Abnormal Morphology of RBCs
1/37
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
38 Terms
Anisocytosis
variations in cell size
normal RDW < 15
normocytosis < 10% variation
quantitated as: 1+, 2+, 3+, or 4+
slight, moderate, marked
poikilocytosis
variations in cell shape
quantitate as:
slight, moderate, marked
1+, 5-10/hpf
2+, 10-20/hpf
3+, >20/hpf
anisochromia
variations in cell color
reflects hemoglobin concentration
central pallor - should be approx the diameter of cytoplasmic staining
other variations in cell morphology
cell inclusions
variations in erythrocyte distribution
normocyte
diameter: 6-8 um
average = 7 um
Anuclear
Biconcave, discoid
central pallor - equal to diameter of stained area
MCV = 80-96 fl
MCH = 27 - 32 pg
MCHC = 32-36%
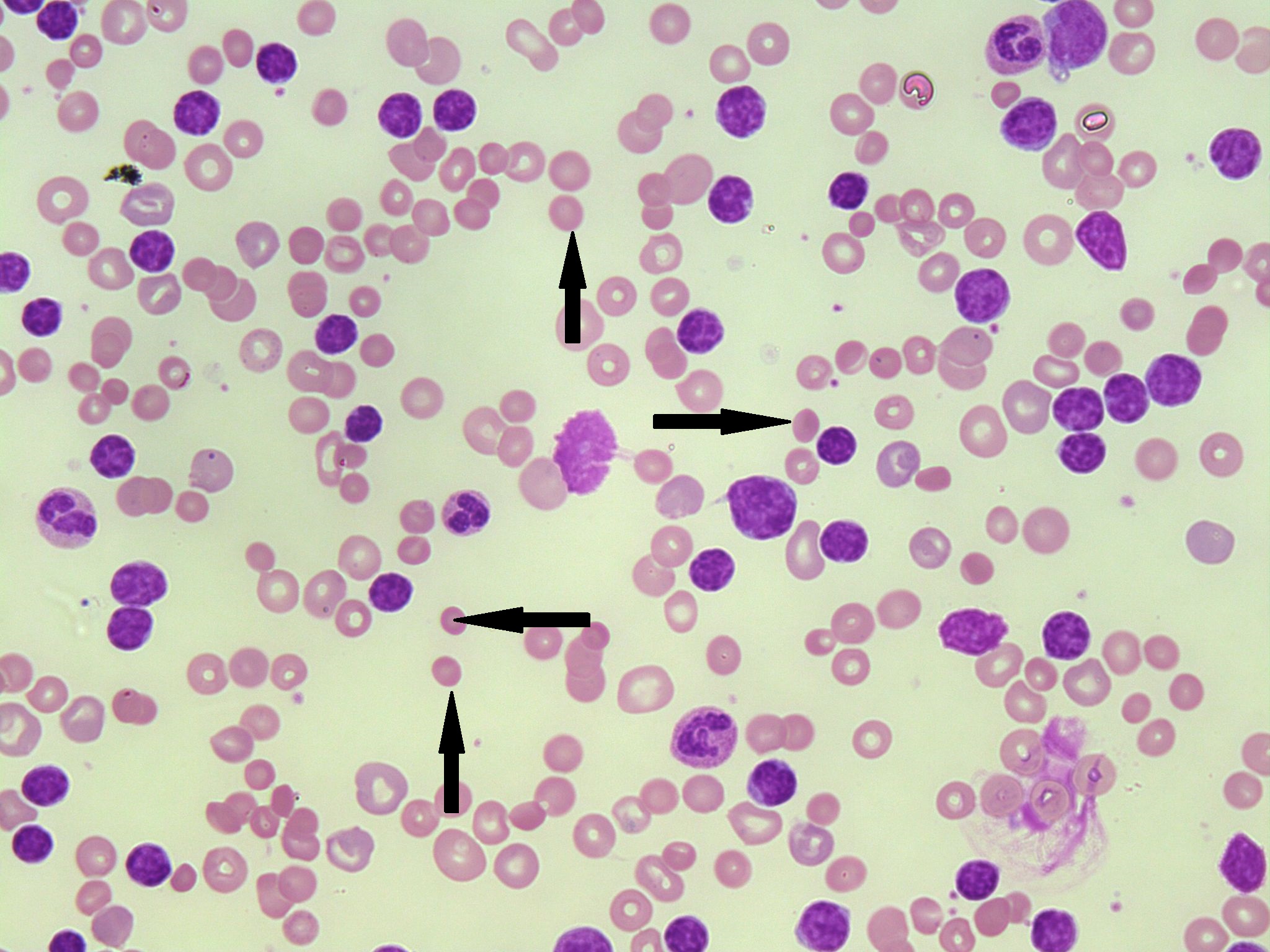
microcyte
Diameter < 6.0 um
MCV < 80 fl
MCH < 26 pg
increased central pallor
quantitated: slight, moderate, many
clinical significance: decreased Hb synthesis, Fe deficiency anemia-IDA, Thalassemia, anemia of chronic disease (ACD), sideroblastic anemia, lead poisoning
macrocyte
diameter is greater than 8.0 um
MCV > 96-100 fl
MCH > 32 pg
clinical implications:
