Antibiotic Use for Ocular Conditions Cases
1/18
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
19 Terms

What is the illness script of an internal hordeolum?
Epidemiology: patients of any age with no predilection for gender
Temporal pattern: acute, possibly recurrent
Syndrome statement: Unilateral swollen eyelid with a localized area of redness contained within a meibomian gland that is soft, warm, and tender to the touch. Pt are afebrile and may show additional signs of blepharitis.

What is prescribed to treat internal hordeolums?
DOC: Augmentin 500mg tablets; 20; take one by mouth twice daily for 10 days; No refills
DOC: Cefprozil 250mg tablets; 20; take 1 by mouth 2x daily for 10 d0ays; No refills
If PCN peds allergy, Azithromycin 500mg tablets; 3; take 1 by mouth daily for 3 days. No refills
If PCN adult allergy, Bactrim DS 800/160mg tablets; 20; take 1 tablet by mouth every 12 hours for 10 days; No refills
(Same Tx for preseptal cellulitis)

What are other management issues for patients with internal hordeolums?
Warm compresses to increase blood flow
Do not rub, pop, massage, express it. Can rupture and turn into preseptal infection
Typically, no follow ups scheduled, but inform patient to return if worsens/ no improvement after 10 days

What are the rules to determine if we culture or not?
1,2,3 rule, where culture if any of the following exist:
1+ or greater anterior chamber cells
2mm dense infiltrate
The edge of a large, central infiltrate is within 3mm of the center of the cornea
What clinical features suggest a likely infectious corneal infiltrate?
Single lesion
Central 6mm in location
Greater than 1mm in size
Staining size = lesion size
Severe Pain
Diffuse Injection
Cells in AC
What clinical features suggest a likely sterile corneal infiltrate?
Can be multiple
Peripheral in location
Less than 1mm in size
Staining area < lesion size
Mild to moderate pain
Localized injection
No/rare cells in AC
What is the illness script of Marginal Keratitis?
Epidemiology: adults > children; males = females
Temp pattern: acute, sometimes recurrent
Syndrome statement: presents with unilateral or rarely bilateral red eye with mild to mod symptoms of pain/irritation, tearing, and photophobia. Exam reveals single or (more likely) multiple peripheral corneal infiltrates/ulcers with no or mild staining. There is often localized conj injection near the limbus of the lesion with a clear zone between limbus and lesion and no or minimal AC reaction. Often seen 2ndary to staph overgrowth from blethparitis.
What is prescribed to treat Marginal Keratitis?
DOC: Zylet Ophthalmic suspension; 5ml; instill 1 drop in eye every 2 hours for 2 days, then 4 times daily for 5 days; no refills; SHAKE WELL PRIOR TO EACH USE
DOC generic: 0.3% tobramycin/0.1%dexamethasone ophthalmic suspension; 2.5ml; instill 1 drop in eye every 2 hours for 2 days, then 4 times daily for 5 days; no refills; SHAKE WELL PRIOR TO EACH USE
What are the other management issues for Marginal keratitis?
Suggest Lid hygiene
No need for follow up, unless monitor compliance on lid hygiene and measure IOP
What are some soap-based lid hygiene products?
OcuSoft Original Scrubs/OcuSoft Foam Cleanser (Soaps only)
OcuSoft Plus Lid Scrubs/OcuSoft Plus Foam Cleanser (Soaps + Disinfectant)
