)
Retrolental fibroplasia ∵ excess oxygen given to many premature babies in hospital
Until discovery & avail. antibiotics, risk infection remained
All delivery equipm. premise sterileNo. infected patients + crowded hospital nursery → cross infections
→ maternal mortality remained high in hospital
Emotional & psychological costs: loss female power/ concerns ab. how some women treated → women suffered severe psychol. dislocations
Safety hospital reliant upon reliability personnel: criminal negligence → deaths babies + degrading,
personaltreatm. (both PS)
Vuln. & ‘alone amongst strangers’ in alien hospital environm.
Loss privacy: teaching hospitals needed to train physicians; mother & baby could be observed/ subject to additional procedures for student training
Treatm. affected by classist & racial prejudices (food to be brought in, fam. to visit, specialist services…) - (Ann Rivington PS)
Fears/ cases baby swaps
Relative to your hospital… see diff. hospital types
(Prof. Harry & Ruth Bakin) ‘hospitals are suited for the care of the newborn’ find yr

diff. hospital types
certainly until 1950s/60s
still had to pay bill
outcome medicalised CB
CB → medical event
→ shift in power relations
(before) mother & immed. family retained most influence over birthing experience
(after) medical staff & physician
Where was the father? (Judith Walzer Leavitt’s Make Room for Daddy focuses on role men in birthing process
Often expectant father excluded ← attending CB f∵ trad., decorum & pot. contagion
More fathers invited into CB room since 70s
‘Nat.’ CB emerged as altern.
What does this case study reveal?
Useful to examine how scientific medicine applied in USA
Can see shift in power relations bet. patient & physician
Can see how ideas gender inform power structures
gender, race & class shaped nature care
What is a disease?
Why disease as a lens?
Studying MH ← perspective non-human actor
Where MH shares elements w/environmental history (can be activist/ negotiation & impact human & non-human)
Useful ∵ disease → remarkable human response:
indiv. response → trace fam. response → community response → trace state response
hence indiv. response useful
Us. disease as lens for human changes & how intersects w/
What poss. questions are asked?
giving agency to disease & ask. how affected human beings
agency to disease & impact on humans
questions getting @ reception disease to tell us lot more
Disease as a ‘lens’ developed by…
benefits disease as ‘lens’
limits to disease as ‘lens’
do we trust source/ person carrying out reporting (did they know what they were talk. ab.)
regional variation: what might be reported as disease in 1 area might not be in another

Treatments for disease are shaped by…
medical & scientific
Knowl. disease & how it affects body
Nature medical technologies (screening)
Treatm. infrastructure (hospitals, clinics, home)
social & political
perception the disease (worthy sympathy?)
financial outlay (who pays bill/ how m/)
race/ class/ gender: does this affect access to treatm./ how people treated?
is condition stigmatised (STIs, certain
abilities)
Studying a past soc.’s response to disease reveals how treatments are socially defined
How is this the case?
Perceptions disease/ treating body sit in isol., alw. rooted in best clinical knowl./ outcome patient
Instead, products people (physicians, nurses, fam., etc) w/their own values, ideas, traditions, debates, hierarchies, predjucies & knowl. their soc.
Those responses can tell historians lot ab. past soc. ∵ everyone can get ill
Disease useful reflective element for social responses
When we → ill, we lose some power; other people’s powers enacted on our bodies (we trade some power to indiv. caring for us)
Shows values soc. & how it approaches disease
Part transnat. knowl. exchange
Treatm. discoveries in 1 part world spread to others
e.g. smallpox (discoveries China → Turkey → England)
Cholera (discoveries England → USA)
Studying a past soc.’s response to disease reveals…
understandings body & disease
perceptions patients & survivors
doctor-patient rel.
nature medical & scientific tech
social values, hierarchies, ideas, prejudices
differences in treatm. based on race, class, gender, religion, sexuality…
polio as lens
What does response in USA tell us?
oral-fecal disease caused by virus & spread by contaminated surfaces & water
anyone could → infected BUT polio had affinity for kids ∵ their developing immune systems (initially called infantile paralysis)
How characterised
Polio consid.
visiblethreat (often anthropomorphised as spectre stalking playgrounds)
How soc. responsed
Inspired lot fear soc. ∵ hard to prevent infection before vaccine licensed 1955
Use chemicals
communities sprayed DDT in hope would ward off contagion
Nature public health
Some neighbourhoods undertook fly eradication programmes
How funded/ how econ. factored in
Debates over amount funding for treatm.; who paid for polio care in soc. embraced priv. medicine?