defect in nuclear/DNA maturation
B12 deficiency
Folic acid deficiency
liver disease
obstructive jaundice
alcoholism
chemotherapy
reticulocytosis, erythropoiesis
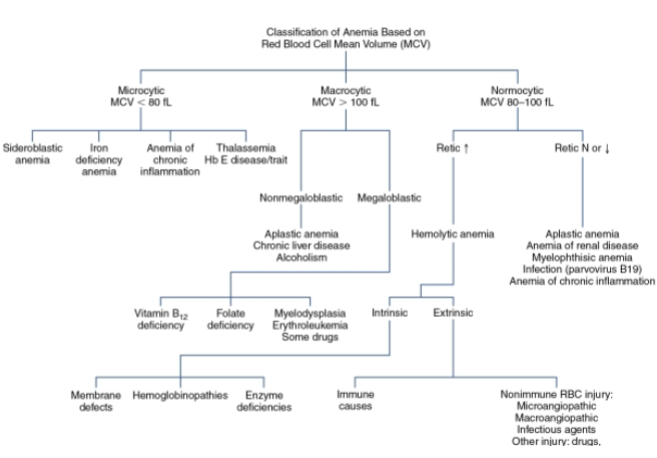
classification of anemia based on RBC MCV
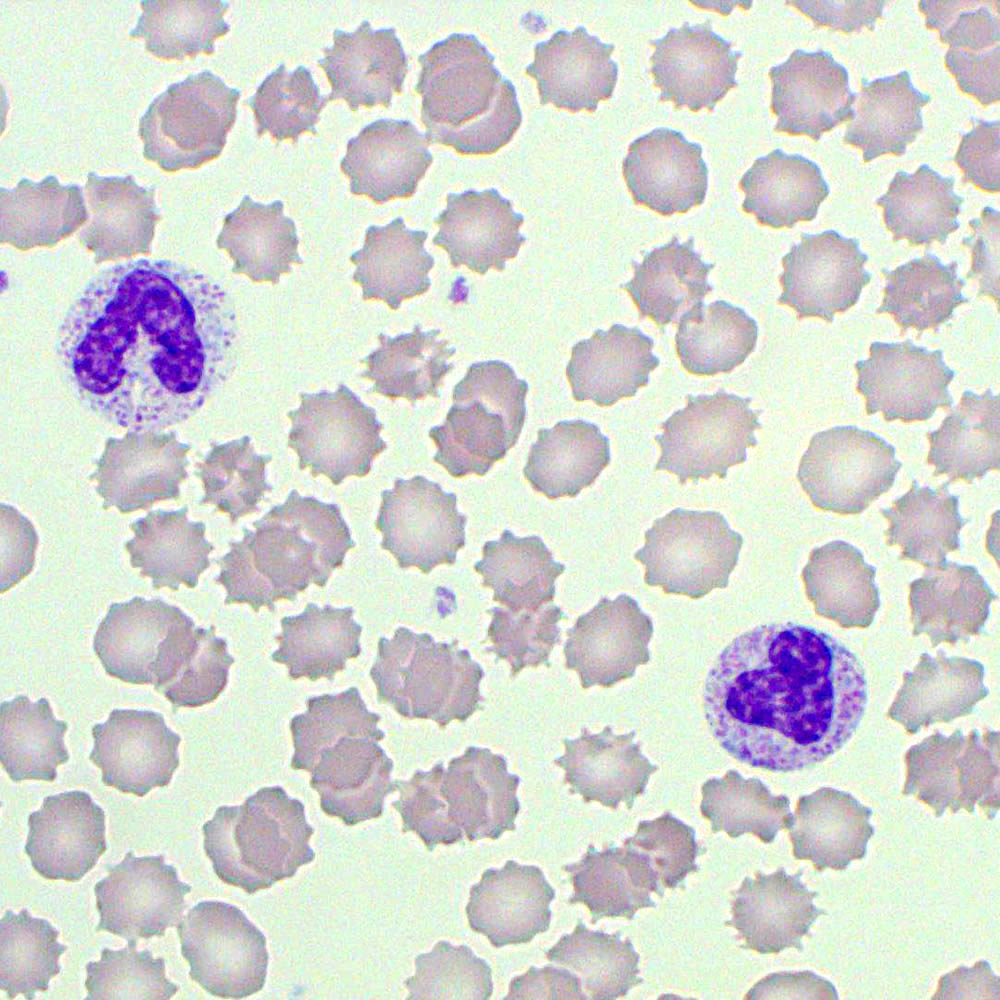
echinocytes
Crenated RBCs, Burr Cells
Short projections
Evenly spaced
Defects:
Depletion of ATP
Osmotic imbalances, physiologic loss of water
Prolonged exposure to anticoagulant
Clinical Implication:
Uremia
Chronic Renal disease
Liver disease (Cirrhosis, Hepatitis)
Renal failure
Hypothyroidism, burns
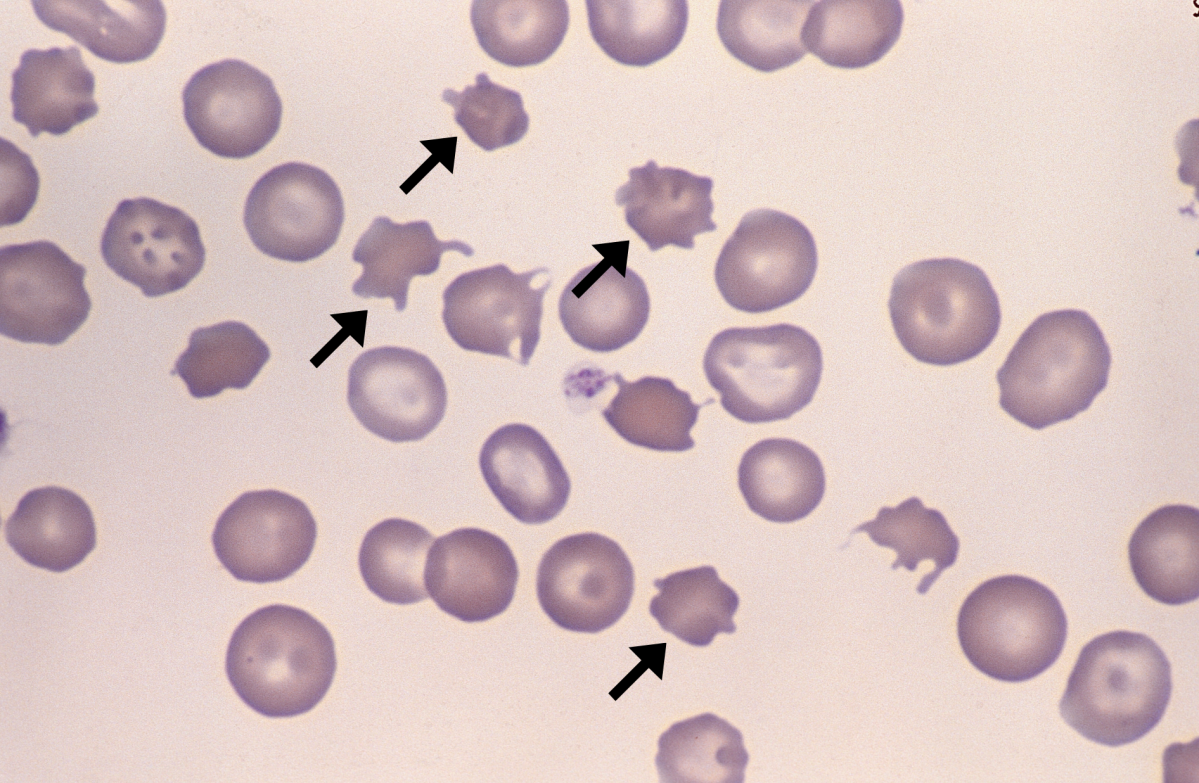
Acanthocytes
THORN, SPUR CELL
Irregular spines protruding from RBC
surface
Unevenly placed
Decrease in cell volume
Results:
Alterations in membrane lipid content
Loss of membrane integrity
High cholesterol to phospholipid ratio
Clinical Implications:
Abetalipoproteinemia
Liver disease
Hemolytic anemia, post-splenectomy
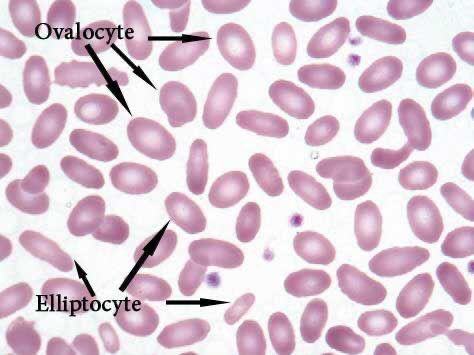
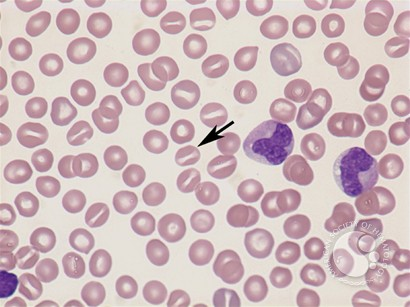
Elliptocytes/Ovalocytes
Elongated RBCs
Rod or Cigar-Shaped
Narrower than
ovalocytes
Membrane defect in
