Protein Electrophoresis (PEL)
1/39
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
40 Terms
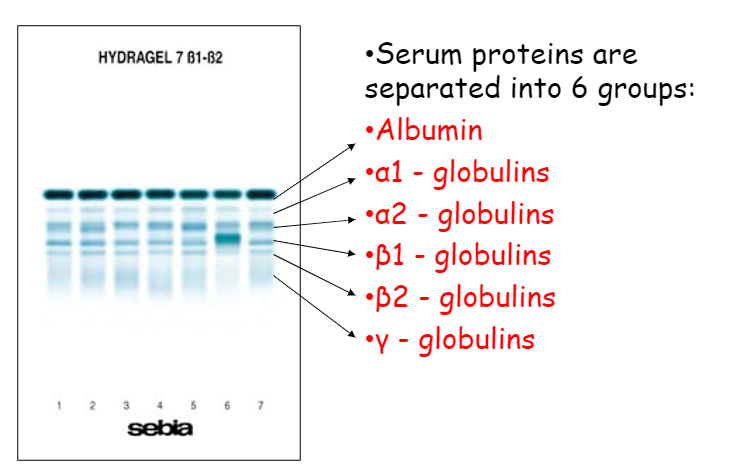
plasma protein distribution
60% albumin
35% globulin
4% fibrinogen
1% other
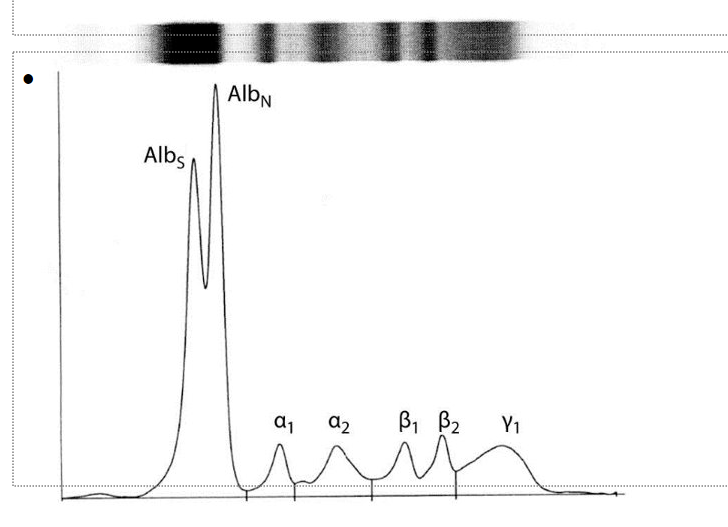
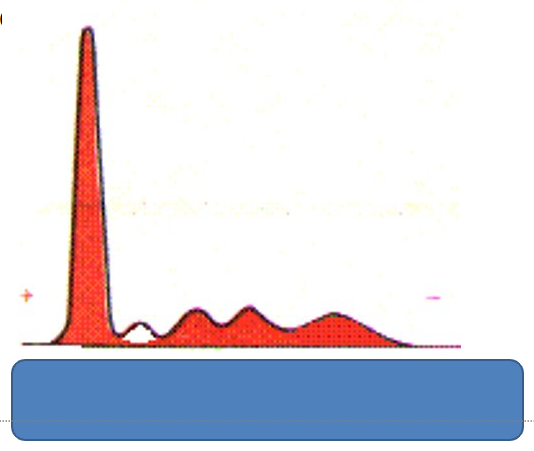
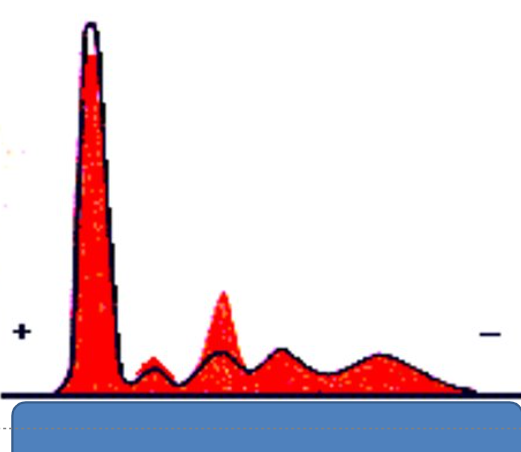
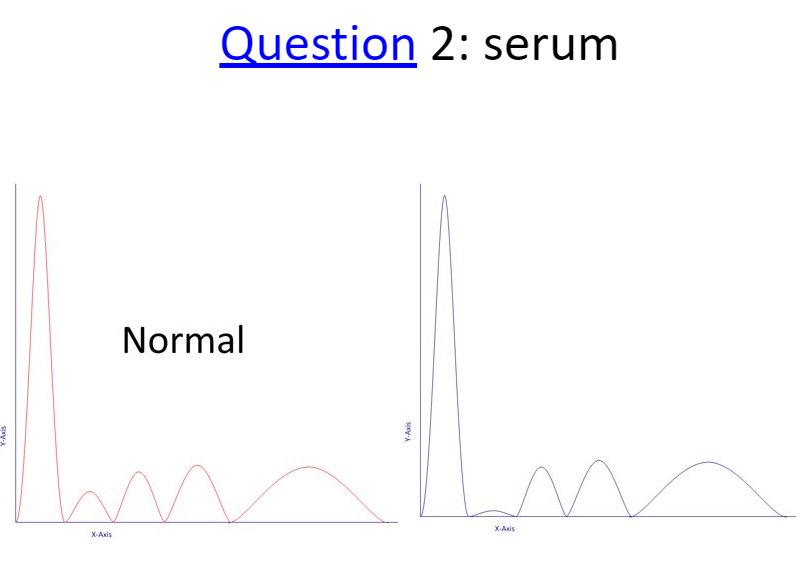
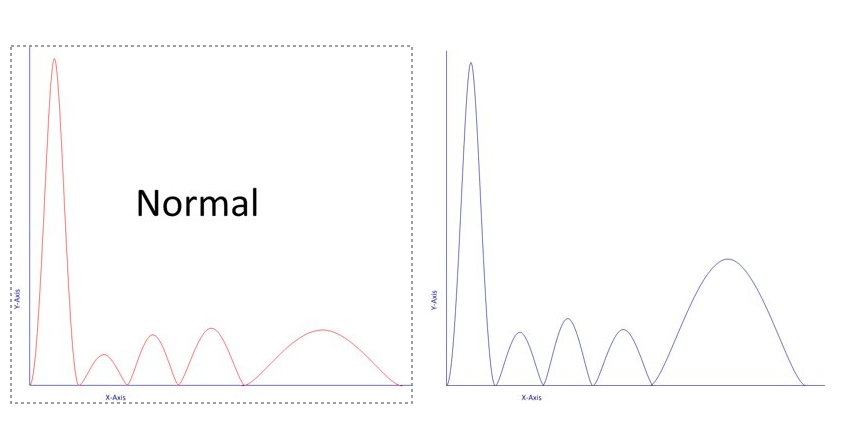
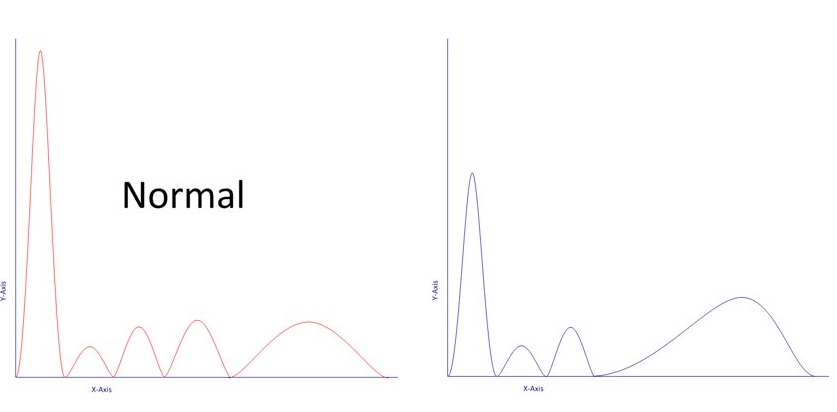
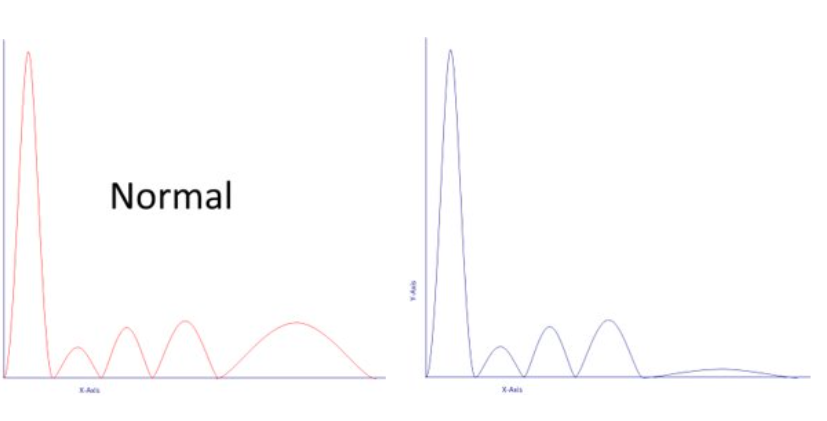
serum PEL
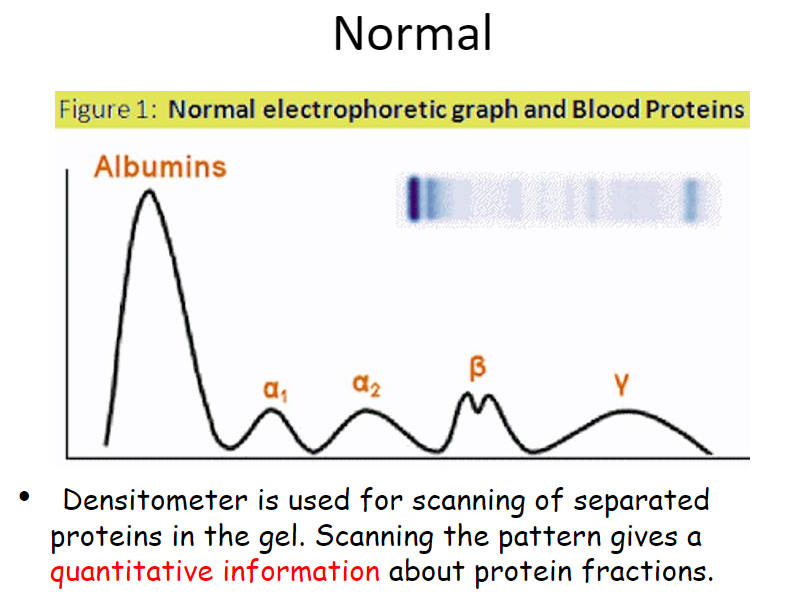
normal PEL graph
hypoalbuminemia