Charity, fam. or govt?
Who blamed
Children erroneously deemed primary carriers & subject to restritions
Signs: (c.1940s/50s) children under 16 not allowed to enter this town
Understandings causation
Many debates as to causation (swimming in contaminated water; too m/sugar, fluoride in drink. water, etc…)
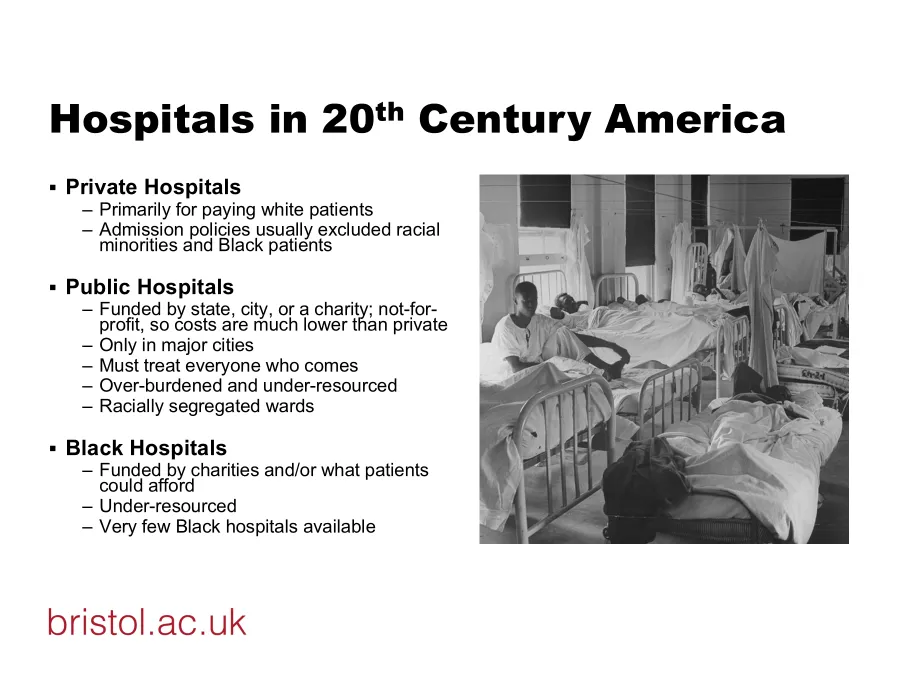
Race
Disease racilaised (framed as white disease).
Acute treatm. prov. in racially integrated wards (cost-effective); convalescent care in segreg. wards
shows us how segreg. functioned in USA: messin. racial segreg.
Ability
Survivors had to adapt to lasting disability in nation
accommodated for disabled
Consid. stigma
Seen as perenially contagios
State medical research
Scientists debated best way to control disease (diet, vaccines, isol. dur. epidemics)
Jake Paralysis as lens…
nature politics justice
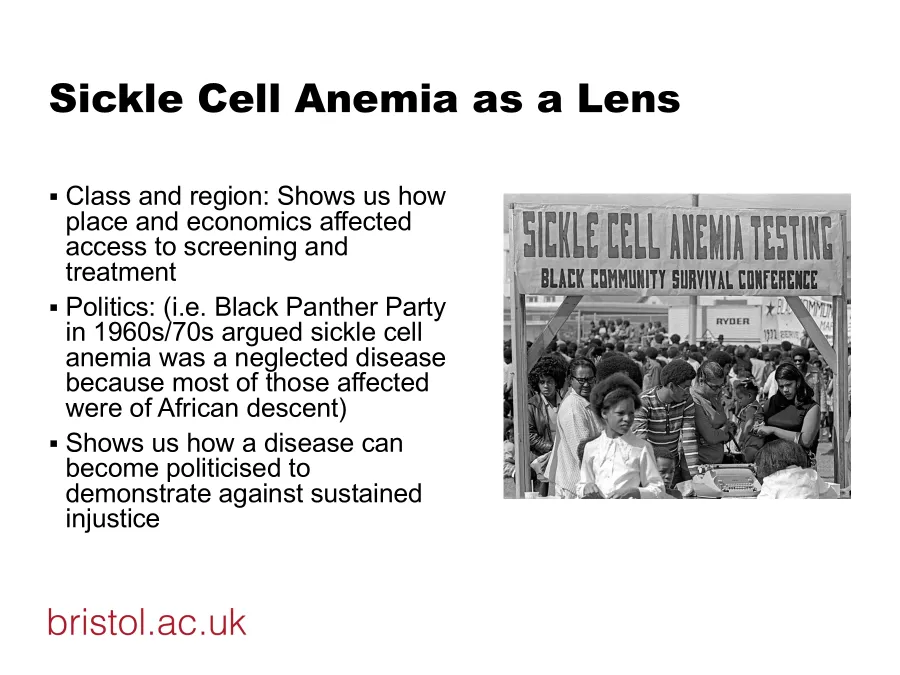
Sickle Cell Anemia as lens race
marginalised; those most affected were African-Americans
HIV/ AIDs as lens
medical knowl.