spectrin and protein
4.1
Normocytic
Clinical Association:
Hereditary elliptocytosis
Thalassemia
Fe Deficiency anemia
Egg-Shaped or oval-shaped
Bipolar aggregates of Hb
Normocytic or macrocytic
Normochromic or
hypochromic
Cause: Reduced ATP and
2,3 DPG
Clinical Association:
Megaloblastic anemia (macro sized ovalocytes)
Myelodylsplastic syndromes
Thalassemia (normocytic ovalocytes seen)
target cells/codocytes
flattened RBC
Hb concentration at center and periphery of cell
Resembles archery target
Membrane defect: excess membrane cholesterol and phospholipid, decreased Hb
implications:
hemoglobinopathies - Hb C, Hb S, Hb SC
thalassemia
iron deficiency anemia
liver disease, obstructive jaundice
post-splenectomy
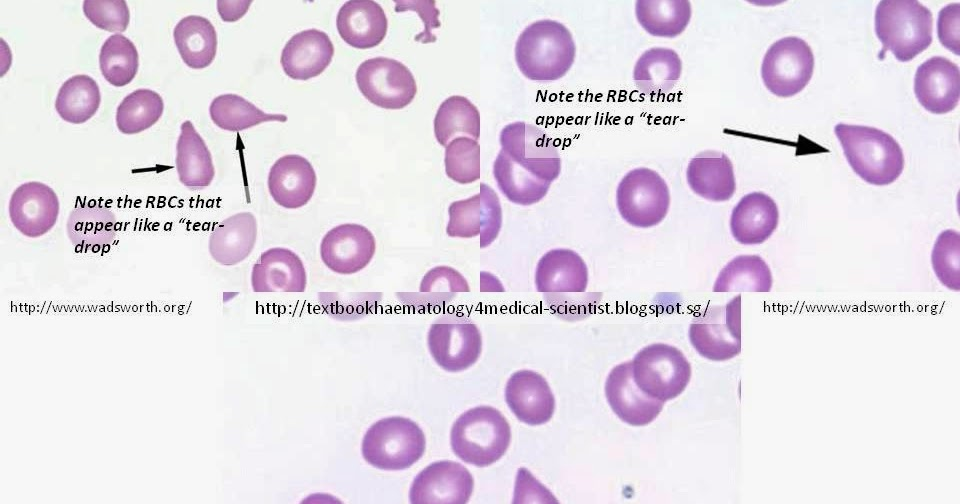
dacrocytes, tear drop cells
teardrop- pear shaped
rounded on one end
pointed on the other
results from squeezing during splenic passage
clinical significance:
primary myelofibrosis (PM)
B12 and folate deficiency
ineffective erythropoiesis
thalassemia
stomatocytes
Round RBC
Elongated, mouth-like central pallor.
Caused by abnormally increased cation influx results in
increased permeability to sodium.