less production by liver / liver dz
inc loss or degradation
malnutrition
hormone therapy
pregnancy
alpha 1-antitrypsin (a1-AT)
if a1-AT defic → liver (cirrhosis) & lung (emphysema) dz
thyroid-binding globulin inc/dec
alpha acid glycoprotein - ulcerative colitis
malignancy & acute inflammation (acute-phase reactants) can inc the alpha1 protein band
alpha 2
ceruloplasmin - copper transport - dec in Wilson’s vs Menke syndrome (eye w golden ring)
alpha 2 macroglobulin - liver & renal dz → large size prevent loss from renal & inc production by liver
haptoglobin - absent in intravascular hemolysis
inc as APR
selective protein loss
long term loss of albumin & IgG in kidney
dec albumin, inc a2 & B globulins
nephrotic syndrome
beta 1
transferrin
inc in Fe defic
asialated transferrin - when transported into CSF leading to double transferrin peak
in microcytic anemia
due to iron defic - TF inc, ferritin
or chronic dz - no clear inc/dec
beta 2
fibrinogen: pseudoparaprotein, incomplete clot - heparinized pt (use EtOH to ppt out)
CRP: inflammation > 10, hs
CRP 2-3 = 3x risk for ACS
IgA
Gamma
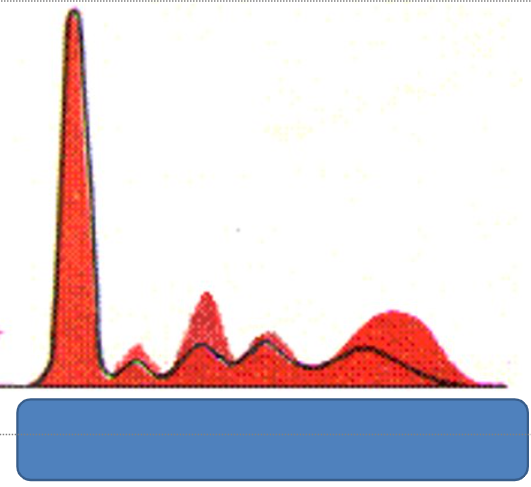
acute/chronic inflammation
IgA/G/M or D/E ?