SteriLid by TheraTears: Linalool is active ingredient= plain oil with antibacterial prop
MediViz & MediViz with Tea Tree Oil (not good for sensitive skin)
What are some lid hygiene with medicinal-based products?
Avenova
Heyedrate
OcuSoft HypoChlor
Bruder Hygienic Eyelid Solution
What do the medicinal-based lid hygiene products contain?
All contain various concentrations of Hypochlorous acid (HOCl), which has a high kill rate across Staphy aureus, Staph epidermidis, MRSA, and some demodex.
What are the safety and formulation advantages of hypochlorous acid lid & lash solutions?
No additives or preservatives. Can be safely used for daily, long-term lid hygiene.
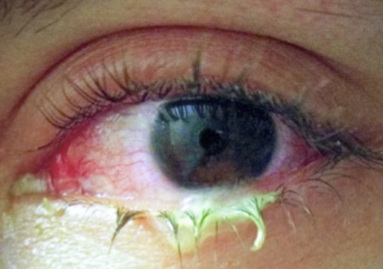
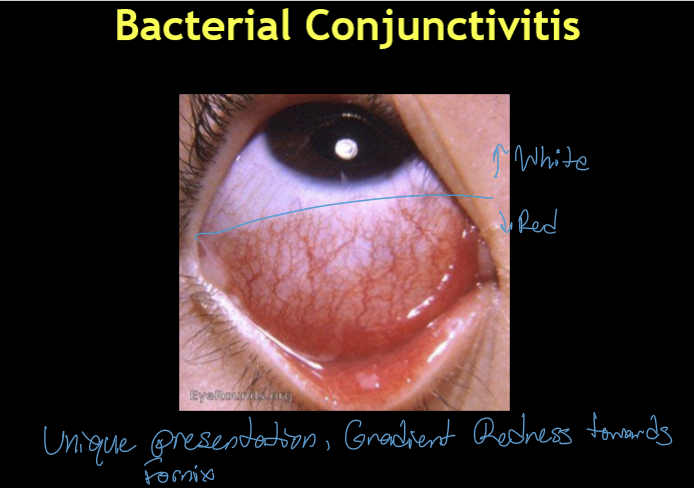
What is the illness script for bacterial conjunctivitis?
Epidemiology: pts of any age with no predilection for gender
Temp pattern: actue
Syndrome statement: Unilateral red eye with symptoms of burning and FB sensation. Often has a meaty redness that is often worse in the inferior portion of the bulbar conj and has palpebral conj infection and papilla. Mucopurulent discharge is a pathognomonic sign which may cause pts to complain of waking up with their eyelids stuck shut and/or intermittent blur
What can be prescribed to treat bacterial conjunctivitis?
DOC: tobramycin 0.3% ophthalmic solution; 5 mL, instill 1 drop in eye 4 times daily for 7 days; no refills
DOC: polytrim ophthalmic solution; 10 mL; instill 1 drop in eye every 3 hours for 7 days; no refills
What are the additional management considerations for patients with bacterial conjunctivitis?
Children: Prefer ointment (↑ contact time, easier administration)
Hygiene: Wash hands; change pillowcases/towels to prevent autoinoculation and spread
Contact lens wear:
Resume CL wear ≥48 hours after completing antibiotics AND symptom‑free (white and pain free)
No routine follow‑up needed if uncomplicated and improving
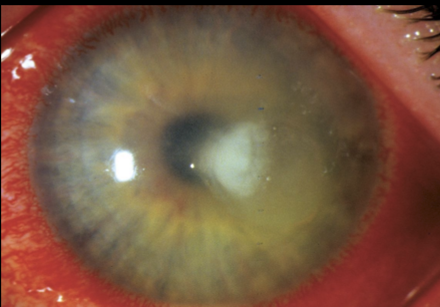
What are the treatments for Microbial keratitis
Need to cover major offenders: Staph, Pseudomonas for CL, H flue, MRSA for community acquired
Daytime Rx#1: Besivance 0.6% Ophthalmic suspension; 5mL; instill 1 drop every 5 minutes for 5 doses, then 1 drop q30 min for 6 hours, then 1 drop every hour until instructed otherwise (wake up every hour); No refills; SHAKE WELL BEFORE USE
Daytime Rx#2: Polytrim Ophthalmic solution; 10mL; instill 1 drop every hour until instructed otherwise; No refills
Nighttime Rx: Tobramycin 0.3% ophthalmic Ung; 3.5g; instill 1/4” strip in eye inside lower eyelide before bed until instructed otherwise; no refills
What are the treatments for staph overgrowth?
DOC: Doxycycline 100mg monohydrate tablets; 30 tabs; take 1 tablet by mouth every morning for 30 days; 3 refills; DO NOT LAY DOWN AFTER TAKING MEDS
Alternative: azithromycin 500mg tablets; 6 tabs; take 2 tabs by mouth once weekly for 3 weeks; 3 refills
What are the additional management for staph overgrowth patients?
Need sustained lid hygiene. No follow up is required. If adequate relief is not obtained from antibiotics and lid hygiene, additional options to consider are:
Assess for Demodex
Debridement of Line of Marx
BlephEx
Therapeutic Gland Expression:
Arita Expresser
LipiFlow
MIBO Thermoflo
iLux
TearCare
Intense Pulse Light Therapy