Asymmetric increase in passive Na+ and K+
permeability
Influx of Na+ exceeds the loss of K+
Causing a net influx of water, overhydration, and
swelling
Clinical Implications:
Hereditary Stomatocytosis
Acute Alcoholism
Rh Null disease
Liver disease, cirrhosis
Glutathione deficiency
Lead poisoning
Artifact
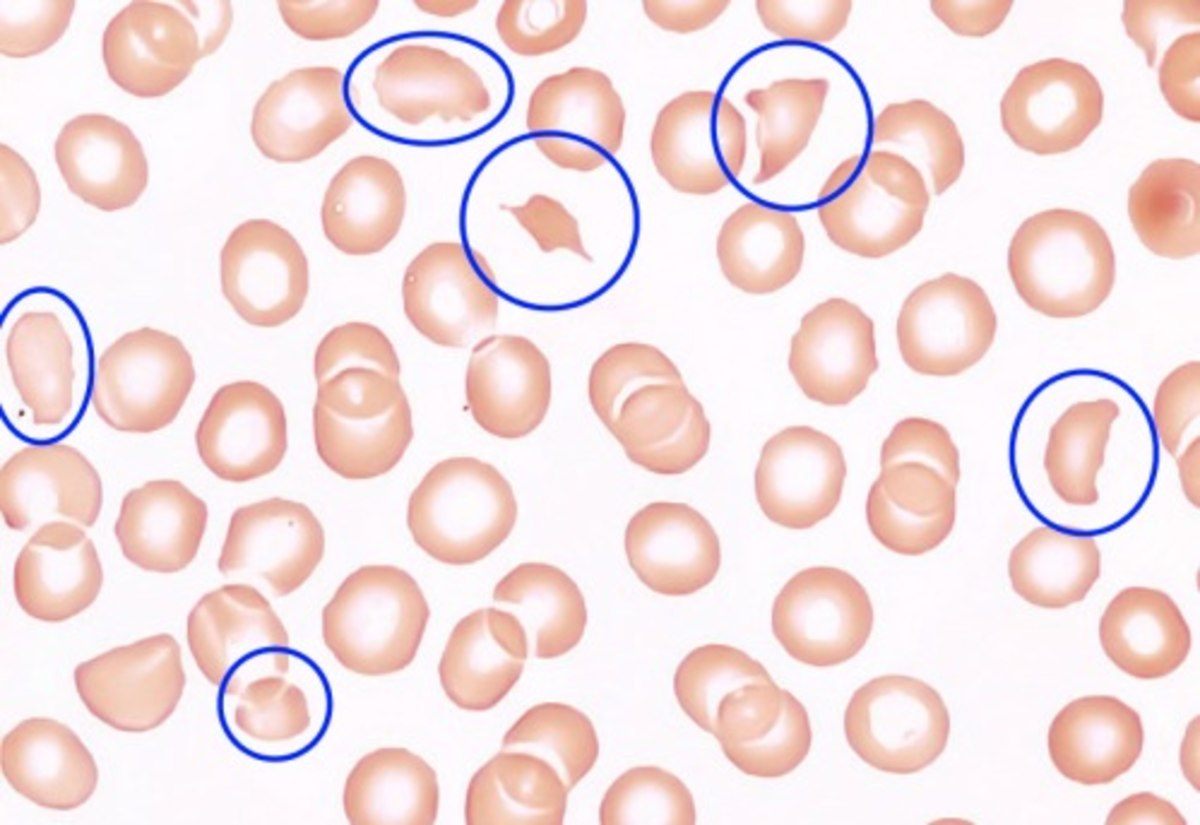
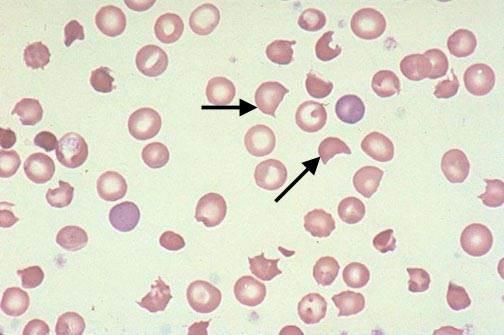
schistocytes
RBC Fragments
Due to membrane damage
Clinical Implications:
Disseminated intravascular Coagulation (DIC)
G6PD deficiency
Hemolytic anemias
Hemolytic uremic syndrome (HUS)
Micro-angiopathic hemolytic anemia
Prostheitc heart valves
Burn patients
ABO/RH incompatibility
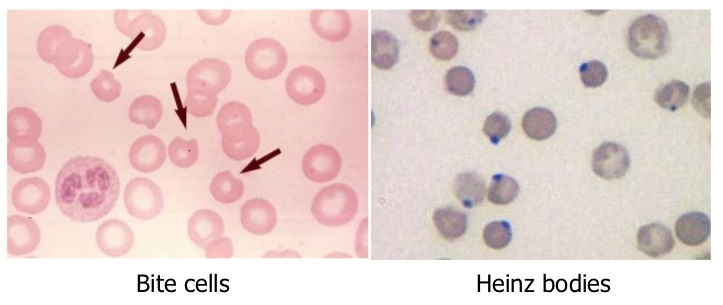
bite cells
spheroid RBC with “bite-like” missing membrane
clinical implications: G-6-PD deficiency, hemolytic episodes, hemoglobinopathies
helmet cells, keratocytes
form of schistocytes
helmut shaped
implications - DIC, hemolytic anemia
spherocytes
Very spheroid,
Smaller in diameter
Loss of biconcavity, no central pallor
Genetic Membrane defect
Defect in Spectrin assembly
Poor Protein 4.1 to spectrin binding
Actin-spectrin band 3 complex defect
Results in defective cytoskeleton
Higher concentration of hemoglobin per cell
Increased MCHC > 36%
Clinical Implications:
Hereditary spherocytosis
Immune Hemolytic anemia (Acute & chronic Extravascular)
pseudo-spherocytes)
Severe burns
Post Splenectomy
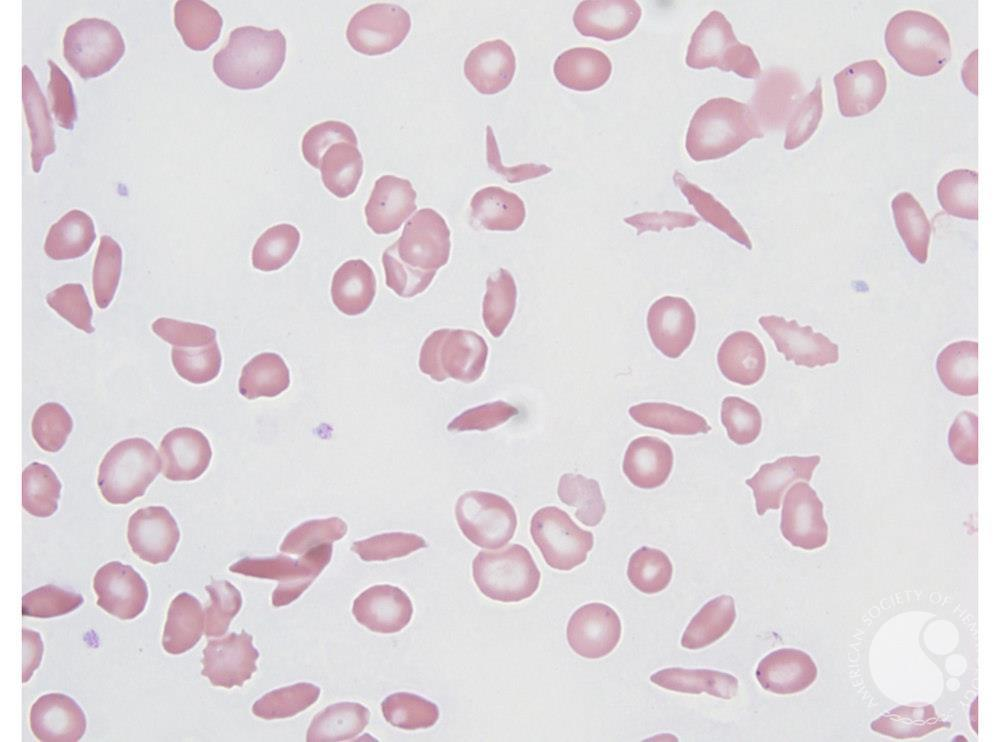
drepanocytes
SICKLE CELLS
Elongated RBCs
Point projections on either end
Cell may be straight or curved
Presence of Hb S
Produces a hemoglobin that crystalizes under low oxygen
tension conditions.
