MLS 2213 Unit 13
1/105
Earn XP
Description and Tags
TDM and tox
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
106 Terms
What are the three primary goals of toxicology in a clinical setting?
Detect poisoning by “Over The Counter” drugs
Detect presence of “recreational” drugs
Detect abuse of Prescribed Drugs
Under what conditions is a qualitative toxicology assay performed versus a quantitative one?
Qualitative if drug level does not affect treatment
Urine and/or Serum
Quantitative if treatment IS based on concentration
Quantitation only valid for serum/plasma levels
How many doses are required to reach Steady State
5
Why is TDM only done during a steady state?
To determine if the patient is within the therapeutic range
What is a linear doseage response
Double Dose = Double Blood Level
1 Yeller Pill/Day = 10 ug/mL 2 Yeller Pills/Day = 20 ug/mL
If you need to reduce blood level 1/3, decrease dosage by 1/3.
What is a non-linear drug response
Double Dose does NOT double blood level.
1 Yeller Pill/day = 10 ug/mL 2 Yeller Pills/day = 15 ug/mL or 27 ug/mL
What drugs show a non-linear response?
Dilantin, Cyclosporine, Tacro-II, Theophylline
What is first order kinetics
Elimination stays fairly-well matched with drug intake.
Increase Dosage = Increase in excretion.
Must continually increase dosage to say in Therapeutic Range
What is zero order kinetics
Elimination does not keep pace with Drug Intake.
e.g. Alcohol, Dilantin, Aspirin do this.
Very easy to create Toxicity
List the five components of pharmacokinetics that determine a drug’s blood level.
Bioavailability
Absorption
Distribution in body
Metabolism
Excretion
How do blood albumin levels influence drug distribution and the risk of toxicity?
Low albumin = More Free Drug = Toxicity
How does age of the patient affect drug metabolism
Young = Fast Metabolizers
Old = Slow Metabolizers
Puberty? (Slow Steroid metabolizers)
How does acidosis affect the excretion of alkaline versus acidic drugs?
Acidosis = More excretion of alkalines
= Less excretion of acidics
At what specific time should a trough level specimen be drawn?
Troughs should be drawn immediately before the next dose of drug is given.
what is the required relationship between a peak result and a trough result if both are assayed?
If Peaks and Troughs are both being assayed, the Peak has to be higher than the Trough.
Name 3 aminoglycosides
Tobramycin, Gentamycin, Vancomycin
What are the nephrotoxic and ototoxic effects of aminoglycosides
Nephrotoxic
Interstitial Nephritis
Toxic to 8th Cranial Nerve
Ototoxicity – deafness, ringing of ears, loss of balance.
What serious hematologic condition can develop in 10% of patients using chloramphenicol
Aplastic anemia
What are the handling requirements for methotrexate
Temperature sensitive (freeze)
Light Labile (protect from light)
Explain the purpose of the Leucovorin Rescue procedure.
Patient is given an almost lethal dose of methotrexate then given leucovorin
How do potassium (K+) levels influence the action of digoxin
Low K+ = Increased action
High K+ = Decreased action
What are the major signs of Digoxin toxicity
Nausea and vomiting, blurred vision, Pounding in Ears, AV-Heart block = Death!
What is theophylline used to treat
Asthma and emphysema
What are the symptoms of theophylline toxicity
Headache, tachycardia, dizziness, nausea, insomnia, irritability, convulsions, seizures, strokes
What is the therapeutic range for Lithium, and how close is it to the toxic threshold?
Toxic above 1.5 mMol/L
Therapeutic Range is 0.7 – 1.5 mMol/L
Why must EDTA whole blood be used for testing Cyclosporine-A and Tacrolimus?
50% bound to RBCs, so specimen is EDTA Whole Blood
What drugs are considered anti convulsants
Phenytoin (Dilantin)
Carbamazepine (Tegretol)
Valproic Acid (VPA)
Primidone (and Phenobarbital)
Phenobarbital and cousins (Pentabarbital, Secobarbital, etc.)
Ethosuximide
Which analytes are typically included in a Serum Emergency Toxicology Screen?
Ethanol
Salicylates
Acetaminophen
TAD (Tricyclic Anti-depressants)
Benzodiazepines (can be done in urine)
Osmolality (check Osmolal Gap)
Which drugs are better detected in a Urine Screen due to their short half-lives?