acute inflammation
inc a1 & a2 globulins
often w dec albumin
due to infn, injury, surg trauma
chronic inflammation
inc gamma globulin
inc a2 globulins
± a1 globulins
dec albumin
in autoimmune dz, chronic liver dz, chronic infn, malignancy
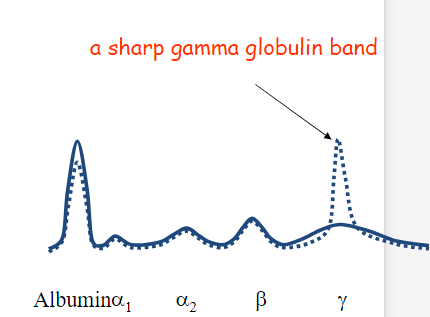
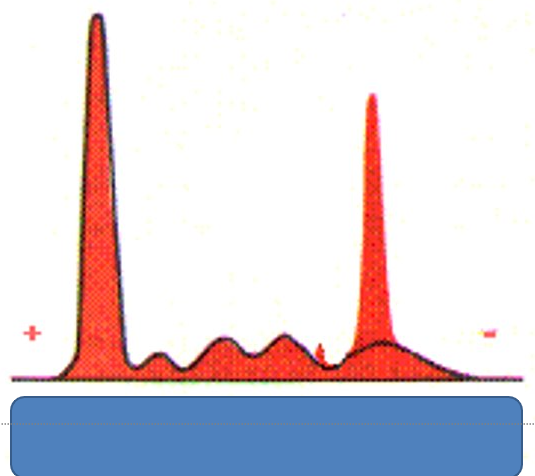
monoclonal gammopathy
alter B-cells produce an abnormal Ig paraprotein → assoc w benign monoclonal gammopathy & multiple myeloma
monoclonal gammopathies
most IgG > M > A > > light chain only »D/E
adverse properties of Ab
1.ability to agglutinate rbc
insolubility at low temp (cryoglobulinemia)
inc viscosity (Waldenstrom macroglobulinemia)