Clinical Implications:
Sickle cell anemia (disease or trait)
Hb C/S disease
Confirm by Dithionite solubility
Hb electrophoresis
normochromic
Hb is normal
MCH is normal
MCHC is normal
Good central pallor
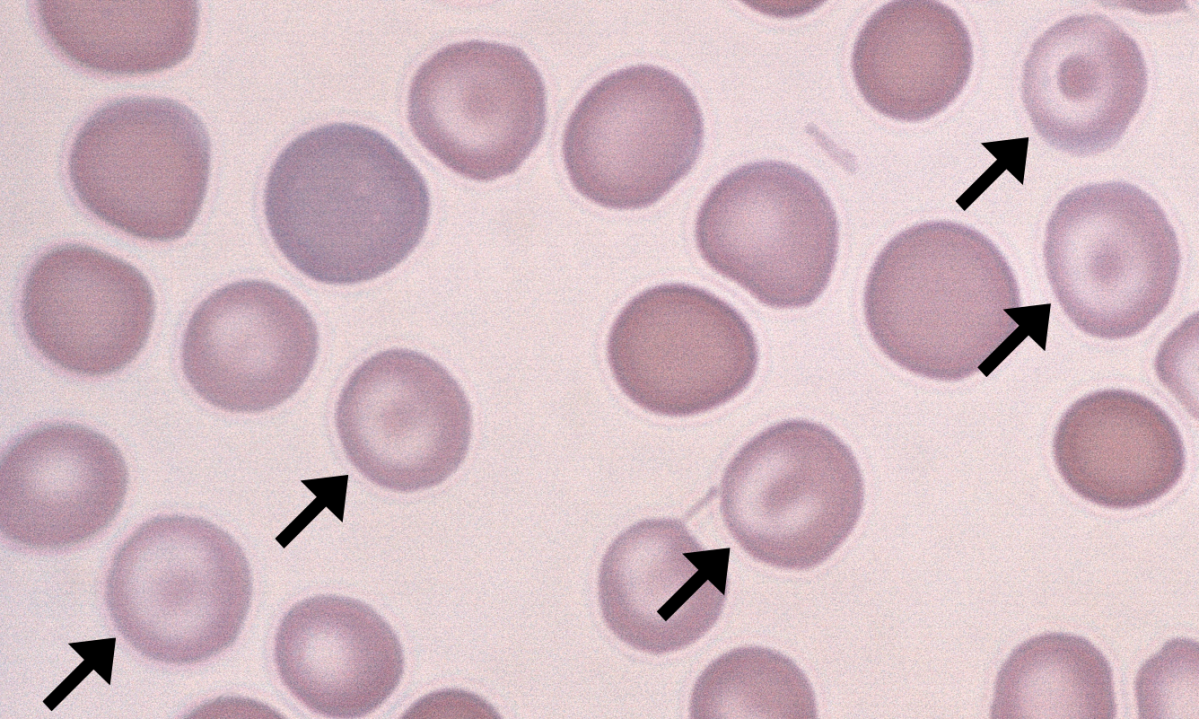
hypochromic
decreased Hb
decreased MCH
decreased MCHC
increased central pallor
clinical indications:
Fe deficiency anemia, thalassemia, anemia of chronic disease (ACD), lead poisoning, sideroblastic anemia
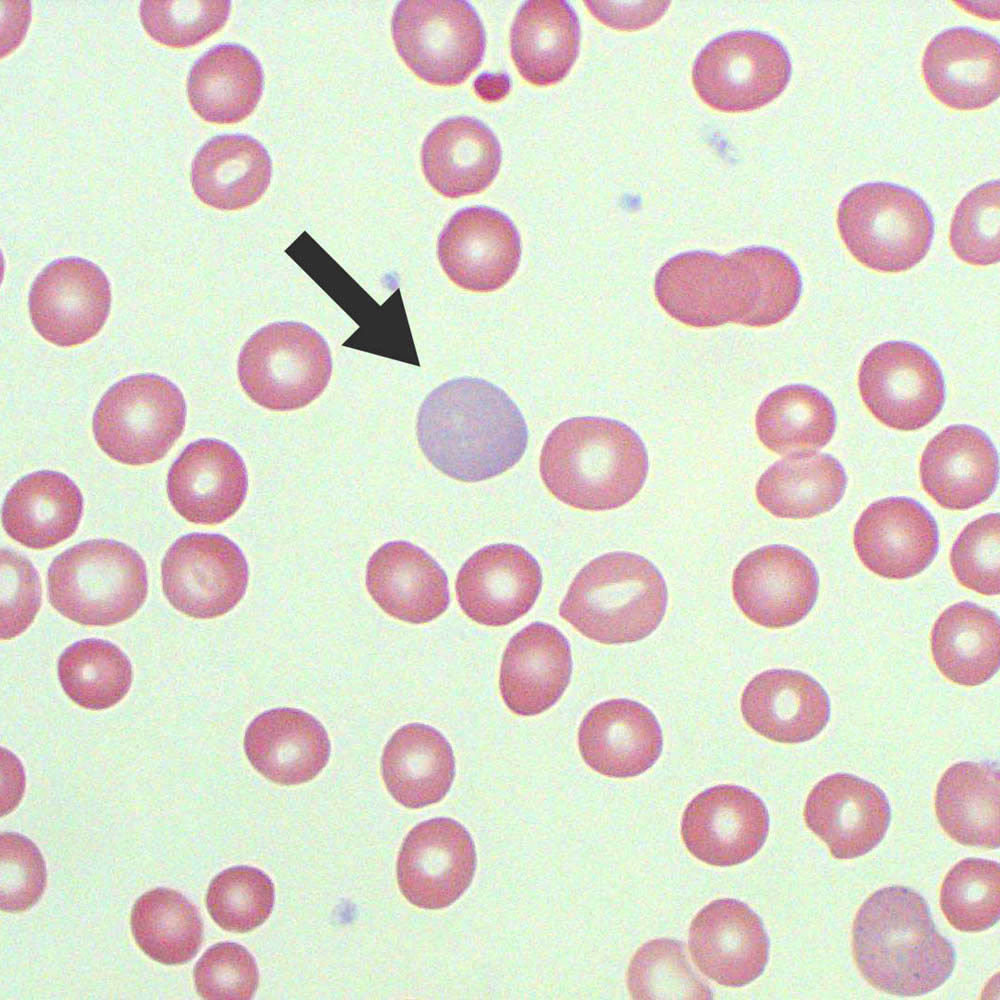
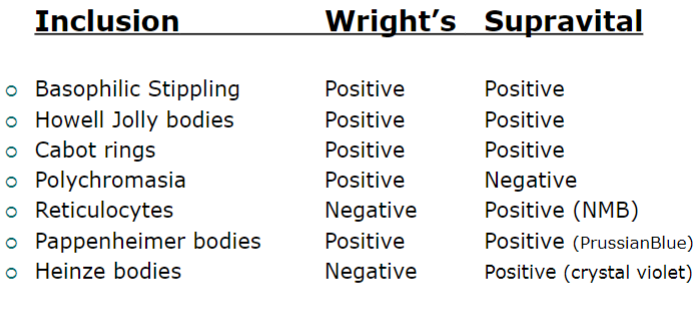
polychromatophilia
polychromasia
wright’s stain
increase in diffuse basophilic RBCs
cells are slightly immature
results from diffuse RNA
supravital stain, reticulocyte
quantitate as:
1+, 1-3/hpf
2+, 3-7/hpf
3+, >7/hpf
clinical significance of polychromasia
Increased Polychromasia:
Increased erythropoiesis
Increased bone marrow production
Associated with:
Physiologic correction for Anemia
Hemolytic anemia
Response to treatment
Not elevated in:
untreated Fe deficiency or B12 Deficiency
anemia
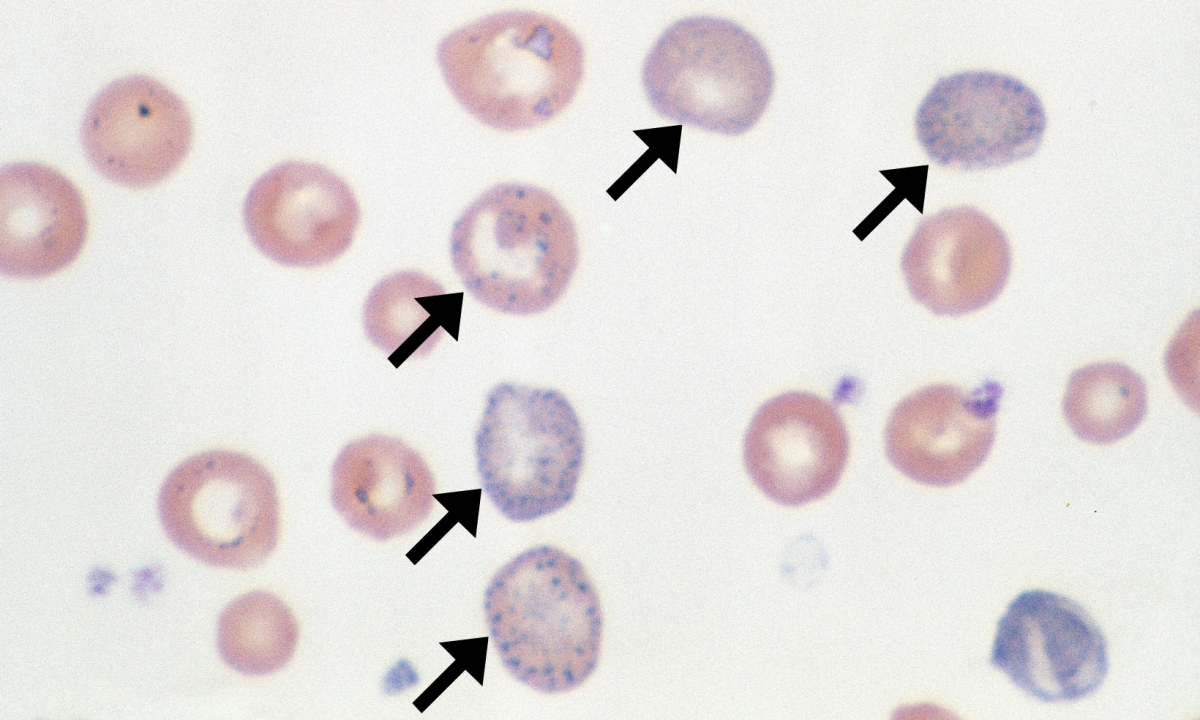
basophilic stippling
Coarse granulation