Stimulant Amines - (Short half-life)
Benzedrine, Dexedrine, Amphetamines, Methamphetamines
Opiate Metabolites – (Short half-life)
Heroin, Morphine, Codeine, Papaverine (pin-point pupils is the flag)
Cocaine Metabolites - (Short half-life)
Cocaine and Crack
At what serum level is iron considered critical, and at what level is it lethal
Above 500 ug/dL Critical
Above 750 ug/dL Lethal
How is exposure to organophosphates measured?
Cholinesterase Activity
What is the binding affinity of CO to hemoglobin compared to oxygen?
binds to Hemoglobin with 250 x binding affinity as Oxygen.
What is the characteristic visual appearance of the blood in CO poisoning
Bright cherry red blood
Which organ systems are primarily damaged by toxic levels of salicylates and acetaminophen?
Salicylate - Nephrotoxic
Acetaminophen - hepatotoxic
What is the goal of TDM
Optimize medication levels to maximize therapeutic effects for patients.
Minimize incidence of Toxicity or ineffective, low blood levels.
What is the goal of toxicology
Detect poisoning by “Over The Counter” drugs
Detect presence of “recreational” drugs
Detect abuse of Prescribed Drugs
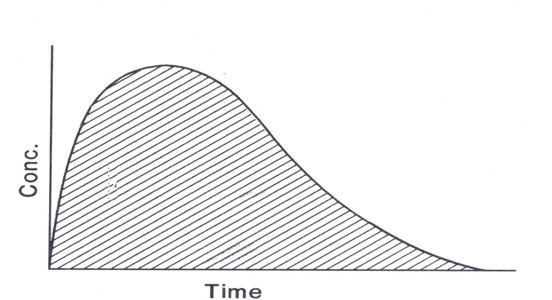
What is the blood concentration of a single dose administration
What is the blood concentration of a multiple dose drug administration
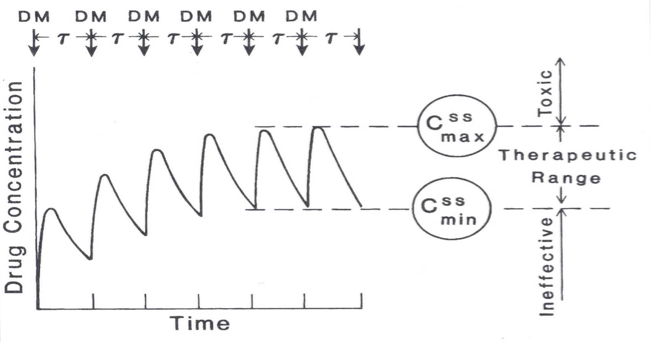
What is a steady state?
Peaks and Troughs continue to rise with each dosing for first 5 doses.
Steady State is reached after 5 Doses of drug.
What is MEC?
Minimum effectiveness concentration
What is MTC?
Minimum toxicity concentration
What is a peak sample?
Peak if patient shows signs of Toxicity right after dosing.
Peak if patient is on a short-half-life drug.
Peak to check for patient compliance
What is a through sample?
Trough for drugs with very long half-lives.
Troughs if patient doesn’t appear to be responding to drug, and compliance is not an issue.
You check troughs to assess MEC issues.
When should a trough be collected
Troughs should be drawn immediately before the next dose of drug is given.
When should a peak be collected
Peaks usually 1 – 4 hours after dosing, for oral dosing.
Peaks usually 30 minutes after dosing for IV administration
How does bioavailability of the drug effect patient blood levels and dosage?
Oral, suppository, IV, IM ?
Ionized or Un-ionized?
Gel Cap or Capsule
How much of the drug actually enters the blood stream and at what rate
How does the absorption into the GI tract of the drug effect patient blood levels and dosage?
Pregnant? (decreased absorption)
Diarrhea? (Whoa!!! – less absorbed)
Constipation? (increased absorption)
How does the distribution of the drug to tissue receptor sites relative to the binding ability of plasma proteins effect patient blood levels and dosage?
Water Soluble or Protein bound?
Blood Albumin levels?
Low albumin = More Free Drug = Toxicity
How does the metabolism by the liver of the drug effect patient blood levels and dosage?