deposition in tissues w resulting organ dysfunction (eg AL (light chain) amyloidosis or Ig deposition dz
neuropathy
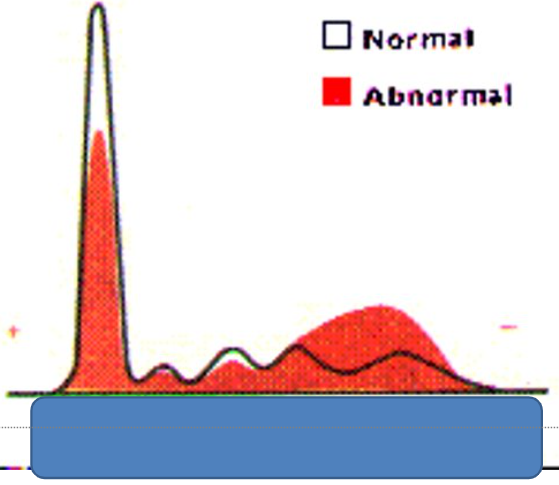
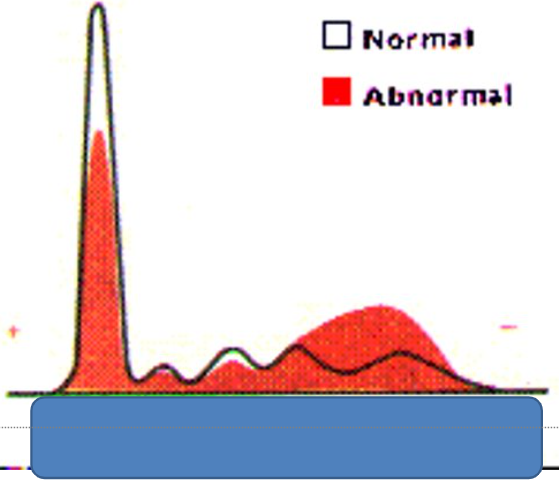
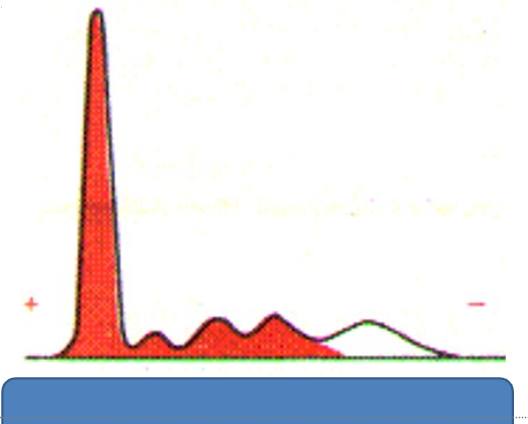
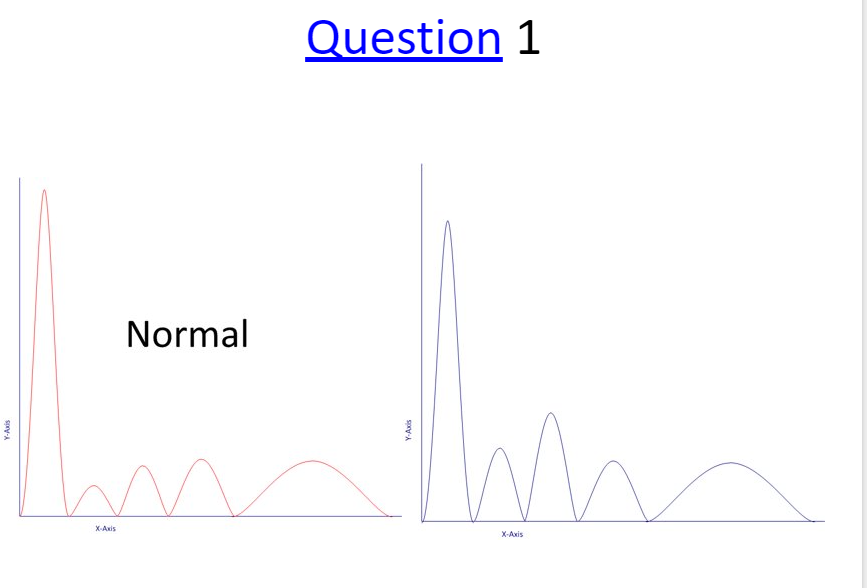
Beta-Gamma bridging
polyclonal inc in IgA extending into beta region
this pt also shows dec albumin
cirrhotic liver dz
malignancy
inflammatory dz
normal variant → do nothing
a1-antitrypsin
nephrotic syndrome??
beta gamma bridging - inc of IgA
also dec albumin
acute phase reactants
chronic inflammation
immunosuppressed / deficient
hypogammaglobulinemia
congenital or
acquired
multiple myeloma
primary amyloidosis