RNA and ribosome/mitochondrial aggregates
Even distribution throughout RBC
Visualized with Wright’s stain and Supravital stains
Clinical Implications:
Lead Intoxication
Heavy metal poisoning
Thalassemia
Severe anemia
Accelerated erythropoiesis
Quantitate as: slight, moderate, marked
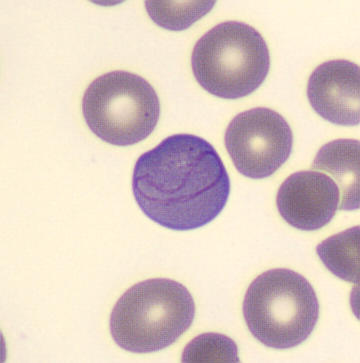
cabot rings
Thread-like rings
Loops or figure eights
Single or Multiple rings
Residual nuclear membrane or mitotic
spindle
Visible with Wright’s stain
Implications:
Severe anemia
Pernicious anemia (B12 deficiency)
Lead Intoxication
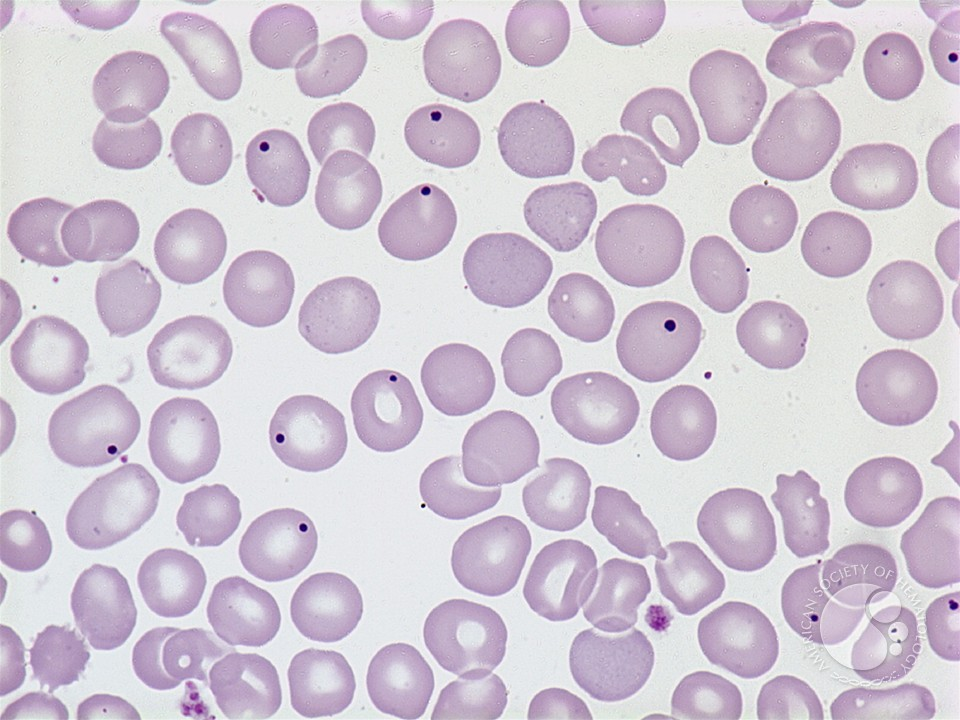
howell jolly bodies
small, round, dark blue- purple masses
eccentric
nuclear DNA remnants
visible with wrights stain
cells may contain 1-2 HJ bodies
implications:
pernicious anemia
hemolytic anemia
sickle cell anemia
post splenectomy
thalassemia
alcoholism
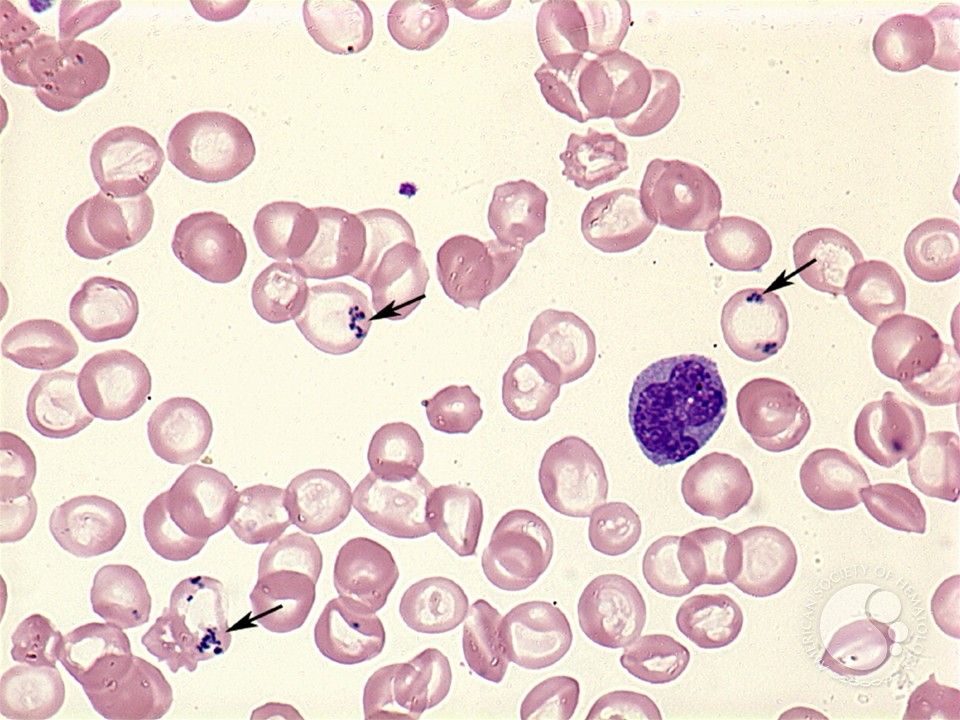
pappenheimer bodies
small blue granules
clusters of free iron. non-heme iron
near the periphery of RBC
visible with wright’s stain and prussian blue
confirm with prussian blue stain - stains iron, siderotic granules