Metabolism by the liver alters how much of the drug is active in the bloodstream; it can convert drugs to active or inactive forms, affecting therapeutic effects and potential toxicity.
How does age effect patient blood levels and dosage?
Young = Fast Metabolizers
Old = Slow Metabolizers
Puberty? (Slow Steroid metabolizers)
What is first order drug kinetics
Elimination stays fairly-well matched with drug intake.
Increase Dosage = Increase in excretion.
Must continually increase dosage to say in Therapeutic Range
What is zero order drug kinetics
Elimination does not keep pace with Drug Intake.
e.g. Alcohol, Dilantin, Aspirin do this.
Very easy to create Toxicity
Why do some drug levels need to be tested for the actual drug and the metabolites in the blood?
Both Parent drug and Metabolite have metabolic activity.
e.g. Primidone and Phenobarbital
Procainamide and N-Acetyl Procainamide (NAPA)
What are aminoglycosides used for and what are some examples?
Antimicrobials
Tobramycin, Gentamycin, Vancomycin
What are Chloramphenicol used for and what are some examples?
Older antimicrobial not used commonly today
Chloromycetin
What are lidocaine used for and what are some examples?
To resist ventricular fibrillation
Xylocaine
What are methotrexate used for?
Antineoplastic and immunosuppressive agent, chemo
What are theophylline used for
Asthma and emphysema
What are digoxin used for
Slows and steadies the heart rate, used for CHF patients
What is lithium used for?
Used for manic-depressive illness
What are cyclosporine-A (CYA) used for
Big gun anti-rejection drug.
What are Tacro-II used for and what are some examples?
Second Generation Anti-rejection drug
Tachrolumus, FK-506
What are some toxic effects of aminoglycosides?
Nephrotoxic
Interstitial Nephritis
Toxic to 8th Cranial Nerve
Ototoxicity – deafness, ringing of ears, loss of balance.
What are some toxic effects of chloramphenicol?
Rots Stem Cells in Bone Marrow
10% develop transient Aplastic Anemia
20%of these become chronic.
What are some toxic effects of lidocaine?
Bradycardia, Cardiovascular collapse, Cardiac Arrest, Low BP, Dizziness, Blurred Vision, Nausea are signs of Toxicity
What are some toxic effects of methotrexate?
Rots Liver, Bone Marrow, Kidneys
What are some toxic effects of theophylline?
Headache, tachycardia, dizziness, nausea, insomnia, irritability, convulsions, seizures, strokes
What are some toxic effects of digoxin?
Nausea and vomiting, blurred vision, Pounding in Ears, AV-Heart block = Death!
What are some toxic effects of lithium?
Muscle tremors, twitching, ataxia, that can result in life-threatening seizures
What are some toxic effects of cyclosporine-A?
Rots everything if toxic, reject transplant if too low.
What are some toxic effects of Tacro-II?
Rots everything – more toxic gram-per-gram than CYA, but takes less drug.
What are some anti convulsants?
Phenytoin (Dilantin)
Carbamazepine (Tegretol)
Valproic Acid (VPA)
Primidone (and Phenobarbital)
Ethosuximide
What are some arrhythmic agents?
Digoxin and Digitoxin
Quinidine
Procainamide (and NAPA)
Lidocaine (Xylocaine)
Disopyramide
Propranolol
What are some benzodiazepines
Chlordiazepoxide (Librium)
Diazepam (Valium)
Oxazepam (Serax)
Alprazolam (Xanax)
Prazepam (Centrax)
Lorazepam (Ativan)
Flurazepam (Dalmane)
What are some tricyclic anti-depressants
Amitriptyline (Nortriptyline)
Imipramine (Desipramine)
Doxepin (Desmethyldoxepin)
What are some analgesics?
Salicylates (Aspirin)
Acetaminophen (Tylenol, etc.)
Which drugs would be in a UDS?
Stimulant Amines - (Short half-life)
Benzedrine, Dexedrine, Amphetamines, Methamphetamines
Opiate Metabolites – (Short half-life)
Heroin, Morphine, Codeine, Papaverine (pin-point pupils is the flag)
Cocaine Metabolites - (Short half-life)
Cocaine and Crack
Which drugs would be in a serum drug screen?