CLL
lymphoma
nephrotic syndrome
monoclonal gammopathy
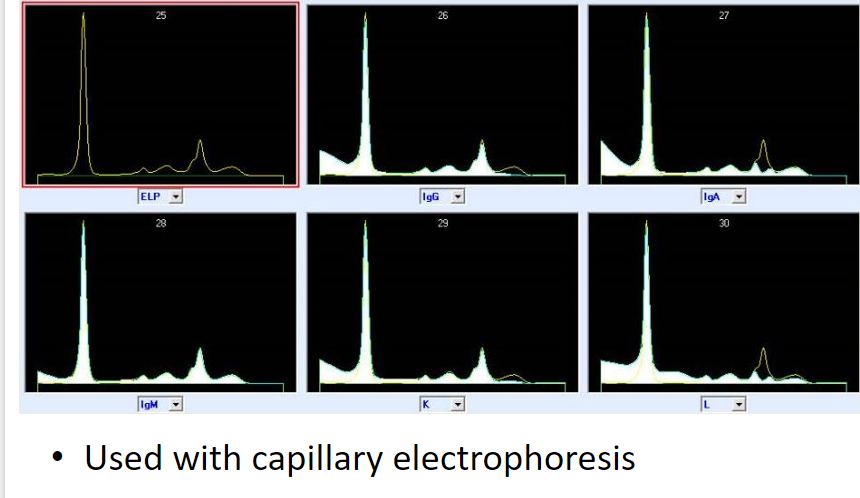
immunofixation (IgM kappa)
permits detection & typing of monoclonal Ab or Ig in serum or urineim
immunotyping (capillary electrophoresis)
myeloma categories
MGUS < 3 g
smoldering > 3 g
MM > 3 g & clinical symptoms
multiple myeloma
CRAB
Calcium
Renal dz
Anemia
Bone lesions
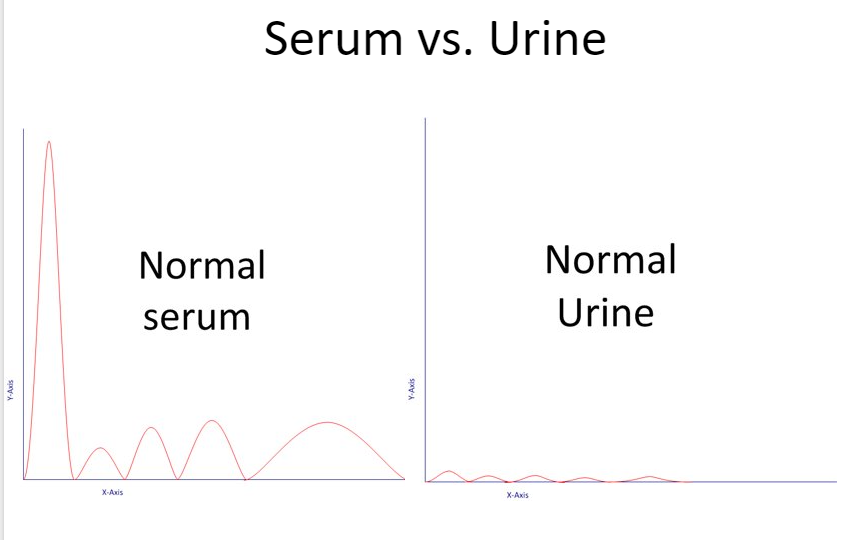
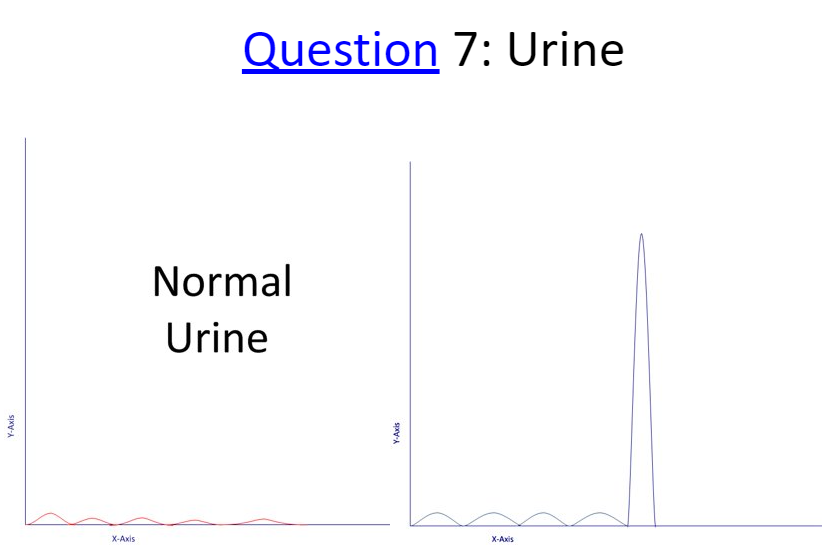
urine PEP
help dx & monitor MM
may be ordered as f/up to otehr lab tests ie abnormal total protein & or albumin level
** urine PEP is more sensitive than serum PEP
usually ordered in difficult cases
serum vs urine PEP graph