clinical implications - sideroblastic anemia, severe hemolytic anemia, thalassemia, post splenectomy, B12, folate defic, sickle cell anemia
siderodic granules
when stained with Prussian blue
if granules are in non-nucleated cell - siderocyte
if granules are in NRBC - ringed sideroblast
malarial pigments
schuffner’s granules
granular pigments appearing in RBC’s parasitized by Plasmodium spp
fine red to pink granules
Plasmodium. Vivax and P. ovale infection
P. falciparum and P. malaria are neg
Visible with Wrigh’ts stain
Mauer’s dots - P. falciparum and larger wedge shaped granules
Schuffner’s granules
P. vviax and P. ovale

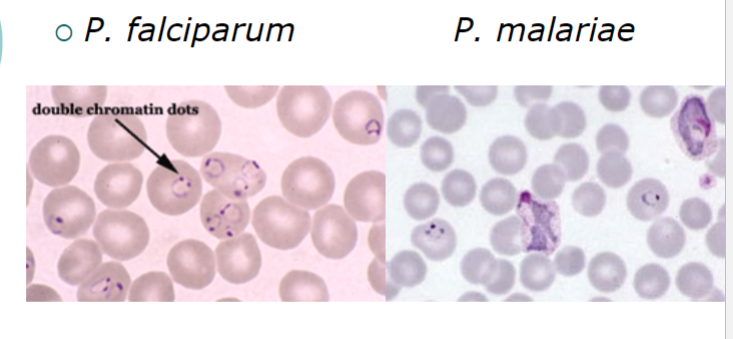
Parasite rings
P. falciparum and P. malariae
Heinz Bodies
Precipitated, denatured, unstable
Hemoglobin
Visible with Supra vital stains
Crystal violet
Not visible with Wright’s stain
Implications:
(G6PD) deficiency
Glucose-6-phosphate dehydrogenase
Drug induced or food induced
Unstable hemoglobin
Alpha Thalassemia
Hb-H, Barts, I
In G6PD deficiency
G6PD protects Hb from oxidation
Globin chains are denatured
Forming Heinze bodies
Heinze bodies attach to cell membrane