as ‘new’ disease, few physicians & nurses adequately prep. to prov. supp. → treatm. for patients remained limited
political
Reagan administration initially ignored public health crisis
treatm.
shows how prevailing prejudices tow. homosexuals in USA 1980s affected delivery care, treatm. & research
approach to discussins ab. sex
shows gen.
comfortdiscussing matters sex & STIs (stigmatised)
public health
fixation on identifying ‘patient zero’,
exam. wider impact & prevent.shows how public health officials thought needed to locate source to underst. disease & attrib. blame (responses to disease → create box, narrow their POV)
shows nature politicisation via health activism
role families & survivors in rais. awaren. & demand. govt response
can assess govt response
be wary retrospective diagnosis…
define + why
proc. classifying past illn. us. modern knowl. & methods
Poses distinct chall. for medical historians
Approach sources w/caution… knowl. body & disease changed consid. over time & place
Source problem: how do we know we’re discussing same thing? Can we trust source?
retrospective diagnosis
syphilis
diffic. to identify in historical documents
got to ensure talk. ab. same things
may be underreported
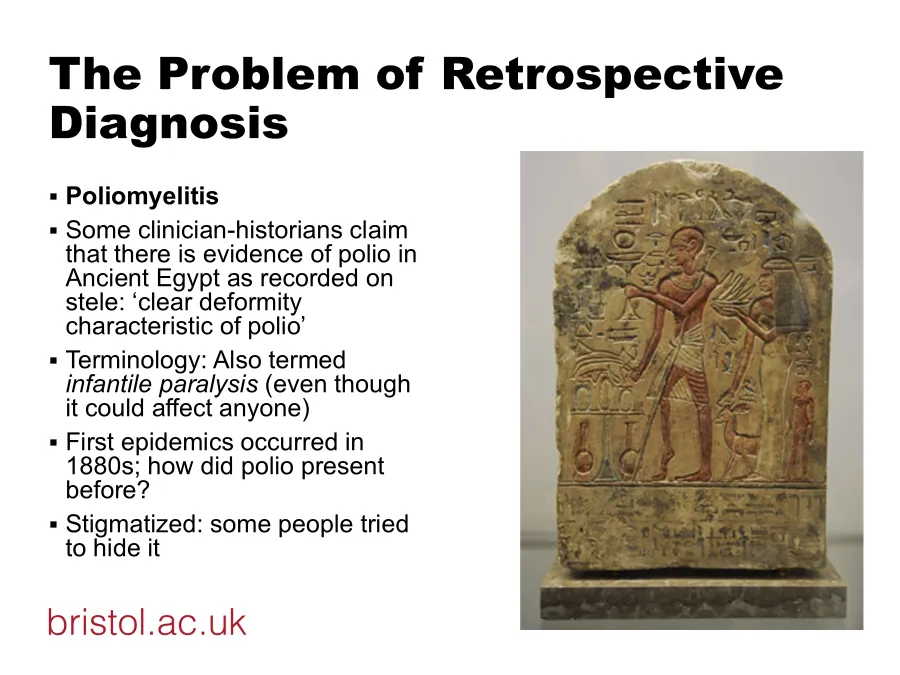
retrospective diagnosis
poliomyelitis
way he limps - this man polio survivor?
how do we account for earlier case studies?
retrospective diagnosis
TB
How to avoid risk retrospective diagnosis in historical evid. & 1st-person accounts
written by orthodox physician, patient…
is there way can corroborate the source?
how did it affect how people wrote ab. it? Did they shroud it in euphemisms?