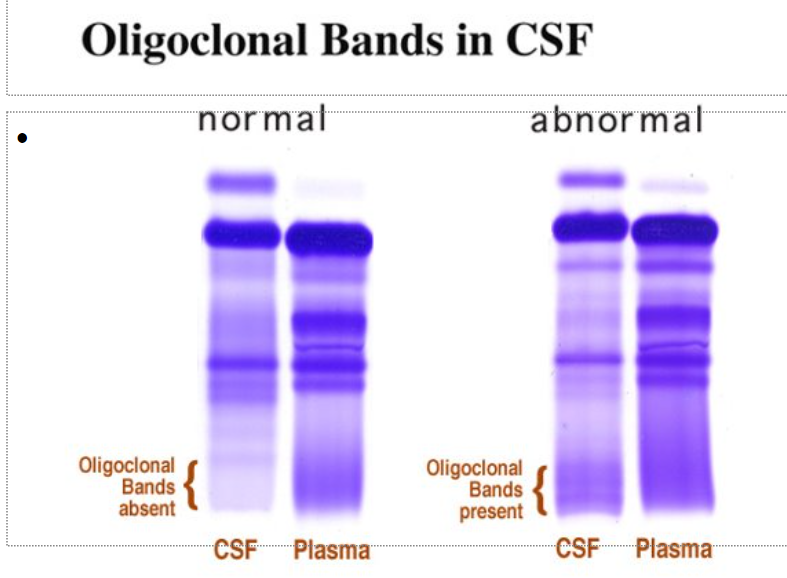
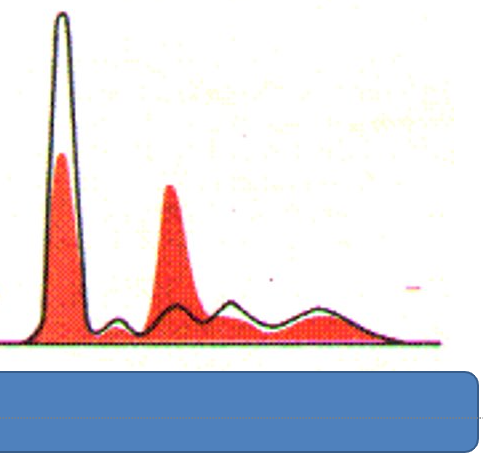
CSF contains all proteins present in serum smaller quantities
char features
prominent pre-albumin bnad
double beta transferrin band
most pt w multiple sclerosis have permanently observable oligoclonal bands - 2 or more bands in CSF & no bands in the serum
multiple sclerosis
sine qua non of MS is symptomatic ep are “separated in space & time” ie occur months/years apart ie weak arm → can’t control baldder
acute phase reactants
a1-antitrypsin → damages liver/lungs
chronic inflammation
Beta-Gamma bridging
immunodeficient or myeloma
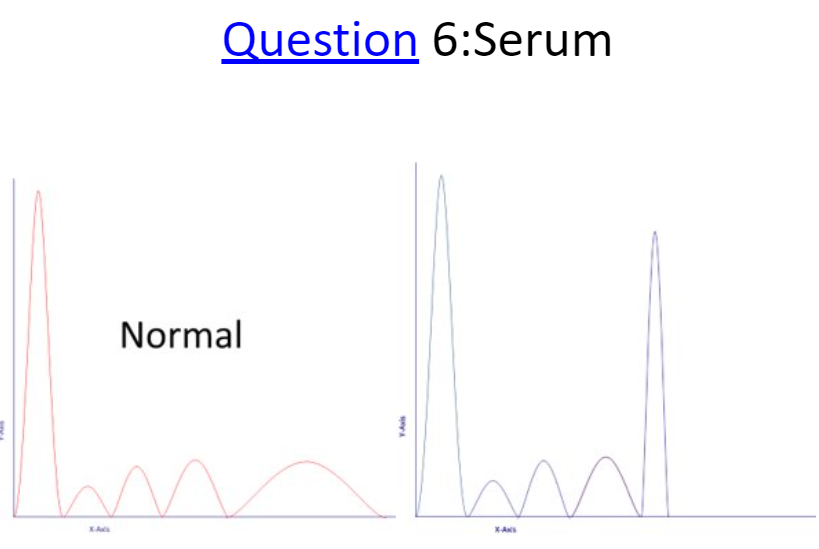
multiple myeloma
myeloma