induce membrane damage
Bite cells and Schistocytes may be seen
Alpha thalassemia: Presence of Hb-H (B4)
Favism
A potential fatal hemolytic episodes
following ingestion of fava beans
associated with G6PD deficiency
causes oxidation of unstable hemoglobin
appearance of bite cells
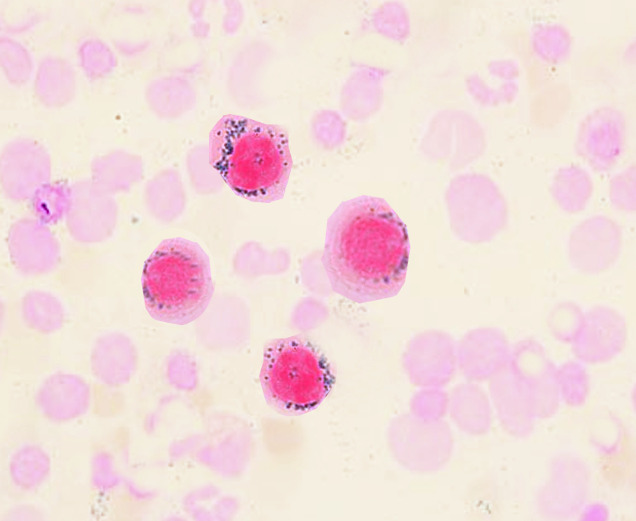
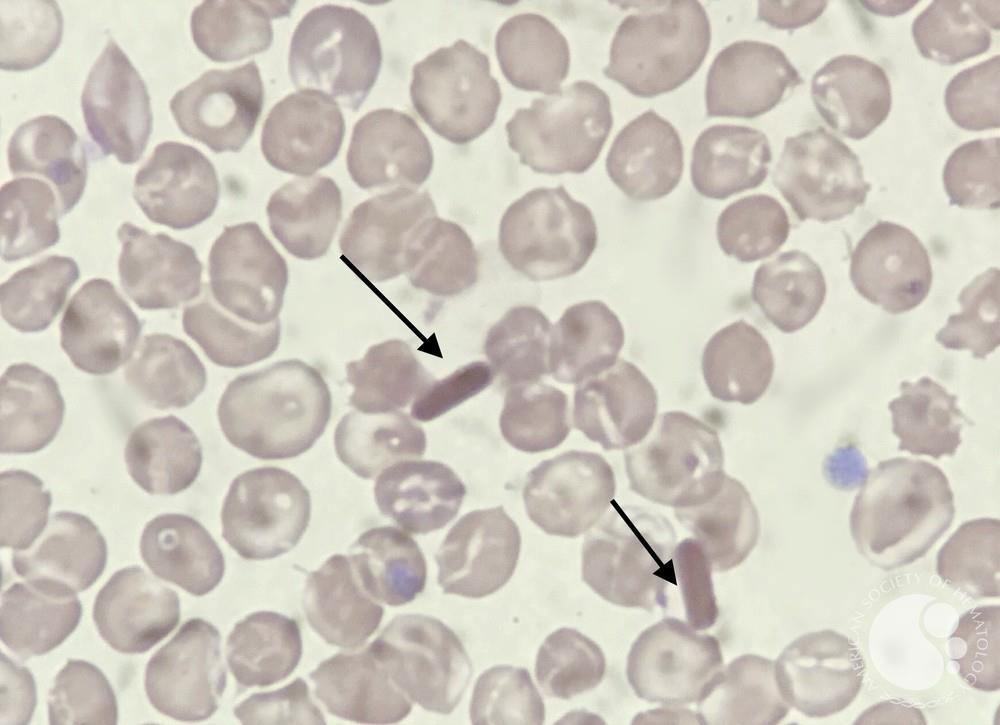
Hemoglobin C crystals
Intra erythrocyte crystals
Oblong hexagonal crystals
Insoluble Hb-C
Crystals are visible with Wright’s stain
Implications:
Hemoglobin CC, SC, CA disease
Staining characteristics in RBCs
Agglutination
Aggregates or clumps
Antibody induced
Clinical Indicates:
Cold agglutinins
Autoimmune Hemolytic anemia
Mycoplasma pneumoniae infections
Falsely affects electronic cell counting:
Decreases RBC count
Increases MCV
Corrected by warming the specimen @ 37 C for 15
minutes.
Rouleaux
stacking of RBCs
Increased plasma proteins
decreased zeta potential - natural repulsion mechanism
creates the stack of coins effects
examine on “high dry” or 40x
clinical association - multiple myeloma
quantitate as - slight, moderate, marked