Ethanol
Salicylates
Acetaminophen
TAD (Tricyclic Anti-depressants)
Benzodiazepines (can be done in urine)
Osmolality (check Osmolal Gap)
What are some examples of stimulant amines
Benzedrine, Dexedrine, Amphetamines, Methamphetamines
What are some examples of opiate metabolites
Heroin, Morphine, Codeine, Papaverine
What does CO2 form when bound with oxygen?
Carboxyhemoglobin
What drug might be used for an emphysema patient?
Theophylline
One of these drugs is not like the other! As in, it's used to treat something that the others don't. Select the odd drug in this group.
Propranolol
Valproic Acid
Phenytoin
Carbamazepine
Propranolol
Illusions of grandeur are a common side effect of this drug of abuse:
phencyclidine
What specific type of specimens (serum or urine) should Stat Toxicology Screens use, and should they be quantitative or just qualitative?
Urine and Qualitative
When looking at how drugs are eliminated from the body, what is it called when the elimination rate increases as the drug dose goes up?
First order
A telemetry patient is currently on Primidone for the last five days. However, the nurses are suspecting toxicity due to behaviors they have witnessed. The lab is called and TDM testing is ordered to be drawn 30 minutes before the patients next dose. What is the metabolite of this drug?
Phenobarbital
One of these drugs is not like the other! As in, it's used to treat something that the others don't. Select the odd drug in this group.
Quinidine
Doxepin
Amitriptyline
Imipramine
Quinidine
Jack Bolono is being treated by the following three medications, and must have TDM monitoring for all of them: Carbamazepine, Procainamide, Diazepam. In looking at what TDMs are ordered for Jack, you notice a fourth drug on his TDM order. What other drug is being test?
NAPA
Jack Bolono is being treated by the following three medications, and must have TDM monitoring for all of them: Carbamazepine, Procainamide, Diazepam. Which of the following conditions are NOT associated with treatment using those drugs?
Depression
A telemetry patient is currently on Primidone for the last five days. However, the nurses are suspecting toxicity due to behaviors they have witnessed. The lab is called and TDM testing is ordered to be drawn 30 minutes before the patients next dose. What type of sample does that represent in TDM testing?
Trough
There are three brothers: Mo, Larry, and Curly. Each brother has a history of suffering numerous and fairly severe seizures. Each brother uses a different physician than the other two. Here is what medication they are taking: Mo is taking Phenytoin. Larry is taking Propranolol. Curly is taking Carbamazepine.
Which brother is taking the incorrect medication for their condition?
Larry
A telemetry patient is currently on Primidone for the last five days. However, the nurses are suspecting toxicity due to behaviors they have witnessed. The lab is called and TDM testing is ordered to be drawn 30 minutes before the patients next dose. Testing is performed and resulted as: 9.5 ug/mL. Therapeutic range = 5-10 ug/mL, and Toxic above 10 ug/mL. Should the next dose of the drug be administered as scheduled?
No, the patient is right below the toxic range so another dose puts them in danger of being in the toxic range
Is a patient who is in "steady state" for medication administration also considered to be in the therapeutic range?
No, we can't assume the patient is in the therapeutic range so we must run TDM studies
You and Jayson Clark are having a discussion about TDM and Toxicology. Jayson doesn’t know the top three (3) reasons that physicians order TDM testing. Which if the following is NOT a reason to order TDM testing?
Guard against Under-medication
Guard against Toxicities
To establish the drug’s therapeutic range
Document Patient Compliance of taking medications
To establish the drug’s therapeutic range
What is the specimen of choice for drugs of abuse in the emergency room?
urine
One of these drugs is not like the other! As in, it's used to treat something that the others don't. Select the odd drug in this group.
Alprazolam
Propranolol
Diazepam
Chlordiazepoxide
Propranolol
One of these drugs is not like the other! As in, it's used to treat something that the others don't Select the odd drug in this group.
Digoxin
Ethosuximide
Propranolol
Lidocaine
Ethosuximide
Jack Bolono is being treated by the following three medications, and must have TDM monitoring for all of them: Carbamazepine, Procainamide, Diazepam. In looking at what TDMs are ordered for Jack, you notice a fourth drug on his TDM order. Why is there an additional drug on his lab ordered?
Because that particular drug has a metabolite that is just as active as the drug so it must also be monitored.
What are the generic drug names for Dilantin and Tegretol?
Phenytoin and Carbamazepine